

The Vaccination Fear Scale (VFS-6): Adaptation, Cross-Cultural Validation, and Invariance among Genders and Six Different Cultures, Applying Classical Test Theory (CTT) and Item Response Theory (IRT)

 ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
2.3. Instruments
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
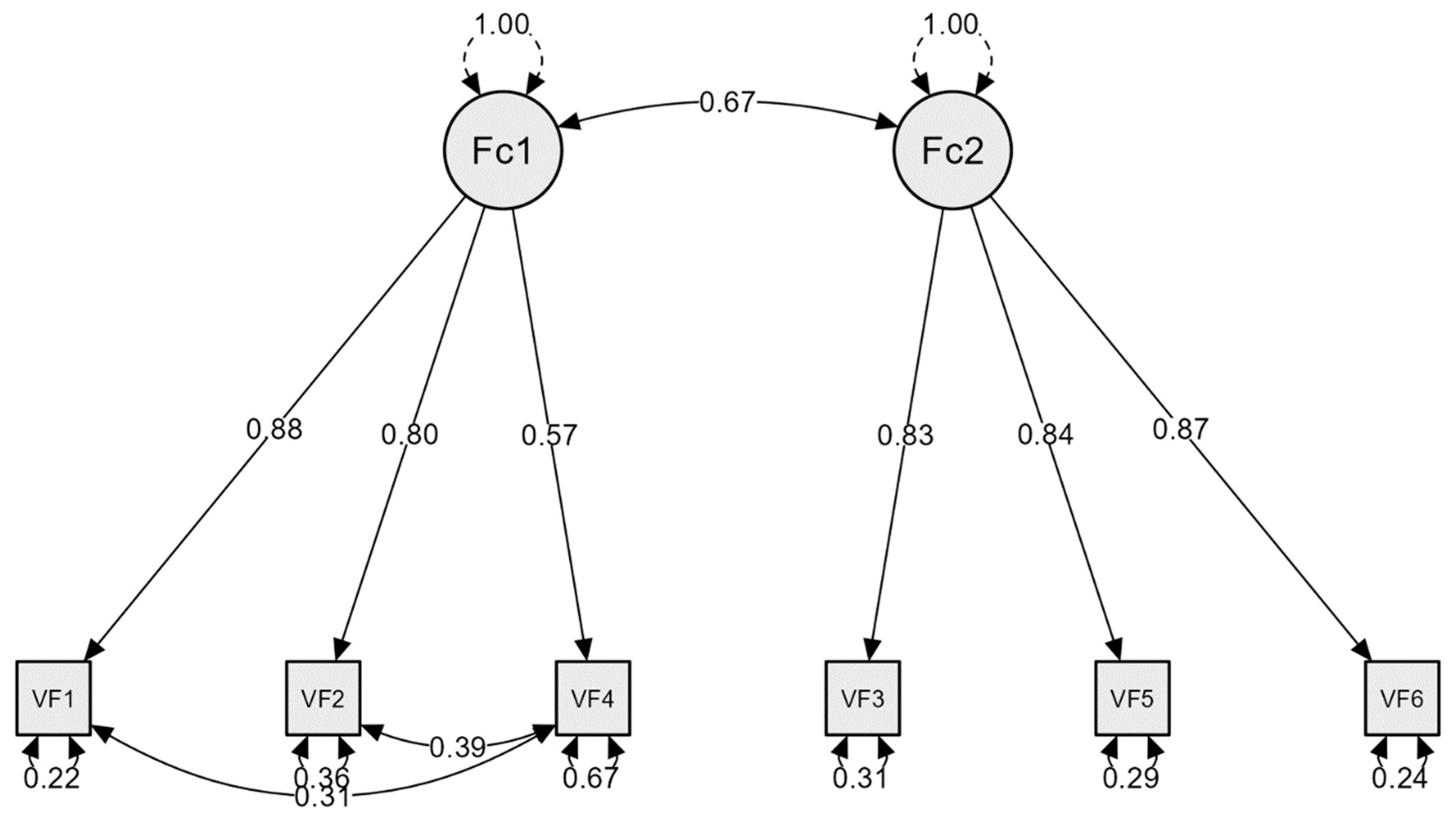
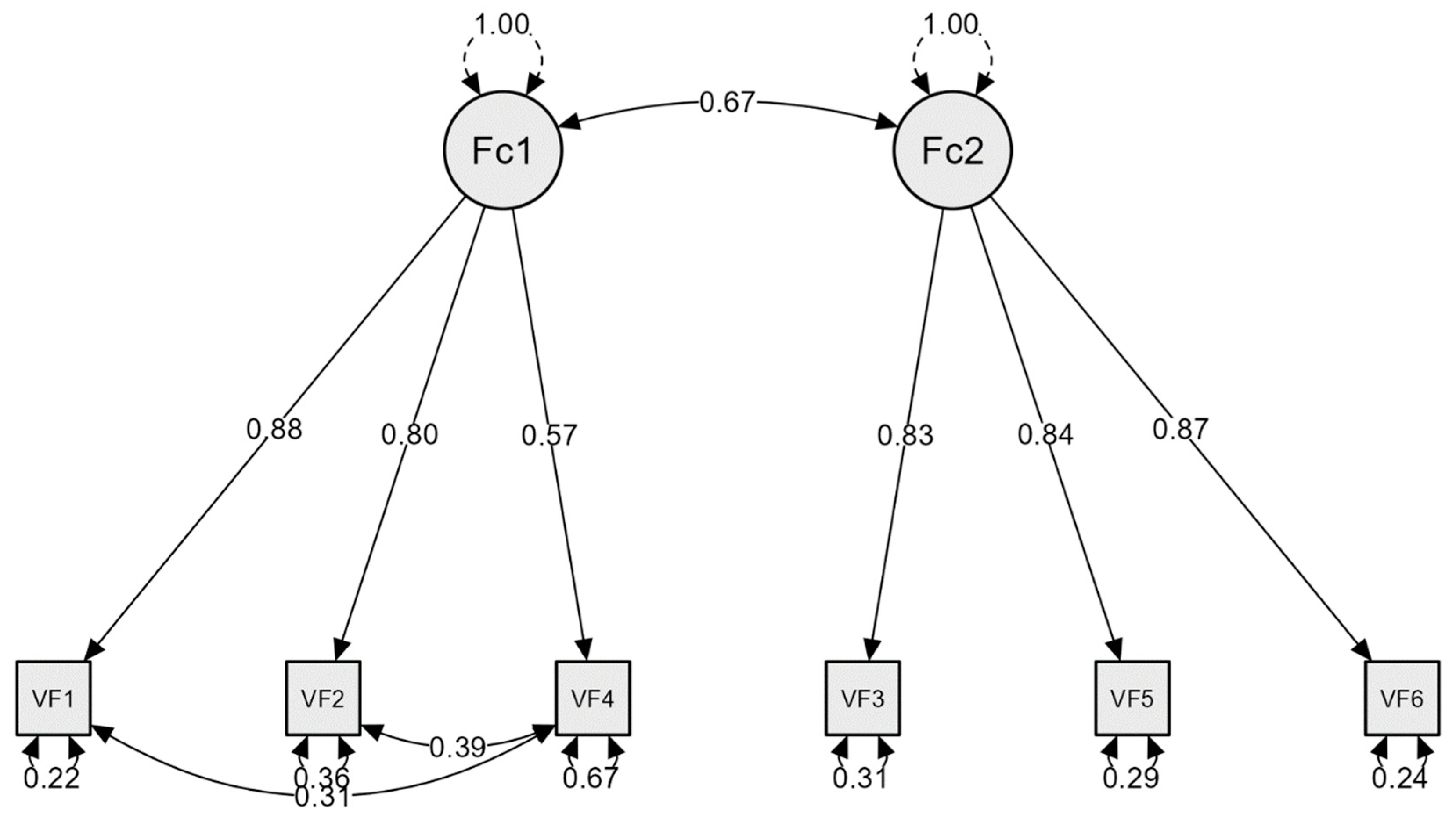
3.2. Confirmatory Factor Analysis
3.3. Reliability and Validity
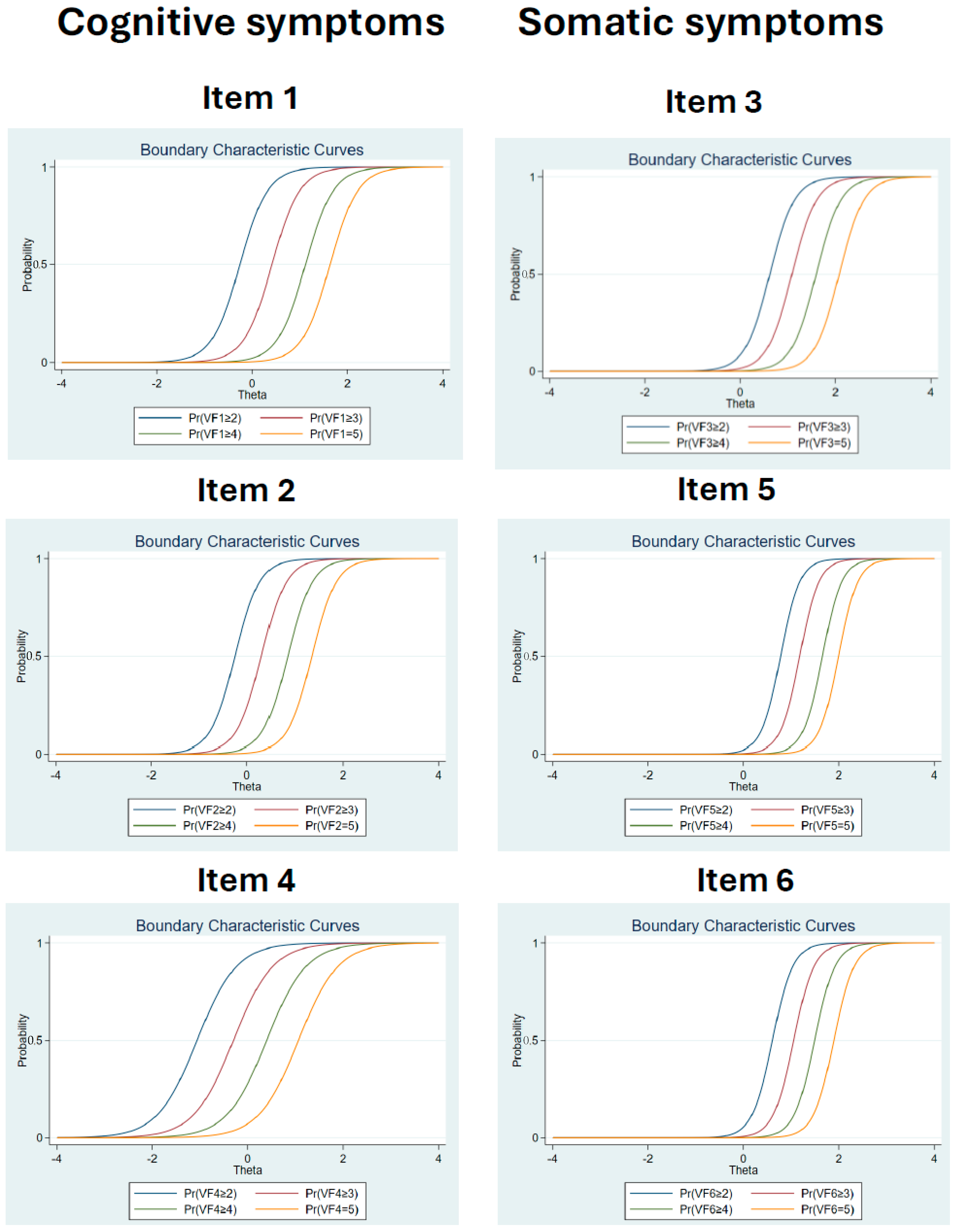
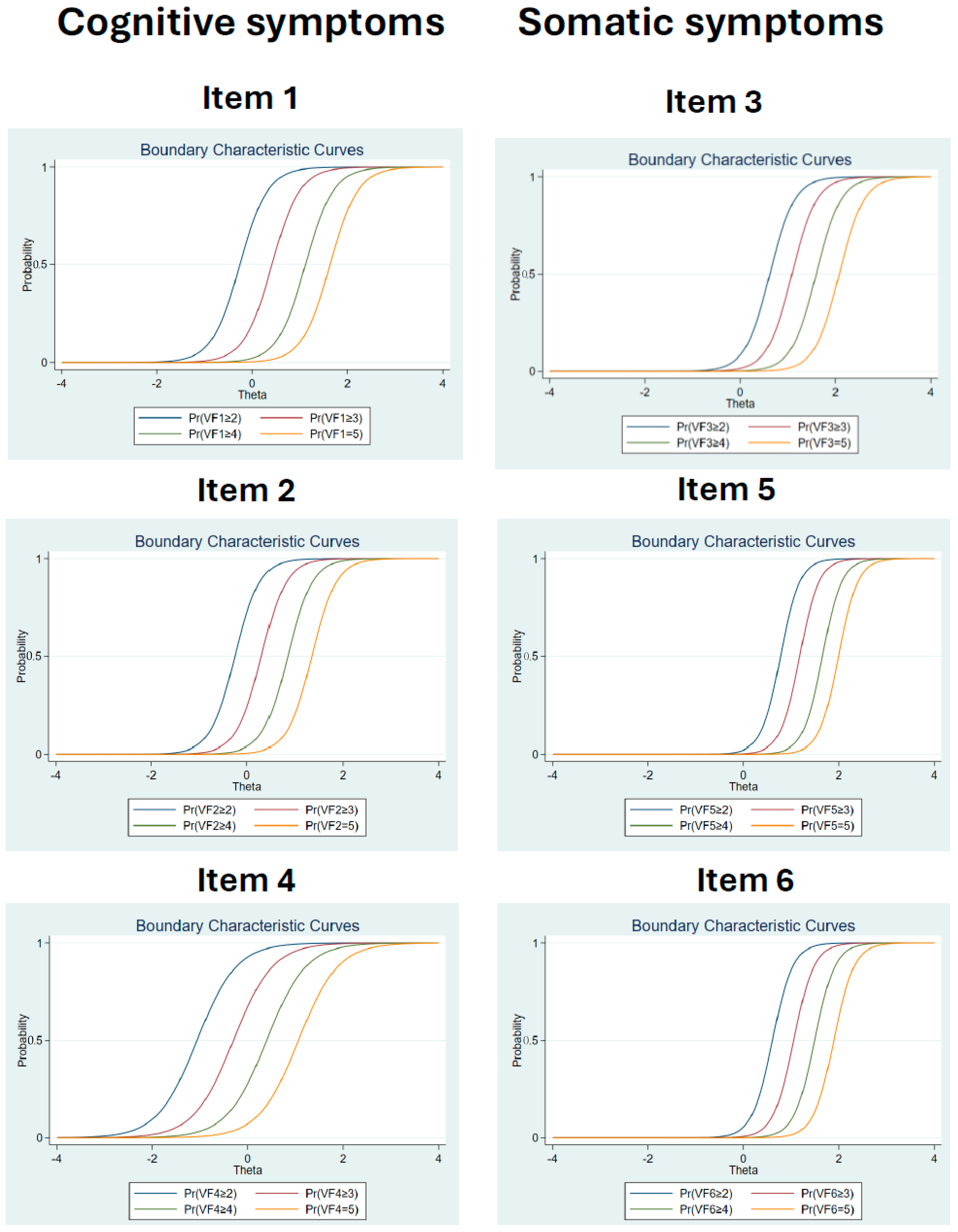
3.4. Item Response Theory (IRT) Analysis
3.5. Measurement Invariance
4. Discussion
Limitations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO) Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 24 January 2024).
- World Health Organization (WHO). Health in the 2030 Agenda for Sustainable Development. Sixty-Ninth World Health Assembly. Doc. A 2016, 69, 2000–2019. [Google Scholar]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. The COVID-19 Vaccine Is Here—Now Who Is Willing to Get It? Vaccines 2021, 9, 339. [Google Scholar] [CrossRef]
- Simione, L.; Vagni, M.; Gnagnarella, C.; Bersani, G.; Pajardi, D. Mistrust and beliefs in conspiracy theories differently mediate the effects of psychological factors on propensity for COVID-19 vaccine. Front. Psychol. 2021, 12, 683684. [Google Scholar] [CrossRef]
- Simione, L.; Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. How Implicit Attitudes toward Vaccination Affect Vaccine Hesitancy and Behaviour: Developing and Validating the V-IRAP. Int. J. Environ. Res. Public Health 2022, 19, 4205. [Google Scholar] [CrossRef]
- Seddig, D.; Maskileyson, D.; Davidov, E.; Ajzen, I.; Schmidt, P. Correlates of COVID-19 vaccination intentions: Attitudes, institutional trust, fear, conspiracy beliefs, and vaccine skepticism. Soc. Sci. Med. 2022, 302, 114981. [Google Scholar] [CrossRef] [PubMed]
- Willis, D.E.; Andersen, J.A.; Bryant-Moore, K.; Selig, J.P.; Long, C.R.; Felix, H.C.; McElfish, P.A. COVID-19 vaccine hesitancy: Race/ethnicity, trust, and fear. Clin. Transl. Sci. 2021, 14, 2200–2207. [Google Scholar] [CrossRef] [PubMed]
- Duradoni, M.; Veloso, M.V.; Gamma, M.L.; Monciatti, A.M.; Guazzini, A. Italian Version of the Vaccination Fear Scale (VFS-6): Internal and External Validation. Mediterr. J. Clin. Psychol. 2022, 10. [Google Scholar] [CrossRef]
- Malas, O.; Tolsá, M.D. Vaccination Fear Scale (VFS-6): Development and Initial Validation. Mediterr. J. Clin. Psychol. 2021, 9. [Google Scholar] [CrossRef]
- Rief, W. Fear of adverse effects and COVID-19 vaccine hesitancy: Recommendations of the treatment expectation expert group. JAMA Health Forum 2021, 2, e210804. [Google Scholar] [CrossRef] [PubMed]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef]
- Pakpour, A.H.; Griffiths, M.D. The fear of COVID-19 and its role in preventive behaviors. J. Concurr. Disord. 2020, 2, 58–63. Available online: http://irep.ntu.ac.uk/id/eprint/39561/ (accessed on 21 January 2024). [CrossRef]
- Sato, R.; Fintan, B. Fear, knowledge, and vaccination behaviors among women in Northern Nigeria. Hum. Vaccines Immunother. 2020, 16, 2438–2448. [Google Scholar] [CrossRef] [PubMed]
- Tahir, A.I.; Ramadhan, D.S.; Taha, A.A.; Abdullah, R.Y.; Karim, S.K.; Ahmed, A.K.; Ahmed, S.F. Public fear of COVID-19 vaccines in Iraqi Kurdistan region: A cross-sectional study. Middle East Curr. Psychiatry 2021, 28, 46. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Benatov, J.; Arzenšek, A. Adaptation and Preliminary Validation of the Fear of Coronavirus Vaccination Scale in the Prospective Study among a Representative Sample of Polish, Israeli, Slovenian, and German Adults during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 11587. [Google Scholar] [CrossRef] [PubMed]
- Gregory, M.E.; MacEwan, S.R.; Powell, J.R.; Volney, J.; Kurth, J.D.; Kenah, E.; Panchal, A.R.; McAlearney, A.S. The COVID-19 Vaccine Concerns Scale: Development and Validation of a New Measure. Hum. Vaccines Immunother. 2022, 18, 2050105. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.; Hagger, M.S. The Vaccination Concerns in COVID-19 Scale (VaCCS): Development and Validation. PLoS ONE 2022, 17, e0264784. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, G.K.; Kaufman, J.; Brewer, N.T.; Wiley, K.; Menning, L.; Leask, J.; Wiysonge, C.S. A critical review of measures of childhood vaccine confidence. Curr. Opin. Immunol. 2021, 71, 34–45. [Google Scholar] [CrossRef]
- Oduwole, E.O.; Pienaar, E.D.; Mahomed, H.; Wiysonge, C.S. Overview of tools and measures investigating vaccine hesitancy in a ten year period: A scoping review. Vaccines 2022, 10, 1198. [Google Scholar] [CrossRef]
- Kotta, I.; Kalcza-Janosi, K.; Szabo, K.; Marschalko, E.E. Development and Validation of the Multidimensional COVID-19 Vaccine Hesitancy Scale. Hum. Vaccines Immunother. 2022, 18, 1–10. [Google Scholar] [CrossRef]
- Luyten, J.; Bruyneel, L.; van Hoek, A.J. Assessing Vaccine Hesitancy in the UK Population Using a Generalized Vaccine Hesitancy Survey Instrument. Vaccine 2019, 37, 2494–2501. [Google Scholar] [CrossRef]
- Alam, M.M.; Melhim, L.K.B.; Ahmad, M.T.; Jemmali, M. Public attitude towards COVID-19 vaccination: Validation of covid-vaccination attitude scale (c-vas). J. Multidiscip. Healthc. 2022, 15, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 20, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Tolsa, M.D.; Malas Tolsá, O. Miedo y creencias sobre la vacunación en docentes de enseñanza obligatoria durante la pandemia por COVID-19. Rev. Española Salud Pública 2022, 96, e1–e14. [Google Scholar]
- Malas, O. Influence of Fear on Anti-Vaccine Conspiracy Theories and Behaviour against Vaccination. Rev. Psicol. Salud 2023, 11, 179–192. [Google Scholar] [CrossRef]
- Hinkle, J.L. The Importance of Cross-Cultural Adaptation of Health Measures. J. Nurs. Meas. 2023, 3, 479. [Google Scholar] [CrossRef]
- Bader, M.; Jobst, L.J.; Zettler, I.; Hilbig, B.E.; Moshagen, M. Disentangling the effects of culture and language on measurement noninvariance in cross-cultural research: The culture, comprehension, and translation bias (CCT) procedure. Psychol. Assess. 2021, 33, 375. [Google Scholar] [CrossRef] [PubMed]
- Mesoudi, A. Cultural selection and biased transformation: Two dynamics of cultural evolution. Philos. Trans. R. Soc. B 2021, 376, 20200053. [Google Scholar] [CrossRef]
- Lacko, D.; Čeněk, J.; Točík, J.; Avsec, A.; Đorđević, V.; Genc, A.; Subotić, S. The necessity of testing measurement invariance in cross-cultural research: Potential bias in cross-cultural comparisons with individualism–collectivism self-report scales. Cross-Cult. Res. 2022, 56, 228–267. [Google Scholar] [CrossRef]
- Byrne, B.M.; Shavelson, R.J.; Muthén, B. Testing for the Equivalence of Factor Covariance and Mean Structures: The Issue of Partial Measurement Invariance. Psychol. Bull. 1989, 105, 456–466. [Google Scholar] [CrossRef]
- Hsiao, Y.Y.; Lai, M.H.C. The Impact of Partial Measurement Invariance on Testing Moderation for Single and Multi-Level Data. Front. Psychol. 2018, 9, 298874. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994; ISBN 978-0-07-047849-7. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson College Div: Boston, MA, USA, 2006; ISBN 978-0-205-45938-4. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Alam, M.D.; Abedin, M.J.; Islam, A.; Mosfeq-Ul-Hasan, M.; Rahman, O.; Xu, Y. Psychological effects and associated factors among vaccinated and unvaccinated general population against COVID-19 infection in Bangladesh. Front. Psychiatry 2022, 13, 916160. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Baker, F.B. The Basics of Item Response Theory, 2nd ed.; ERIC Clearinghouse on Assessment and Evaluation: College Park, MD, USA, 2001; Available online: http://echo.edres.org:8080/irt/baker/ (accessed on 21 January 2024).
- Reise, S.P.; Scheines, R.; Widaman, K.F.; Haviland, M.G. Multidimensionality and Structural Coefficient Bias in Structural Equation Modeling: A Bifactor Perspective. Educ. Psychol. Meas. 2013, 73, 5–26. [Google Scholar] [CrossRef]
- Kline, P. A Handbook of Test Construction (Psychology Revivals): Introduction to Psychometric Design; Routledge: London, UK, 2015; ISBN 978-1-315-69599-0. [Google Scholar]
- Nevitt, J.; Hancock, G.R. Performance of Bootstrapping Approaches to Model Test Statistics and Parameter Standard Error Estimation in Structural Equation Modeling. Struct. Equ. Model. A Multidiscip. J. 2001, 8, 353–377. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Monger, K.; Zarate, D.; Prokofieva, M.; Schivinski, B. Online Gambling Disorder Questionnaire (OGD-Q): An item response theory examination. Addict. Behav. Rep. 2022, 16, 100449. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M. Constructing Measures: An Item Response Modeling Approach; Routledge: London, UK, 2023. [Google Scholar]
- Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental Health Issues during and after COVID-19 Vaccine Era. Brain Res. Bull. 2021, 176, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Kimble, C.; Coustasse, A.; Maxik, K. Considerations on the distribution and administration of the new COVID-19 vaccines. Int. J. Healthc. Manag. 2021, 14, 306–310. [Google Scholar] [CrossRef]
- Mustapha, M.; Lawal, B.K.; Sha’aban, A.; Jatau, A.I.; Wada, A.S.; Bala, A.A.; Mustapha, S.; Haruna, A.; Musa, A.; Ahmad, M.H.; et al. Factors associated with acceptance of COVID-19 vaccine among University health sciences students in Northwest Nigeria. PLoS ONE 2021, 29, e0260672. [Google Scholar] [CrossRef]
- Patelarou, E.; Galanis, P.; Mechili, E.A.; Argyriadi, A.; Argyriadis, A.; Asimakopoulou, E.; Brokaj, S.; Bucaj, J.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; et al. Factors influencing nursing students’ intention to accept COVID-19 vaccination: A pooled analysis of seven European countries. Nurse Educ. Today 2021, 104, 105010. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Sample Nationality | Cross-Country Comparison | |||||||
|---|---|---|---|---|---|---|---|---|
| TS | 1 | 2 | 3 | 4 | 5 | 6 | ||
| Age | ||||||||
| Mean | 20.60 | 21.37 | 21.78 | 20.25 | 19.95 | 21.53 | 18.69 | χ2/df = 30.4 |
| SD | 2.04 | 2.07 | 1.79 | 1.13 | 2.36 | 1.41 | 1.34 | p < 0.001 |
| Sex (%) | ||||||||
| Male | 26.75 | 20.10 | 21.01 | 41.27 | 31.20 | 20.24 | 19.81 | χ2/df = 17.94 |
| Female | 73.25 | 79.90 | 78.99 | 58.73 | 68.80 | 79.76 | 80.19 | p < 0.001 |
| Branch (%) | ||||||||
| Health Sci. | 28.28 | 25.77 | 23.40 | 20.94 | 61.50 | 3.66 | 21.41 | χ2/df = 45.90 |
| Social Sci. | 32.66 | 37.11 | 10.37 | 51.64 | 17.11 | 54.88 | 23.32 | p < 0.001 |
| Pure Sci. | 10.25 | 12.89 | 2.66 | 13.35 | 12.66 | 12.19 | 4.47 | |
| Humanities | 17.59 | 15.21 | 35.37 | 3.90 | 1.60 | 25.12 | 39.30 | |
| Engineering | 5.56 | 0.51 | 8.77 | 6.16 | 7.13 | 0.00 | 11.50 | |
| Other | 5.64 | 8.50 | 19.41 | 4.11 | 0.00 | 4.15 | 0.00 | |
| Vaccination (%) | ||||||||
| Yes | 76.41 | 96.40 | 96.01 | 87.47 | 37.61 | 92.93 | 58.79 | χ2/df = 156.73 |
| No | 23.59 | 3.60 | 3.99 | 12.53 | 62.39 | 7.07 | 41.21 | p < 0.001 |
| Sample | Vaccination (%) | Mean (SD) | Skewness | Kurtosis | K-S | ||
|---|---|---|---|---|---|---|---|
| z | p | ||||||
| VFS-6 | TS | 76.40 | 12.09 (5.56) | 0.99 | 0.28 | 7.00 | 0.000 |
| 1 | 96.39 | 9.82 (4.81) | 2.02 | 4.45 | 4.12 | 0.000 | |
| 2 | 96.01 | 9.69 (4.30) | 1.69 | 2.64 | 3.92 | 0.000 | |
| 3 | 87.47 | 12.69 (5.50) | 0.84 | −0.40 | 3.47 | 0.000 | |
| 4 | 37.61 | 14.63 (5.92) | 0.46 | −0.50 | 2.31 | 0.000 | |
| 5 | 92.92 | 13.29 (5.48) | 0.74 | 0.17 | 1.91 | 0.000 | |
| 6 | 76.41 | 10.61 (4.58) | 1.33 | 1.64 | 2.79 | 0.000 | |
| F1 | TS | -- | 7.43 (3.55) | 0.53 | −0.79 | 6.94 | 0.000 |
| 1 | -- | 6.09 (3.16) | 1.02 | 0.13 | 4.19 | 0.000 | |
| 2 | -- | 5.90 (2.97) | 1.23 | 0.88 | 3.50 | 0.000 | |
| 3 | -- | 7.16 (3.13) | 0.63 | 0.49 | 3.18 | 0.000 | |
| 4 | -- | 9.17 (3.63) | −0.02 | −1.01 | 1.95 | 0.000 | |
| 5 | -- | 8.55 (3.57) | 0.14 | −0.95 | 1.86 | 0.000 | |
| 6 | -- | 6.79 (3.32) | 0.71 | −0.42 | 2.70 | 0.000 | |
| F2 | TS | -- | 4.65 (2.77) | 1.88 | 2.76 | 15.92 | 0.000 |
| 1 | -- | 3.80 (2.19) | 3.42 | 11.88 | 8.68 | 0.000 | |
| 2 | -- | 3.79 (1.86) | 2.94 | 8.84 | 8.13 | 0.000 | |
| 3 | -- | 5.53 (3.04) | 1.25 | 0.48 | 4.82 | 0.000 | |
| 4 | -- | 5.47 (3.26) | 1.20 | 0.33 | 6.12 | 0.000 | |
| 5 | -- | 4.75 (2.82) | 1.87 | 2.95 | 6.18 | 0.000 | |
| 6 | -- | 3.81 (1.85) | 3.85 | 13.68 | 6.77 | 0.000 | |
| χ2/df | p | TLI | CFI | RMSEA | RMSEA IC 90% | SRMR | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | TS | 153.14 | <0.001 | 0.737 | 0.860 | 0.245 | 0.220–0.269 | 0.095 | ||
| Model 2 | TS | 8. | <0.001 | 0.986 | 0.995 | 0.056 | 0.043–0.070 | 0.016 | ||
| M | 3.70 | <0.001 | 0.979 | 0.992 | 0.065 | 0.039–0.096 | 0.021 | |||
| F | 5.28 | <0.001 | 0.990 | 0.996 | 0.048 | 0.032–0.065 | 0.016 | |||
| 1 | 3.25 | 0.003 | 0.980 | 0.992 | 0.076 | 0.040–0.115 | 0.017 | |||
| 2 | 2.88 | 0.008 | 0.981 | 0.992 | 0.071 | 0.033–0.111 | 0.018 | |||
| 3 | 2.13 | 0.046 | 0.990 | 0.996 | 0.048 | 0.006–0.085 | 0.013 | |||
| 4 | 3.28 | 0.003 | 0.977 | 0.991 | 0.064 | 0.034–0.096 | 0.023 | |||
| 5 | 2.44 | 0.024 | 0.984 | 0.994 | 0.059 | 0.020–0.098 | 0.022 | |||
| 6 * | 2.06 | 0.082 | 0.983 | 0.995 | 0.058 | 0.000–0.115 | 0.014 | |||
| Model 3 | TS | 12.24 | <0.001 | 0.983 | 0.994 | 0.062 | 0.047–0.077 | 0.016 | ||
| M | 4.68 | <0.001 | 0.974 | 0.991 | 0.074 | 0.045–0.105 | 0.021 | |||
| F | 6.34 | <0.001 | 0.988 | 0.996 | 0.054 | 0.037–0.072 | 0.016 | |||
| 1 | 3.91 | 0.002 | 0.974 | 0.991 | 0.087 | 0.048–0.129 | 0.017 | |||
| 2 | 3.45 | 0.004 | 0.975 | 0.992 | 0.081 | 0.041–0.124 | 0.018 | |||
| 3 | 2.56 | 0.025 | 0.986 | 0.995 | 0.057 | 0.018–0.096 | 0.013 | |||
| 4 | 3.94 | 0.001 | 0.970 | 0.990 | 0.072 | 0.041–0.107 | 0.023 | |||
| 5 | 2.92 | 0.012 | 0.978 | 0.993 | 0.068 | 0.029–0.111 | 0.022 | |||
| 6 * | 2.75 | 0.041 | 0.972 | 0.994 | 0.075 | 0.014–0.138 | 0.014 | |||
| Model 2 | α—coefficient | ω—coefficient | AVE | HTMT | ||||||
| VFS-6 | F1 | F2 | VFS-6 | F1 | F2 | F1 | F2 | F1-F2 | ||
| TS | 0.87 | 0.85 | 0.88 | 0.86 | 0.72 | 0.88 | 0.57 | 0.72 | 0.61 | |
| 1 | 0.87 | 0.84 | 0.91 | 0.83 | 0.76 | 0.93 | 0.57 | 0.83 | 0.68 | |
| 2 | 0.87 | 0.89 | 0.87 | 0.88 | 0.80 | 0.89 | 0.66 | 0.73 | 0.62 | |
| 3 | 0.88 | 0.85 | 0.88 | 0.87 | 0.69 | 0.88 | 0.54 | 0.72 | 0.67 | |
| 4 | 0.83 | 0.80 | 0.86 | 0.84 | 0.69 | 0.86 | 0.51 | 0.67 | 0.55 | |
| 5 | 0.84 | 0.83 | 0.99 | 0.84 | 0.70 | 0.89 | 0.55 | 0.73 | 0.53 | |
| 6 | 0.84 | 0.868 | 0.81 | 0.88 | 0.84 | 0.76 | 0.66 | 0.60 | 0.61 | |
| Student’s t-test ** | t | p | Cohen’s d | SE Cohen’s d | 95% CI for Cohen’s d | |||||
| VFS-6 | 13.49 | <0.001 | 0.63 | 0.05 | 0.54–0.72 | |||||
| F1 | 17.03 | <0.001 | 0.80 | 0.05 | 0.70–0.89 | |||||
| F2 | 5.505 | <0.001 | 0.26 | 0.05 | 0.17–0.35 | |||||
| ΔCFI | ΔRMSEA | |||||||
|---|---|---|---|---|---|---|---|---|
| Model Comparison | CFI | M2-M1 | M3-M2 | M4-M3 | RMSEA | M2-M1 | M3-M2 | M4-M3 |
| Sex | 0.995 | −0.003 | −0.005 | −0.003 | 0.053 | 0.007 | 0.006 | −0.004 |
| Country | ||||||||
| Spain/Italy | 0.992 | 0.001 | −0.012 | −0.028 | 0.074 | −0.013 | 0.027 | 0.030 |
| Spain/Lebanon | 0.994 | −0.025 | −0.018 | −0.070 | 0.062 | 0.060 | 0.015 | 0.044 |
| Spain/Nigeria | 0.991 | −0.015 | −0.003 | −0.149 | 0.069 | 0.030 | −0.005 | 0.110 |
| Spain/Turkey | 0.993 | −0.019 | −0.011 | −0.069 | 0.068 | 0.042 | 0.009 | 0.050 |
| Spain/Ukraine | 0.987 | −0.001 | −0.002 | −0.039 | 0.089 | −0.007 | −0.005 | 0.044 |
| Italy/Lebanon | 0.994 | −0.018 | −0.013 | −0.069 | 0.059 | 0.046 | 0.011 | 0.051 |
| Italy/Nigeria | 0.992 | −0.010 | −0.006 | −0.188 | 0.067 | 0.018 | 0.003 | 0.130 |
| Italy/Turkey | 0.993 | −0.013 | −0.027 | −0.086 | 0.065 | 0.03 | 0.034 | 0.055 |
| Italy/Ukraine | 0.987 | −0.001 | −0.017 | −0.028 | 0.087 | −0.008 | 0.025 | 0.018 |
| Lebanon/Nigeria | 0.994 | −0.002 | −0.015 | −0.034 | 0.057 | −0.002 | 0.028 | 0.028 |
| Lebanon/Turkey | 0.995 | −0.001 | −0.027 | −0.014 | 0.054 | −0.004 | 0.055 | 0.002 |
| Lebanon/Ukraine | 0.990 | −0.014 | −0.020 | −0.025 | 0.074 | 0.026 | 0.021 | 0.007 |
| Nigeria/Turkey | 0.992 | 0.001 | −0.008 | −0.031 | 0.062 | −0.012 | 0.015 | 0.033 |
| Nigeria/Ukraine | 0.986 | −0.007 | −0.001 | −0.097 | 0.08 | 0.005 | −0.007 | 0.075 |
| Turey/Ukraine | 0.987 | −0.009 | −0.012 | −0.031 | 0.081 | 0.013 | 0.009 | 0.017 |
| Factor | Item | α | Z | p | β1 | β2 | β3 | β4 |
|---|---|---|---|---|---|---|---|---|
| F1 | 1 | 3.39 | 21.02 | <0.001 | −0.25 | 0.41 | 1.12 | 1.63 |
| 2 | 3.88 | 18.12 | <0.001 | −0.24 | 0.30 | 0.84 | 1.35 | |
| 4 | 2.40 | 25.45 | <0.001 | −1.06 | −0.30 | 0.40 | 1.06 | |
| F2 | 3 | 3.85 | 17.54 | <0.001 | 0.62 | 1.09 | 1.59 | 2.00 |
| 5 | 4.95 | 15.01 | <0.001 | 0.77 | 1.18 | 1.65 | 1.99 | |
| 6 | 4.66 | 15.03 | <0.001 | 0.60 | 1.05 | 1.49 | 1.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malas, O.; Boustani, N.M.; Duradoni, M.; Omotoso, D.; Avşar, A.Ş.; Shyroka, A.; Colombini, G.; Blanch, A. The Vaccination Fear Scale (VFS-6): Adaptation, Cross-Cultural Validation, and Invariance among Genders and Six Different Cultures, Applying Classical Test Theory (CTT) and Item Response Theory (IRT). Eur. J. Investig. Health Psychol. Educ. 2024, 14, 808-822. https://doi.org/10.3390/ejihpe14040052
Malas O, Boustani NM, Duradoni M, Omotoso D, Avşar AŞ, Shyroka A, Colombini G, Blanch A. The Vaccination Fear Scale (VFS-6): Adaptation, Cross-Cultural Validation, and Invariance among Genders and Six Different Cultures, Applying Classical Test Theory (CTT) and Item Response Theory (IRT). European Journal of Investigation in Health, Psychology and Education. 2024; 14(4):808-822. https://doi.org/10.3390/ejihpe14040052
Chicago/Turabian StyleMalas, Olga, Nada Mallah Boustani, Mirko Duradoni, Dayo Omotoso, Asiye Şengül Avşar, Anastasiia Shyroka, Giulia Colombini, and Angel Blanch. 2024. "The Vaccination Fear Scale (VFS-6): Adaptation, Cross-Cultural Validation, and Invariance among Genders and Six Different Cultures, Applying Classical Test Theory (CTT) and Item Response Theory (IRT)" European Journal of Investigation in Health, Psychology and Education 14, no. 4: 808-822. https://doi.org/10.3390/ejihpe14040052
APA StyleMalas, O., Boustani, N. M., Duradoni, M., Omotoso, D., Avşar, A. Ş., Shyroka, A., Colombini, G., & Blanch, A. (2024). The Vaccination Fear Scale (VFS-6): Adaptation, Cross-Cultural Validation, and Invariance among Genders and Six Different Cultures, Applying Classical Test Theory (CTT) and Item Response Theory (IRT). European Journal of Investigation in Health, Psychology and Education, 14(4), 808-822. https://doi.org/10.3390/ejihpe14040052