


VISCERAL SENSITIVITY INDEX (VSI-IT): Italian Adaptation and Validation

 ,
,  ,
, 
 , , ,
, , ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Instruments
2.3.1. VSI
2.3.2. MAIA
- Noticing: awareness of uncomfortable, comfortable, and neutral bodily sensations.
- Not distracting: tendency to ignore or distract oneself from sensations of pain or discomfort.
- Not worrying: emotional distress or worry associated with sensations of pain or discomfort.
- Attention regulation: the ability to sustain and control attention to bodily sensations.
- Emotional awareness: awareness of the connection between bodily sensations and emotional states.
- Self-regulation: the ability to regulate psychological discomfort through attention to bodily sensations.
- Body listening: active listening to the body for understanding.
- Trusting: experiencing one’s own body as safe and reliable.
2.4. Statistical Analysis
3. Results
3.1. Factor Structure, Validity, and Reliability of VSI-IT
3.2. Sensitivity and Discriminant Validity of the VSI-IT
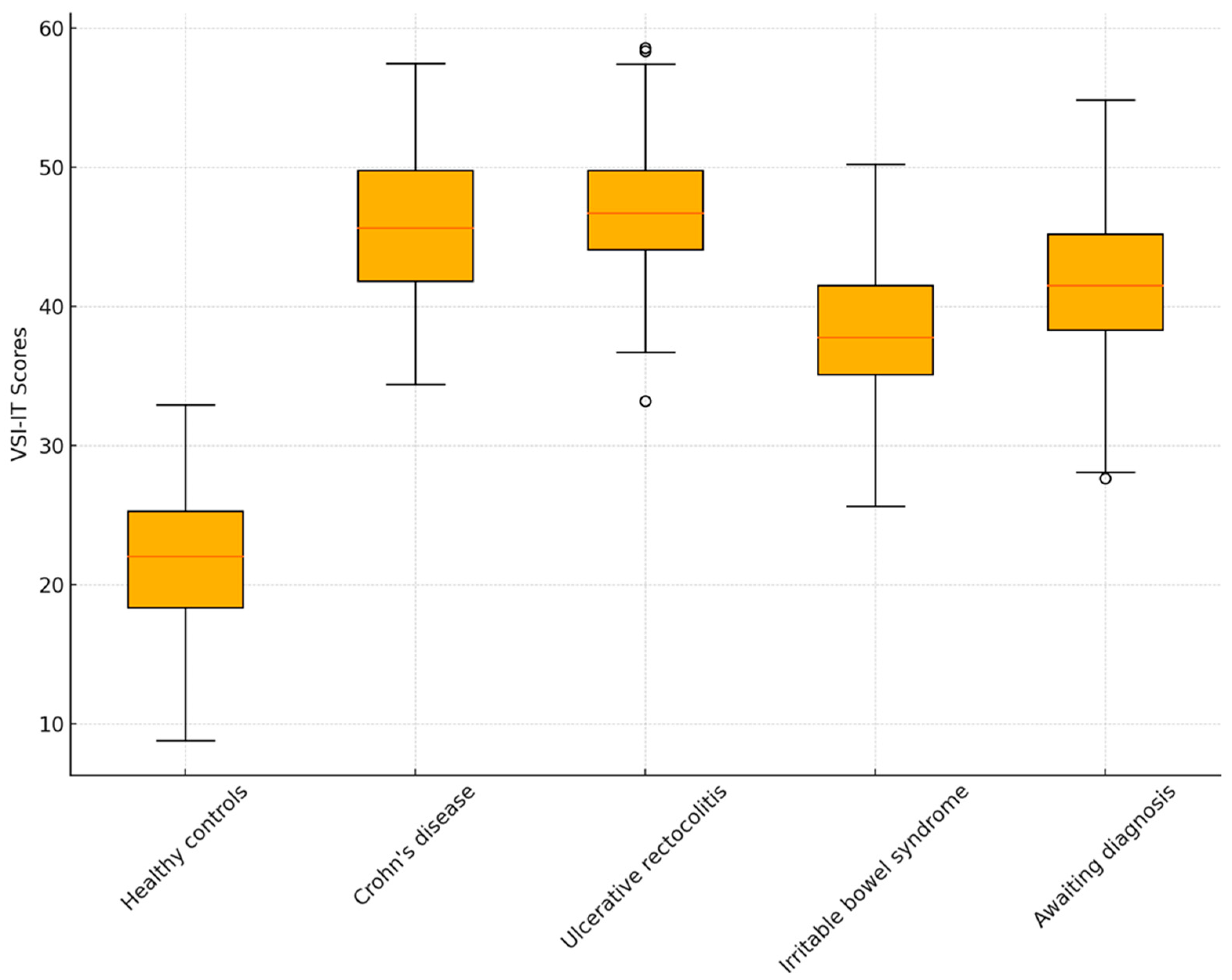
3.2.1. The Ability of the VSI-IT to Discriminate between Pathological Conditions
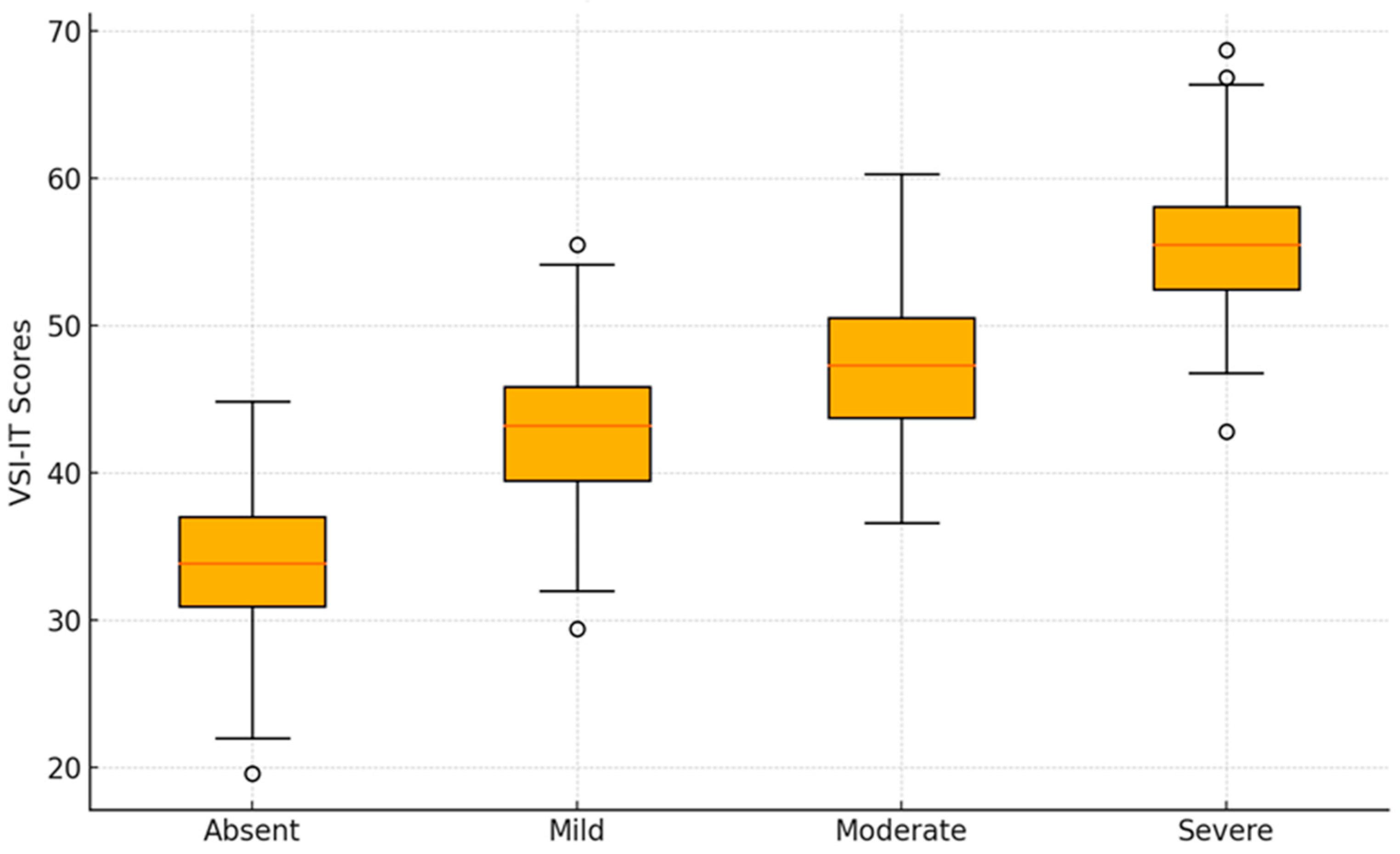
3.2.2. The Ability of the VSI-IT to Discriminate Based on the Severity of Symptoms
3.3. Concurrent Validity of VSI-IT
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Pienamente d’accordo | D’accordo | Parzialmente d’accordo | Parzialmente in disaccordo | In disaccordo | Fortemente in disaccordo | |
| 1. Temo che ogni volta che mangio durante il giorno, il gonfiore e la distensione della pancia peggioreranno. | □ | □ | □ | □ | □ | □ |
| 2. Divento ansioso quando vado in un nuovo ristorante. | □ | □ | □ | □ | □ | □ |
| 3. Mi preoccupo spesso per problemi alla pancia. | □ | □ | □ | □ | □ | □ |
| 4. Ho difficoltà a divertirmi perché non riesco a distogliere la mente dal disagio della pancia. | □ | □ | □ | □ | □ | □ |
| 5. Spesso temo di non riuscire ad avere un normale movimento intestinale. | □ | □ | □ | □ | □ | □ |
| 6. A causa della paura di sviluppare disturbi addominali, raramente provo cibi nuovi. | □ | □ | □ | □ | □ | □ |
| 7. Qualunque cosa mangi, probabilmente mi sentirò a disagio. | □ | □ | □ | □ | □ | □ |
| 8. Non appena sento fastidio addominale comincio a preoccuparmi e a sentirmi ansioso. | □ | □ | □ | □ | □ | □ |
| 9. Quando entro in un posto dove non sono mai stato, una delle prime cose che faccio è cercare un bagno. | □ | □ | □ | □ | □ | □ |
| 10. Sono costantemente consapevole delle sensazioni che ho nella mia pancia. | □ | □ | □ | □ | □ | □ |
| 11. Sento spesso che il fastidio alla pancia potrebbe essere segno di una grave malattia. | □ | □ | □ | □ | □ | □ |
| 12. Non appena mi sveglio, temo che avrò fastidio alla pancia durante il giorno. | □ | □ | □ | □ | □ | □ |
| 13. Quando sento disagio nel mio ventre, mi spavento. | □ | □ | □ | □ | □ | □ |
| 14. In situazioni stressanti, la mia pancia mi dà molto fastidio. | □ | □ | □ | □ | □ | □ |
| 15. Penso costantemente a ciò che sta accadendo nella mia pancia. | □ | □ | □ | □ | □ | □ |
References
- Labus, J.S.; Bolus, R.; Chang, L.; Wiklund, I.; Naesdal, J.; Mayer, E.A.; Naliboff, B.D. The Visceral Sensitivity Index: Development and validation of a gastrointestinal symptom-specific anxiety scale. Aliment. Pharmacol. Ther. 2004, 20, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Trieschmann, K.; Chang, L.; Park, S.; Naliboff, B.; Joshi, S.; Labus, J.S.; Sauk, J.S.; Limketkai, B.N.; Mayer, E.A. The visceral sensitivity index: A novel tool for measuring GI-symptom-specific anxiety in inflammatory bowel disease. Neurogastroenterol. Motil. 2022, 34, e14384. [Google Scholar] [CrossRef] [PubMed]
- Caballero-Mateos, A.M. Gut Feelings: The Psychological Impact of Inflammatory Bowel Disease. J. Clin. Med. 2023, 12, 3867. [Google Scholar] [CrossRef] [PubMed]
- Lind, R.; Lied, G.A.; Lillestøl, K.; Valeur, J.; Berstad, A. Do psychological factors predict symptom severity in patients with subjective food hypersensitivity? Scand. J. Gastroenterol. 2010, 45, 835–843. [Google Scholar] [CrossRef]
- Saigo, T.; Tayama, J.; Hamaguchi, T.; Nakaya, N.; Tomiie, T.; Bernick, P.J.; Kanazawa, M.; Labus, J.S.; Naliboff, B.D.; Shirabe, S.; et al. Gastrointestinal specific anxiety in irritable bowel syndrome: Validation of the Japanese version of the visceral sensitivity index for university students. BioPsychoSocial Med. 2014, 8, 1–9. [Google Scholar] [CrossRef]
- Neverovskyi, A.; Shypulin, V.; Mikhnova, N. Translation and validation of the Ukrainian version of the visceral sensitivity index for patients with irritable bowel syndrome. Prz. Gastroenterol. 2023, 18, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Davey, S.; Bell, E.; Halberstadt, J. Using targeted visceroception to improve interoceptive sensibility and emotion regulation. New Ideas Psychol. 2023, 68, 100989. [Google Scholar] [CrossRef]
- Calì, G.; Ambrosini, E.; Picconi, L.; Mehling, W.E.; Committeri, G. Investigating the relationship between interoceptive accuracy, interoceptive awareness, and emotional susceptibility. Front. Psychol. 2015, 6, 1202. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A.; Reilly, E.E.; Murray, H.B.; Perry, T.R.; Kaye, W.H.; Wierenga, C.E. Validating the visceral sensitivity index in an eating disorder sample. Int. J. Eat. Disord. 2021, 54, 986–994. [Google Scholar] [CrossRef]
- Hayes, B.; Burgell, R.; Apputhurai, P.; Garg, M.; Knowles, S.R. Extending the Common Sense Model to Explore the Impact of Visceral Sensitivity on Quality of Life in Inflammatory Bowel Disease. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2022, 33, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Larussa, T.; Abenavoli, L.; Corea, A.; Procopio, A.C.; Giubilei, L.; Vallelunga, R.; Polimeni, N.; Suraci, E.; Marasco, R.; Imeneo, M.; et al. Trends and characteristics associated with dietary triggers and psychological distress in patients with irritable bowel syndrome: A cross-sectional study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3752–3761. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, E.; Bergamaschi, W.; Russo, A.G. Population-based incidence and prevalence of inflammatory bowel diseases in Milan (Northern Italy), and estimates for Italy. Eur. J. Gastroenterol. Hepatol. 2021, 33, e383–e389. [Google Scholar] [CrossRef] [PubMed]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.L.; Nicholls, A.R.; Clough, P.J.; Crust, L. Assessing model fit: Caveats and recommendations for confirmatory factor analysis and exploratory structural equation modeling. Meas. Phys. Educ. Exerc. Sci. 2015, 19, 12–21. [Google Scholar] [CrossRef]
- Montoya, A.K.; Edwards, M.C. The poor fit of model fit for selecting number of factors in exploratory factor analysis for scale evaluation. Educ. Psychol. Meas. 2021, 81, 413–440. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.; Rizzo, A.; Muscatello, M.R.A.; Celebre, L.; Silvestri, M.C.; Zoccali, R.A.; Mento, C. Hyperarousal scale: Italian cultural validation, age and gender differences, in a nonclinical population. Int. J. Environ. Res. Public Health 2020, 17, 1176. [Google Scholar] [CrossRef] [PubMed]
- Fracas, E.; Constantino, A.; Vecchi, M.; Buoli, M. Depressive and Anxiety Disorders in Patients with Inflammatory Bowel Diseases: Are There Any Gender Differences? Int. J. Environ. Res. Public Health 2023, 20, 6255. [Google Scholar] [CrossRef]
- Labus, J.S.; Mayer, E.A.; Chang, L.; Bolus, R.; Naliboff, B.D. The central role of gastrointestinal-specific anxiety in irritable bowel syndrome: Further validation of the visceral sensitivity index. Psychosom. Med. 2007, 69, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Schiller, D.; Alessandra, N.C.; Alia-Klein, N.; Becker, S.; Cromwell, H.C.; Dolcos, F.; Eslinger, P.J.; Frewen, P.; Kemp, A.H.; Pace-Schott, E.F.; et al. The human affectome. Neurosci. Biobehav. Rev. 2023, 158, 105450. [Google Scholar] [CrossRef]
- Atanasova, K.; Lotter, T.; Reindl, W.; Lis, S. Multidimensional Assessment of Interoceptive Abilities, Emotion Processing and the Role of Early Life Stress in Inflammatory Bowel Diseases. Front. Psychiatry 2021, 12, 680878. [Google Scholar] [CrossRef]
- Gîlcă-Blanariu, G.E.; Șchiopu, C.G.; Ștefănescu, G.; Mihai, C.; Diaconescu, S.; Afrăsânie, V.A.; Lupu, V.V.; Lupu, A.; Boloș, A.; Ștefănescu, C. The intertwining roads between psychological distress and gut microbiota in inflammatory bowel disease. Microorganisms 2023, 11, 2268. [Google Scholar] [CrossRef] [PubMed]
- Fairbrass, K.M.; Costantino, S.J.; Gracie, D.J.; Ford, A.C. Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Belvedere, A.; Scoglio, R.; Viola, A.; Costantino, G.; Sitibondo, A.; Muscianisi, M.; Inferrera, S.; Alibrandi, A.; Fries, W. A real world investigation on prevalence, clinical features, and therapy of inflammatory bowel disease in the city of Messina, Italy. Acta Bio Med. Atenei Parmensis 2021, 92, e2021161. [Google Scholar]
- Viola, A.; Fontana, A.; Belvedere, A.; Scoglio, R.; Costantino, G.; Sitibondo, A.; Muscianisi, M.; Inferrera, S.; Bruno, L.M.; Alibrandi, A.; et al. Diagnostic accuracy of faecal calprotectin in a symptom-based algorithm for early diagnosis of inflammatory bowel disease adjusting for differential verification bias using a Bayesian approach. Scand. J. Gastroenterol. 2020, 55, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Yildrim, M.; Turan, M.E.; Albeladi, N.S.; Crescenzo, P.; Rizzo, A.; Nucera, G.; Ferrari, G.; Navolokina, A.; Szarpak, L.; Chirico, F. Resilience and perceived social support as predictors of emotional well-being. J. Health Soc. Sci. 2023, 8, 59–75. [Google Scholar]

{kind=link}
{kind=link}
| Variable | Category | CD (n = 111) | UC (n = 180) | IBS (n = 34) | HC (n = 164) |
|---|---|---|---|---|---|
| Gender | Males | 4.72% | 5.13% | 2.05% | 9.86% |
| Females | 18.07% | 31.83% | 4.93% | 23.41% | |
| Other | 0.00% | 0.00% | 0.00% | 0.21% | |
| Age Group | 18–30 years | 6.37% | 14.78% | 3.49% | 23.20% |
| 31–45 years | 10.06% | 14.37% | 1.44% | 3.70% | |
| 46–60 years | 5.54% | 7.19% | 1.23% | 4.11% | |
| 61–75 years | 0.82% | 0.62% | 0.41% | 2.46% | |
| 76–85 years | 0.00% | 0.00% | 0.21% | 0.00% | |
| Region of Residence | North | 8.62% | 16.43% | 0.21% | 3.08% |
| Center | 4.93% | 6.57% | 0.41% | 1.64% | |
| South | 4.93% | 8.62% | 4.93% | 21.36% | |
| Islands | 4.31% | 5.34% | 1.44% | 7.39% | |
| Education Level | Elementary | 0.00% | 0.21% | 0.00% | 0.00% |
| Lower Secondary | 3.49% | 1.64% | 0.21% | 2.26% | |
| Upper Secondary | 11.29% | 17.66% | 3.70% | 18.89% | |
| Diploma | 0.41% | 0.41% | 0.00% | 0.41% | |
| Bachelor’s Degree | 4.11% | 8.01% | 1.85% | 8.21% | |
| Postgraduate | 2.87% | 7.39% | 1.23% | 3.70% | |
| Occupational Status | Student | 4.31% | 6.57% | 3.08% | 20.74% |
| Employee | 6.16% | 15.81% | 1.44% | 4.72% | |
| Freelancer | 2.67% | 4.52% | 0.82% | 2.05% | |
| Worker | 3.08% | 2.87% | 0.62% | 1.23% | |
| Housewife | 4.11% | 3.29% | 0.62% | 2.05% | |
| Retired | 0.41% | 0.21% | 0.21% | 0.82% | |
| Marital Status | Single | 6.78% | 12.12% | 3.08% | 18.89% |
| Married | 9.65% | 14.17% | 2.46% | 10.06% | |
| Cohabiting | 4.93% | 9.65% | 0.82% | 2.87% | |
| Separated | 1.03% | 0.41% | 0.21% | 0.21% | |
| Divorced | 0.41% | 0.62% | 0.21% | 1.23% | |
| Widowed | 0.00% | 0.00% | 0.21% | 0.21% |
| VSI-IT Item | Item Factor Loading |
|---|---|
| Item 1—I worry that whenever I eat during the day, bloating and distension in my belly will get worse/Temo che ogni volta che mangio durante il giorno, il gonfiore e la distensione della pancia peggioreranno. | 0.67 |
| Item 2—I get anxious when I go to a new restaurant/Divento ansioso quando vado in un nuovo ristorante. | 0.74 |
| Item 3—I often worry about problems in my belly/Mi preoccupo spesso per problemi alla pancia. | 0.83 |
| Item 4—I have a difficult time enjoying myself because I cannot get my mind off of discomfort in my belly/Ho difficoltà a divertirmi perché non riesco a distogliere la mente dal disagio della pancia. | 0.83 |
| Item 5—I often fear that I won’t be able to have a normal bowel movement/Spesso temo di non riuscire ad avere un normale movimento intestinale. | 0.82 |
| Item 6—Because of fear of developing abdominal discomfort, I seldom try new foods/A causa della paura di sviluppare disturbi addominali, raramente provo cibi nuovi. | 0.78 |
| Item 7—No matter what I eat, I will probably feel uncomfortable/Qualunque cosa mangi, probabilmente mi sentirò a disagio. | 0.80 |
| Item 8—As soon as I feel abdominal discomfort, I begin to worry and feel anxious/Non appena sento fastidio addominale comincio a preoccuparmi e a sentirmi ansioso. | 0.83 |
| Item 9—When I enter a place I haven’t been before, one of the first things I do is to look for a bathroom/Quando entro in un posto dove non sono mai stato, una delle prime cose che faccio è cercare un bagno. | 0.71 |
| Item 10—I am constantly aware of the feelings I have in my belly/Sono costantemente consapevole delle sensazioni che ho nella mia pancia. | 0.58 |
| Item 11—I often feel discomfort in my belly could be a sign of a serious illness/Sento spesso che il fastidio alla pancia potrebbe essere segno di una grave malattia. | 0.76 |
| Item 12—As soon as I awake, I worry that I will have discomfort in my belly during the day/Non appena mi sveglio, temo che avrò fastidio alla pancia durante il giorno. | 0.83 |
| Item 13—When I feel discomfort in my belly, it frightens me/Quando sento disagio nel mio ventre, mi spavento. | 0.76 |
| Item 14—In stressful situations, my belly bothers me a lot/In situazioni stressanti, la mia pancia mi dà molto fastidio. | 0.72 |
| Item 15—I constantly think about what is happening inside my belly/Penso costantemente a ciò che sta accadendo nella mia pancia. | 0.84 |
| N | Mean | Std. Deviation | Std. Error | 95% CI | ||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Healthy controls | 164 | 21.60 | 14.90 | 1.16 | 19.29 | 23.90 |
| Crohn’s disease | 111 | 45.53 | 15.65 | 1.48 | 42.58 | 48.47 |
| Ulcerative rectocolitis | 180 | 47.06 | 16.31 | 1.21 | 44.66 | 49.46 |
| Irritable bowel syndrome | 34 | 38.94 | 16.70 | 2.86 | 33.11 | 44.76 |
| Awaiting diagnosis | 11 | 41.36 | 11.86 | 3.57 | 33.39 | 49.33 |
| Sample 1 | Sample 2 | Mean Difference (I-J) | Std. Error | Sig. | 95% C.I. | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Healthy controls | Crohn’s disease | −23.93 * | 1.92 | <0.001 | −29.36 | −18.49 |
| Ulcerative rectocolitis | −25.46 * | 1.69 | <0.001 | −30.24 | −20.69 | |
| Irritable bowel syndrome | −17.33 * | 2.95 | <0.001 | −25.66 | −9.01 | |
| Awaiting diagnosis | −19.76 * | 4.87 | <0.001 | −33.51 | −6.00 | |
| Crohn’s disease | Healthy controls | 23.93 * | 1.92 | <0.001 | 18.49 | 29.36 |
| Ulcerative rectocolitis | −1.53 | 1.89 | 1.000 | −6.86 | 3.79 | |
| Irritable bowel syndrome | 6.59 | 3.06 | 0.323 | −2.06 | 15.24 | |
| Awaiting diagnosis | 4.16 | 4.95 | 1.000 | −9.79 | 18.12 | |
| Ulcerative rectocolitis | Healthy controls | 25.46 * | 1.69 | <0.001 | 20.69 | 30.24 |
| Crohn’s disease | 1.53 | 1.89 | 1.000 | −3.79 | 6.86 | |
| Irritable bowel syndrome | 8.12 | 2.92 | 0.057 | −0.13 | 16.38 | |
| Awaiting diagnosis | 5.70 | 4.86 | 1.000 | −8.01 | 19.41 | |
| Irritable bowel syndrome | Healthy controls | 17.33 * | 2.95 | <0.001 | 9.01 | 25.66 |
| Crohn’s disease | −6.59 | 3.06 | 0.323 | −15.24 | 2.06 | |
| Ulcerative rectocolitis | −8.12 | 2.92 | 0.057 | −16.38 | 0.13 | |
| Awaiting diagnosis | −2.42 | 5.43 | 1.000 | −17.74 | 12.89 | |
| Awaiting diagnosis | Healthy controls | 19.76 * | 4.87 | <0.001 | 6.00 | 33.51 |
| Crohn’s disease | −4.16 | 4.95 | 1.000 | −18.12 | 9.79 | |
| Ulcerative rectocolitis | −5.70 | 4.86 | 1.000 | −19.41 | 8.01 | |
| Irritable bowel syndrome | 2.42 | 5.43 | 1.000 | −12.89 | 17.74 | |
| W | N | Mean | Std. Deviation | Std. Error | 95% C.I. | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Absent | 54 | 34.79 | 17.85 | 2.42 | 29.92 | 39.66 |
| Mild | 94 | 43.57 | 16.43 | 1.69 | 40.20 | 46.94 |
| Moderate | 144 | 47.82 | 13.15 | 1.09 | 45.66 | 49.99 |
| Severe | 41 | 55.73 | 14.13 | 2.20 | 51.26 | 60.19 |
| Symptoms Severity | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Absent | Mild | −8.77 * | 2.57 | 0.004 | −15.60 | −1.94 |
| Moderate | −13.03 * | 2.40 | <0.001 | −19.41 | −6.64 | |
| Severe | −20.93 * | 3.12 | <0.001 | −29.22 | −12.64 | |
| Mild | Absent | 8.77 * | 2.57 | 0.004 | 1.94 | 15.60 |
| Moderate | −4.25 | 1.99 | 0.205 | −9.55 | 1.05 | |
| Severe | −12.15 * | 2.82 | <0.001 | −19.64 | −4.66 | |
| Moderate | Absent | 13.03 * | 2.40 | <0.001 | 6.64 | 19.41 |
| Mild | 4.25 | 1.99 | 0.205 | −1.05 | 9.55 | |
| Severe | −7.90 * | 2.66 | 0.020 | −14.98 | −0.82 | |
| Severe | Absent | 20.93 * | 3.12 | <0.001 | 12.64 | 29.22 |
| Mild | 12.15 * | 2.82 | <0.001 | 4.66 | 19.64 | |
| Moderate | 7.90 * | 2.66 | 0.020 | 0.82 | 14.98 | |
| Variable | Visceral Sensitivity Index |
|---|---|
| Noticing | 0.277 ** |
| Not distracting | −0.044 |
| Not worrying | −0.414 ** |
| Attention regulation | −0.142 ** |
| Emotional awareness | 0.235 ** |
| Self-regulation | −0.135 * |
| Body listening | 0.056 |
| Trusting | −0.302 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, A.; Mautone, A.; Sitibondo, A.; Nucera, G.; Tarchi, L.; Khabbache, H.; Ait Ali, D.; Ouazizi, K.; Szarpak, Ł.; Pruc, M.; et al. VISCERAL SENSITIVITY INDEX (VSI-IT): Italian Adaptation and Validation. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 1953-1968. https://doi.org/10.3390/ejihpe14070130
Rizzo A, Mautone A, Sitibondo A, Nucera G, Tarchi L, Khabbache H, Ait Ali D, Ouazizi K, Szarpak Ł, Pruc M, et al. VISCERAL SENSITIVITY INDEX (VSI-IT): Italian Adaptation and Validation. European Journal of Investigation in Health, Psychology and Education. 2024; 14(7):1953-1968. https://doi.org/10.3390/ejihpe14070130
Chicago/Turabian StyleRizzo, Amelia, Aurora Mautone, Aldo Sitibondo, Gabriella Nucera, Livio Tarchi, Hicham Khabbache, Driss Ait Ali, Khalid Ouazizi, Łukasz Szarpak, Michal Pruc, and et al. 2024. "VISCERAL SENSITIVITY INDEX (VSI-IT): Italian Adaptation and Validation" European Journal of Investigation in Health, Psychology and Education 14, no. 7: 1953-1968. https://doi.org/10.3390/ejihpe14070130
APA StyleRizzo, A., Mautone, A., Sitibondo, A., Nucera, G., Tarchi, L., Khabbache, H., Ait Ali, D., Ouazizi, K., Szarpak, Ł., Pruc, M., Yıldırım, M., & Chirico, F. (2024). VISCERAL SENSITIVITY INDEX (VSI-IT): Italian Adaptation and Validation. European Journal of Investigation in Health, Psychology and Education, 14(7), 1953-1968. https://doi.org/10.3390/ejihpe14070130