.png)
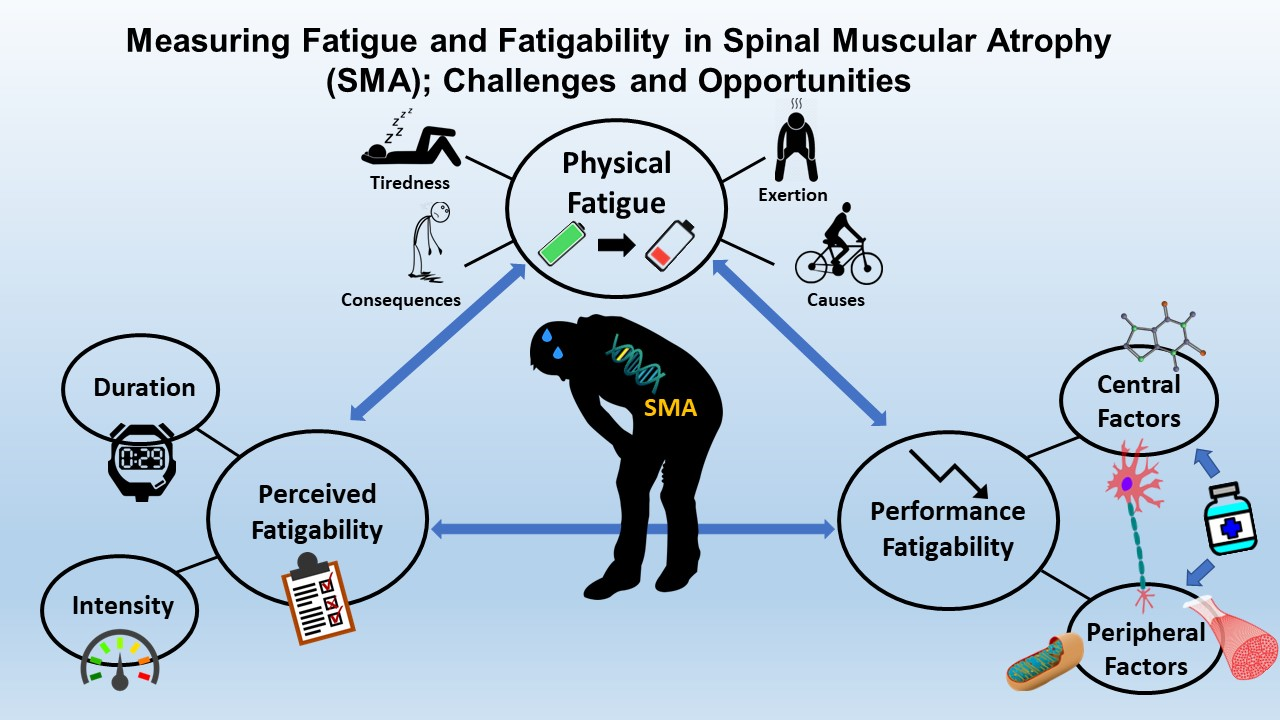
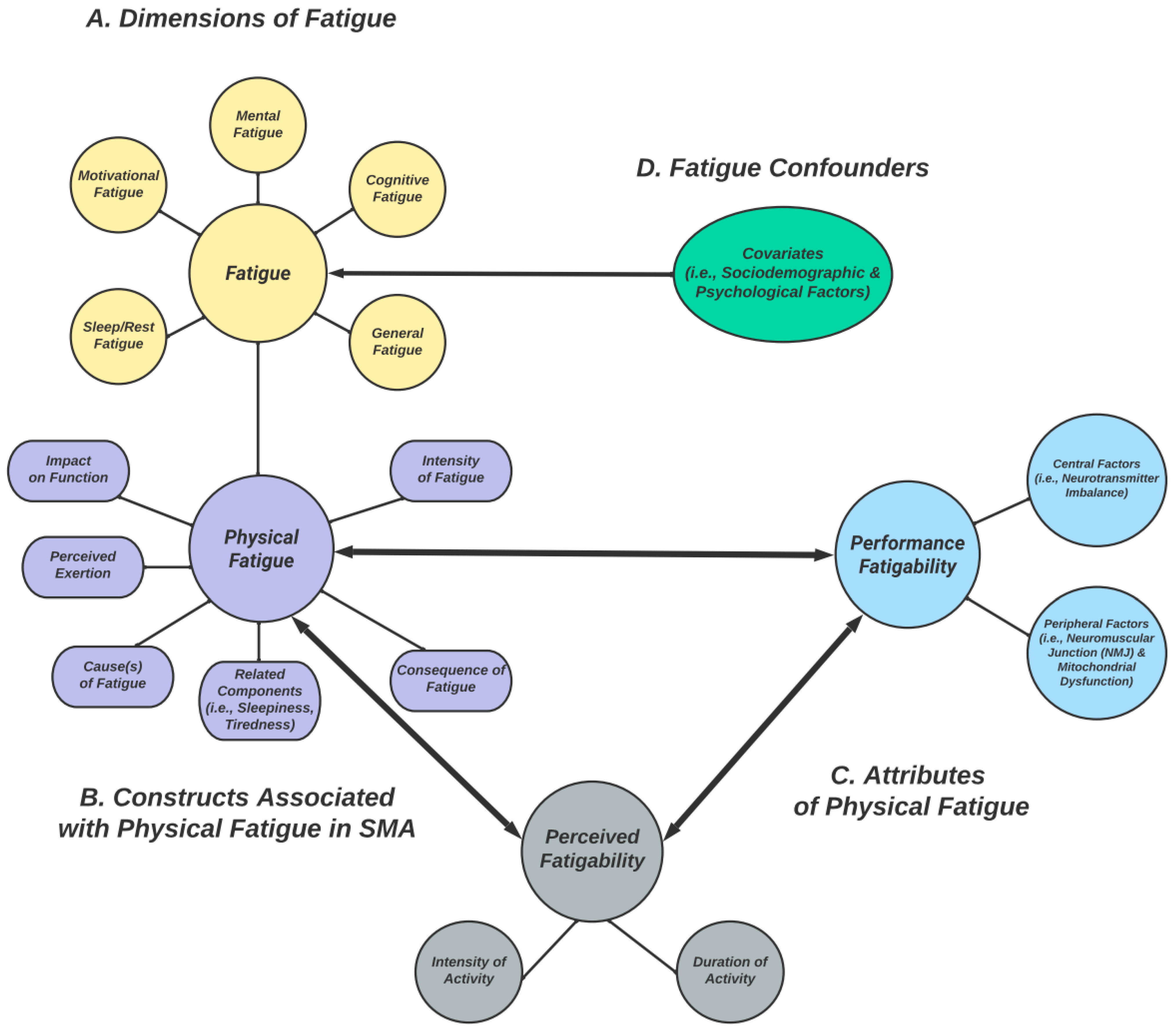
Measuring Fatigue and Fatigability in Spinal Muscular Atrophy (SMA): Challenges and Opportunities

 , ,
, ,  , ,
, ,  and
and Abstract

{kind=link}
{kind=link}
Share and Cite
Rodriguez-Torres, R.S.; Uher, D.; Gay, E.L.; Coratti, G.; Dunaway Young, S.; Rohwer, A.; Muni Lofra, R.; De Vivo, D.C.; Hirano, M.; Glynn, N.W.; et al. Measuring Fatigue and Fatigability in Spinal Muscular Atrophy (SMA): Challenges and Opportunities. J. Clin. Med. 2023, 12, 3458. https://doi.org/10.3390/jcm12103458
Rodriguez-Torres RS, Uher D, Gay EL, Coratti G, Dunaway Young S, Rohwer A, Muni Lofra R, De Vivo DC, Hirano M, Glynn NW, et al. Measuring Fatigue and Fatigability in Spinal Muscular Atrophy (SMA): Challenges and Opportunities. Journal of Clinical Medicine. 2023; 12(10):3458. https://doi.org/10.3390/jcm12103458
Chicago/Turabian StyleRodriguez-Torres, Rafael S., David Uher, Emma L. Gay, Giorgia Coratti, Sally Dunaway Young, Annemarie Rohwer, Robert Muni Lofra, Darryl C. De Vivo, Michio Hirano, Nancy W. Glynn, and et al. 2023. "Measuring Fatigue and Fatigability in Spinal Muscular Atrophy (SMA): Challenges and Opportunities" Journal of Clinical Medicine 12, no. 10: 3458. https://doi.org/10.3390/jcm12103458
APA StyleRodriguez-Torres, R. S., Uher, D., Gay, E. L., Coratti, G., Dunaway Young, S., Rohwer, A., Muni Lofra, R., De Vivo, D. C., Hirano, M., Glynn, N. W., & Montes, J. (2023). Measuring Fatigue and Fatigability in Spinal Muscular Atrophy (SMA): Challenges and Opportunities. Journal of Clinical Medicine, 12(10), 3458. https://doi.org/10.3390/jcm12103458