
An Analytic Hierarchy Process Contingency Analysis of Factors Affecting the Emigration Decision of Medical Doctors in Turkey



Abstract
1. Introduction
2. Literature Review
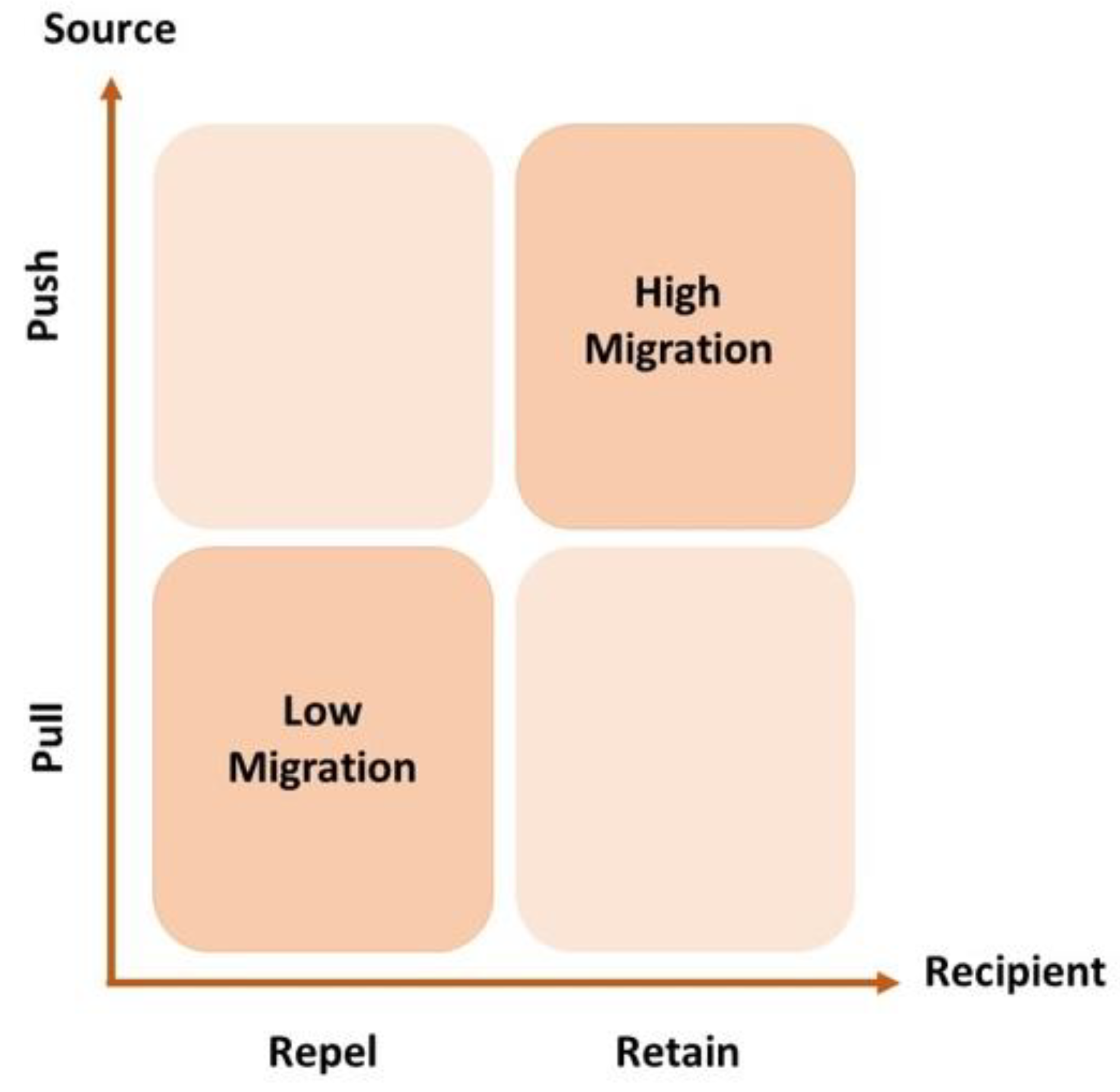
3. Theoretical Framework
- What are the driving factors for MDs’ emigration in Turkey?
- What is the importance of the different factors driving MDs’ decision to emigrate in Turkey?
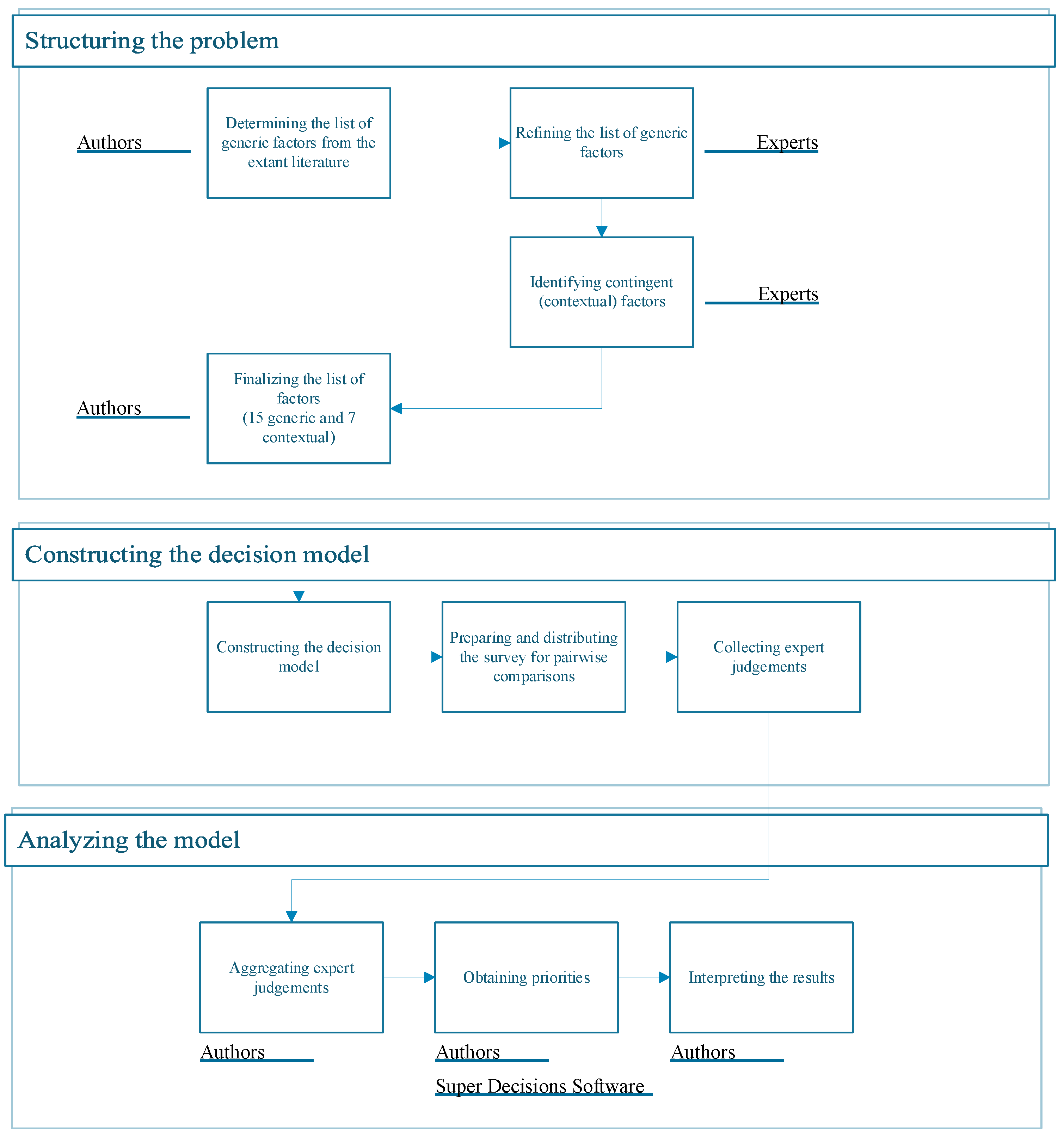
4. Decision Making Framework
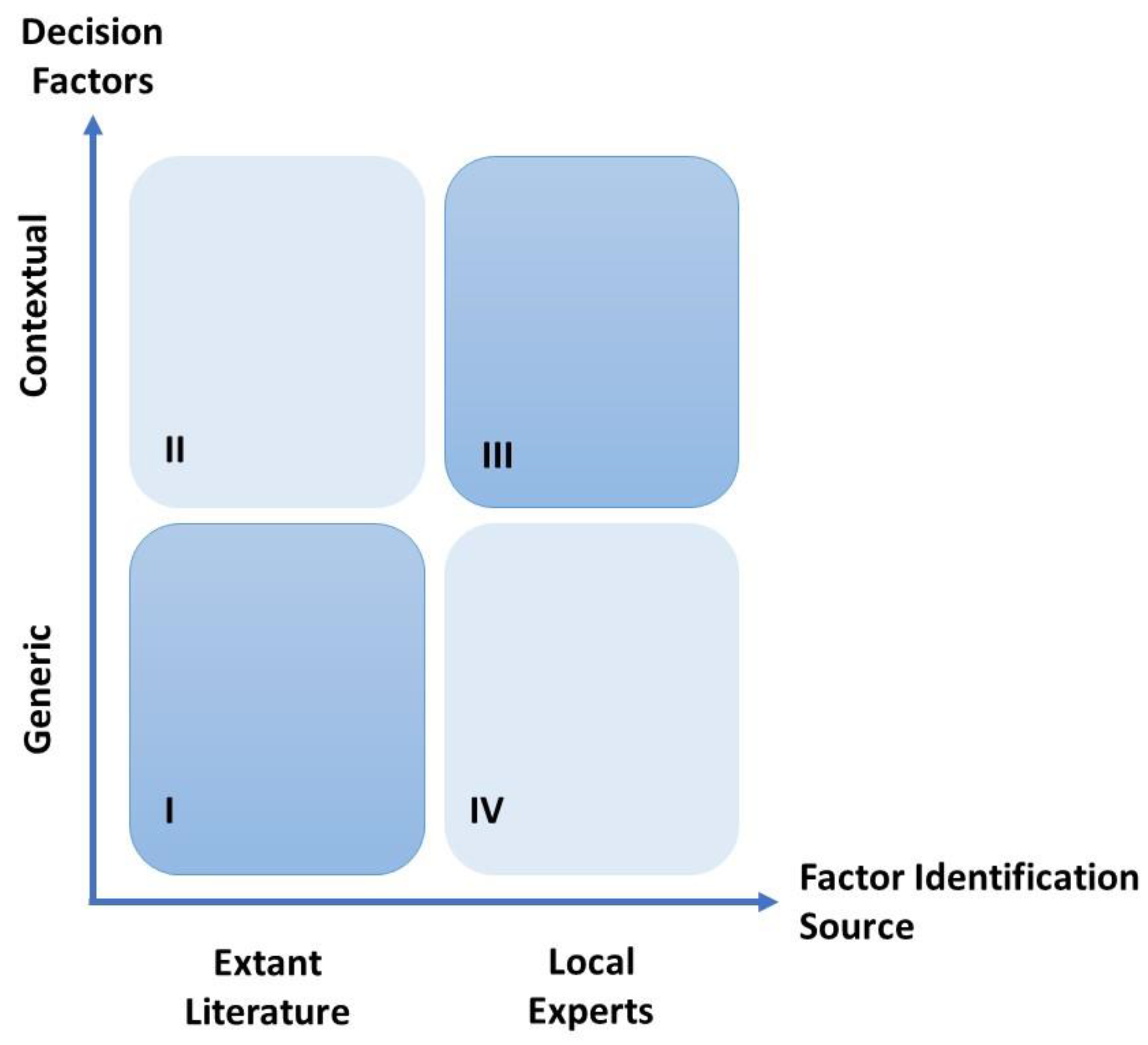
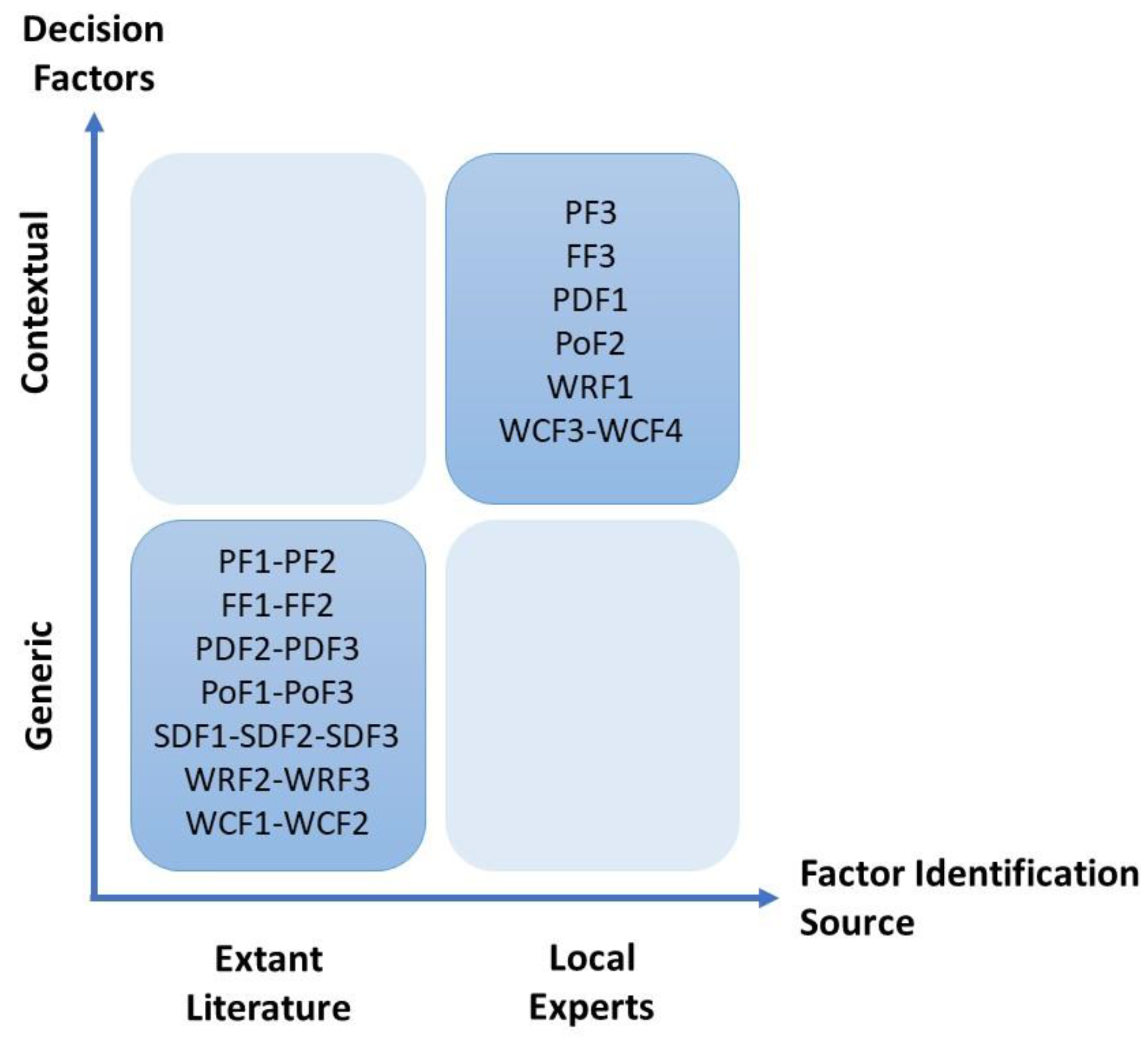
4.1. Structuring the Problem
4.2. Constructing the Decision Model
4.3. Analyzing the Model
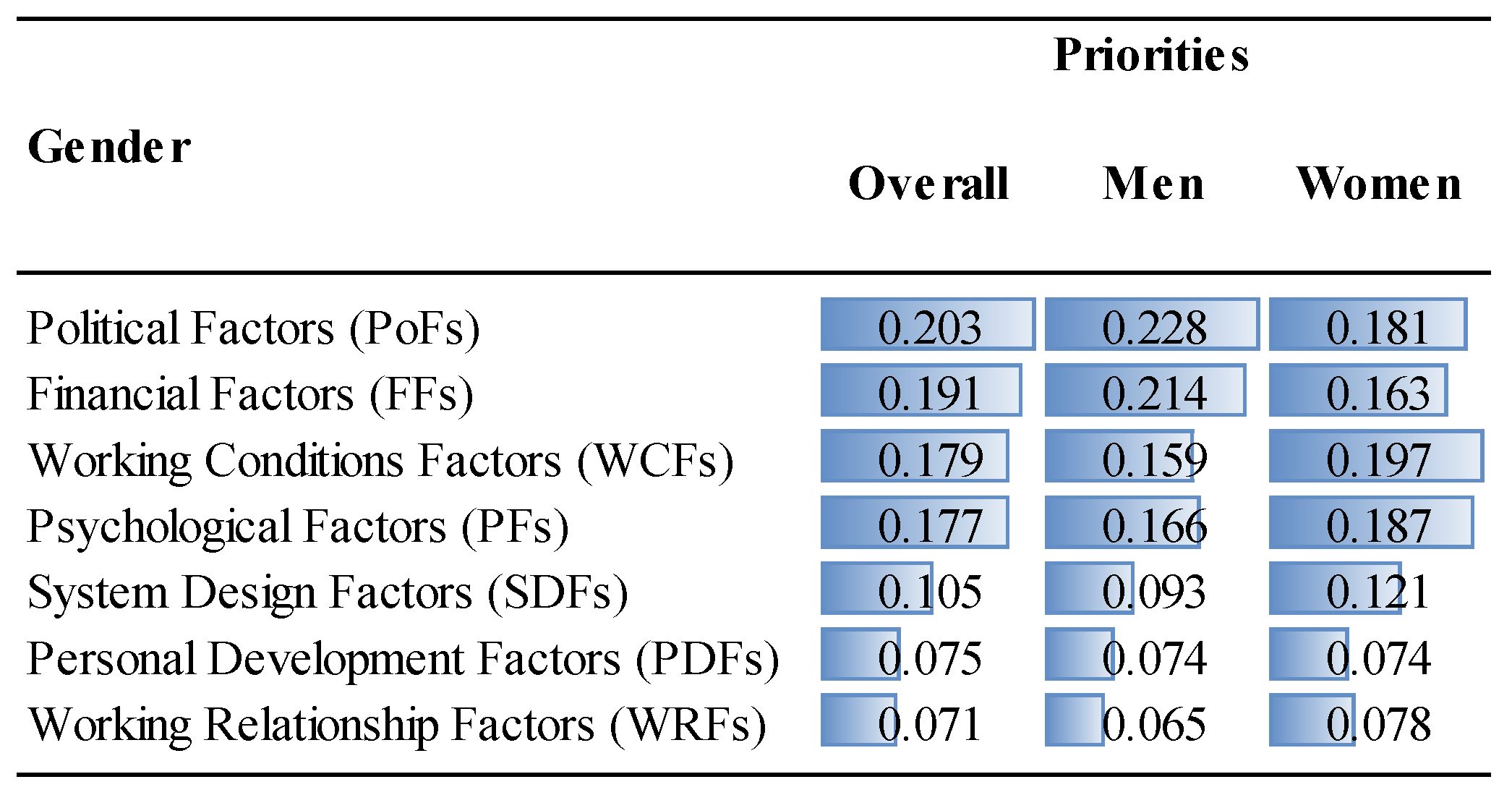
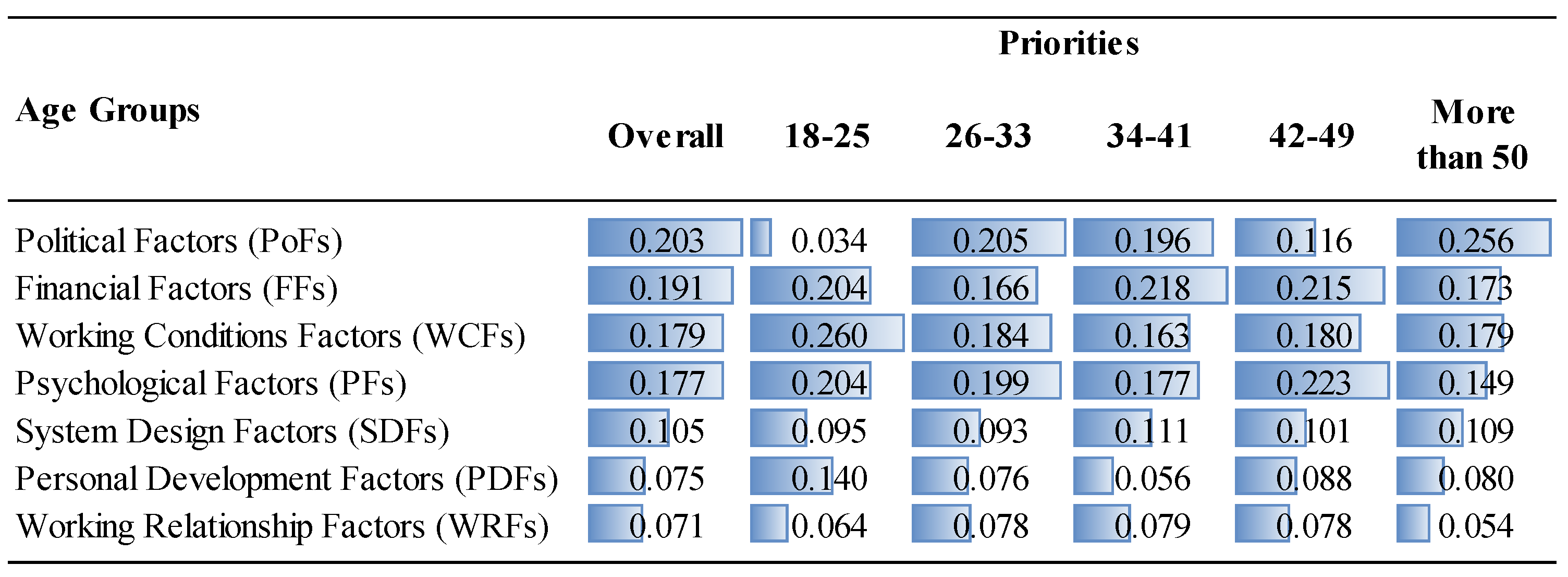
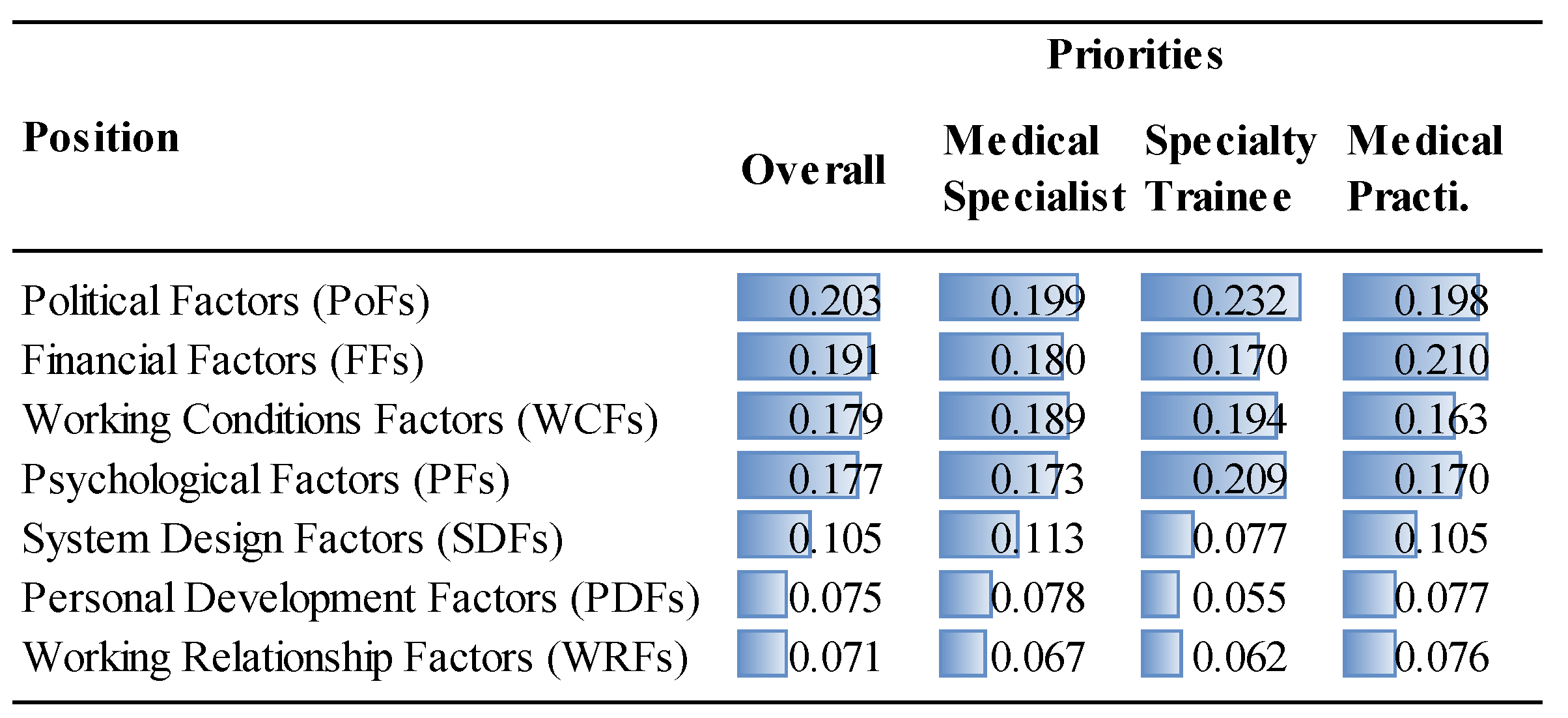
5. Results and Discussion
6. Conclusions and Further Suggestions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Questionnaire
- PART I
- Examining Factors Affecting Emigration Decision of MDs through the Analytic Hierarchy Process
- I agree to participate in the survey
- I disagree to participate in the survey
- Demographic Information
- Please select the option that best describes you:
- ○
- I am a Medical Practitioner
- ○
- I am a Medical Specialist
- ○
- I am a Specialty Trainee
- ○
- I am a Medical Student
- 2.
- Please provide the medical school that you graduated from:
- 3.
- Year of graduation:
- 4.
- Area of specialty: (please indicate if you have not started your specialty training yet)
- 5.
- Please select the option that best describes you:
- ○
- I am currently studying/working abroad.
- ○
- I definitely want to study/work abroad.
- ○
- I want to study/work abroad.
- ○
- I do not want to study/work abroad.
- ○
- I definitely do not want to study/work abroad.
- ○
- I haven’t decided about studying/working abroad yet.
- 6.
- Please provide the medical school at which you are studying:
- 7.
- Please select the option that best describes you:
- ○
- I am currently studying/working abroad.
- ○
- I definitely want to study/work abroad.
- ○
- I want to study/work abroad.
- ○
- I do not want to study/work abroad.
- ○
- I definitely do not want to study/work abroad.
- ○
- I haven’t decided about studying/working abroad yet.
- 8.
- Which country are you in?
- 9.
- At what stage did you decide to study/work abroad?
- ○
- Before medical training
- ○
- During medical training
- ○
- During specialty training
- ○
- After specialty training
- 10.
- How many years have you been abroad?
- 11.
- Select the option that best describes your intention to return to the country:
- ○
- Definitely will not return
- ○
- Probably will not return
- ○
- Indifferent
- ○
- Probably will return
- ○
- Definitely will return
- 12.
- Your age:
- ○
- 18–25
- ○
- 26–33
- ○
- 34–41
- ○
- 42–49
- ○
- 50+
- 13.
- Your gender:
- ○
- Female
- ○
- Male
- ○
- Prefer not to answer
- PART II: Pairwise Comparison Questions
- 1.
- Of the affecting psychological factors, which one affects “emigration decision of MDs” more, and how much more?
| Loss of Professional Reputation | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Personal Security Concerns |
| Personal Security Concerns | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Concerns About Ethical Violations by Colleagues |
| Concerns About Ethical Violations by Colleagues | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Loss of Professional Reputation |
- 2.
- Of the affecting financial factors, which one affects “emigration decision of MDs” more, and how much more?
| Low Remuneration | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Inadequate Performance Payments |
| Inadequate Performance Payments | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Unfair Performance Payments |
| Unfair Performance Payments | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Low Remuneration |
- 3.
- Of the affecting personal development factors, which one affects “emigration decision of MDs” more, and how much more?
| Lack of Research Funds | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Lack of Training and Self-development Areas |
| Lack of Training and Self-development Areas | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Lack of Experience Opportunities |
| Lack of Experience Opportunities | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Lack of Research Funds |
- 4.
- Of the affecting political factors, which one affects “emigration decision of MDs” more and how much more?
| Frustration with the Political Situation | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Anxiety About Their Future due to the Political Situation |
| Anxiety About Their Future due to the Political Situation | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Political Ethics and Transparency Issues |
| Political Ethics and Transparency Issues | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Frustration with the Political Situation |
- 5.
- Of the affecting system design factors, which one affects “emigration decision of MDs” more, and how much more?
| Dysfunctional Healthcare System | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Poor Professional Standards |
| Poor Professional Standards | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Unfair Competition for Promotion and Managerial Positions |
| Unfair Competition for Promotion and Managerial Positions | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Dysfunctional Healthcare System |
- 6.
- Of the affecting working relationship factors, which one affects “emigration decision of MDs” more, and how much more?
| Bullying | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Unsatisfactory Mentorship |
| Unsatisfactory Mentorship | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Distressing Relationships with Peers or Other Healthcare Staff |
| Distressing Relationships with Peers or Other Healthcare Staff | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Bullying |
- 7.
- Of the affecting working conditions factors, which one affects “emigration decision of MDs” more, and how much more?
| Long Working Hours | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Lack of Preventive and Therapeutic Equipment and Healthcare Personnel |
| Lack of Preventive and Therapeutic Equipment and Healthcare Personnel | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Compulsory Service Liability |
| Compulsory Service Liability | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Assignment of Doctors Against Their Will |
| Long Working Hours | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Compulsory Service Liability |
| Lack of Preventive and Therapeutic Equipment and Healthcare Personnel | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Assignment of Doctors Against Their Will |
| Assignment of Doctors Against Their Will | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Long Working Hours |
- 8.
- Of the affecting factors, which one affects “emigration decision of MDs” more, and how much more?
| Psychological Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Financial Factors |
| Financial Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Personal Development Factors |
| Personal Development Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Political Factors |
| Political Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | System Design Factors |
| System Design Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Relationship Factors |
| Working Relationship Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Conditions Factors |
| Psychological Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Personal Development Factors |
| Financial Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Political Factors |
| Personal Development Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | System Design Factors |
| Political Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Relationship Factors |
| System Design Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Conditions Factors |
| Psychological Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Political Factors |
| Financial Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | System Design Factors |
| Personal Development Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Relationship Factors |
| Political Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Conditions Factors |
| Psychological Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | System Design Factors |
| Financial Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Relationship Factors |
| Personal Development Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Conditions Factors |
| Psychological Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Relationship Factors |
| Financial Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Working Conditions Factors |
| Working Conditions Factors | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Psychological Factors |
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pairwise Comparisons (wrt.) | Overall | Current Position | Gender | Emigration Intention | Age | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical Specialist | Specialty Trainee | Pract. | Women | Men | Yes | No | Indiff. | Abroad | 18–25 | 26–33 | 34–41 | 42–49 | >50 | ||
| Goal | 0.44% | 0.68% | 2.58% | 0.62% | 0.84% | 0.55% | 1.03% | 0.55% | 0.65% | 4.13% | 9.46% | 0.62% | 1.12% | 3.33% | 0.56% |
| Psychological Factors | 0.46% | 1.02% | 1.14% | 0.08% | 0.19% | 0.75% | 0.29% | 3.11% | 0.00% | 0.10% | 6.52% | 0.09% | 3.85% | 0.01% | 0.10% |
| Financial Factors | 0.04% | 0.43% | 7.26% | 0.27% | 0.07% | 0.02% | 1.19% | 1.41% | 5.31% | 4.49% | 0.02% | 0.12% | 6.53% | 2.84% | 0.08% |
| Personal Dev. Factors | 0.01% | 1.19% | 2.38% | 0.19% | 0.43% | 0.45% | 0.30% | 2.32% | 0.00% | 0.07% | 0.22% | 0.01% | 0.11% | 3.29% | 1.85% |
| Political Factors | 0.34% | 0.02% | 0.14% | 2.23% | 1.60% | 0.00% | 0.02% | 0.87% | 4.22% | 0.83% | 0.68% | 0.08% | 4.18% | 0.27% | 0.14% |
| System Design Factors | 0.03% | 0.96% | 0.21% | 0.42% | 1.45% | 1.62% | 0.63% | 0.01% | 1.36% | 1.49% | 0.00% | 0.02% | 0.27% | 6.72% | 0.78% |
| Working Rel. Factors | 0.57% | 0.66% | 0.03% | 0.78% | 0.03% | 2.21% | 0.95% | 0.01% | 1.49% | 0.78% | 4.54% | 1.43% | 0.61% | 1.64% | 0.62% |
| Working Cond. Factors | 0.26% | 0.89% | 0.25% | 0.23% | 0.43% | 0.25% | 0.41% | 0.03% | 0.93% | 2.32% | 5.66% | 0.23% | 1.50% | 4.86% | 0.44% |
References
- Byrne, J.-P.; Conway, E.; McDermott, A.M.; Matthews, A.; Prihodova, L.; Costello, R.W.; Humphries, N. How the Organisation of Medical Work Shapes the Everyday Work Experiences Underpinning Doctor Migration Trends: The Case of Irish-Trained Emigrant Doctors in Australia. Health Policy 2021, 125, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R.; Sharma, M.K. Measures of Sustainability in Healthcare. Sustain. Anal. Model. 2021, 1, 100001. [Google Scholar] [CrossRef]
- Akl, E.A.; Maroun, N.; Major, S.; Afif, C.; Chahoud, B.; Choucair, J.; Sakr, M.; Schünemann, H.J. Why Are You Draining Your Brain? Factors Underlying Decisions of Graduating Lebanese Medical Students to Migrate. Soc. Sci. Med. 2007, 64, 1278–1284. [Google Scholar] [CrossRef]
- Botezat, A.; Moraru, A. Brain Drain from Romania: What Do We Know so Far about the Romanian Medical Diaspora? East. J. Eur. Stud. 2020, 11, 309–334. [Google Scholar]
- Gouda, P.; Kitt, K.; Evans, D.S.; Goggin, D.; McGrath, D.; Last, J.; Hennessy, M.; Arnett, R.; O’Flynn, S.; Dunne, F. Ireland’s Medical Brain Drain: Migration Intentions of Irish Medical Students. Hum. Resour. Health 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Humphries, N.; McDermott, A.M.; Conway, E.; Byrne, J.P.; Prihodova, L.; Costello, R.; Matthews, A. ‘Everything Was Just Getting Worse and Worse’: Deteriorating Job Quality as a Driver of Doctor Emigration from Ireland. Hum. Resour. Health 2019, 17, 97. [Google Scholar] [CrossRef] [PubMed]
- Onah, C.K.; Azuogu, B.N.; Ochie, C.N.; Akpa, C.O.; Okeke, K.C.; Okpunwa, A.O.; Bello, H.M.; Ugwu, G.O. Physician Emigration from Nigeria and the Associated Factors: The Implications to Safeguarding the Nigeria Health System. Hum. Resour. Health 2022, 20, 85. [Google Scholar] [CrossRef]
- Sheikh, A.; Naqvi, S.H.A.; Sheikh, K.; Naqvi, S.H.S.; Bandukda, M.Y. Physician Migration at Its Roots: A Study on the Factors Contributing towards a Career Choice Abroad among Students at a Medical School in Pakistan. Glob. Health 2012, 8, 1–11. [Google Scholar] [CrossRef]
- Genc, K. Turkish Doctors Emigrate amid Low Pay and Rising Violence. Lancet 2022, 400, 482–483. [Google Scholar] [CrossRef]
- Türk Tabipleri Birliği @ttborgtr. TTB’ye “İyi Hal Belgesi” Başvuru Sayısı; Aralık Ayında 268, 2022 Yılında 2685 oldu. Image attached. Twitter 2023. Available online: https://twitter.com/ttborgtr/status/1609828230948683782?lang=en (accessed on 12 May 2023).
- Health Resources—Doctors—OECD Data. Available online: http://data.oecd.org/healthres/doctors.htm (accessed on 12 April 2023).
- Demïroğlu, T.; Kilinç, E.; Atay, E. Violence towards Health Professionals: The Case of Kilis City. J. Health Sci. 2015, 24, 49–55. [Google Scholar]
- Devebakan, N. Workplace Violence in Health Care Organizations and Evaluation of “Code White” Application in Dokuz Eylul University Application and Research Hospital. Suleyman Demirel Univ. J. Fac. Econ. Adm. Sci. 2018, 23, 383–399. [Google Scholar]
- Mïlet, M.; Yanik, A. Workplace Violence against Health Workers. Int. J. Health Manag. Strateg. Res. 2017, 3, 25–36. [Google Scholar]
- The Central Bank of Turkey. Available online: https://www.tcmb.gov.tr/wps/wcm/connect/EN/TCMB+EN/Main+Menu/Statistics/Exchange+Rates/Indicative+Exchange+Rates (accessed on 12 April 2023).
- Türk-IS Temmuz 2022. Açlik Ve Yoksulluk Siniri. Available online: https://www.turkis.org.tr/temmuz-aclik-yoksulluk-siniri/ (accessed on 12 April 2023).
- Turkish Medical Association Sağlık Bakanlığı Yeni Ek Ödeme Yönetmeliği: Kâr Odaklı ve Geçici Düzenlemelere Değil, Toplumu Önceleyen Yeni Bir Sağlık Sistemine İhtiyaç Vardır. Available online: https://www.ttb.org.tr/haber_goster.php?Guid=c018f720-1d62-11ed-88fa-ab1256785955 (accessed on 12 April 2023).
- Mu, E.; Cooper, O. A Contingency Approach to Multi-Criteria Decision-Making: A Search for Validity through Rigor and Relevance. In New Perspectives in Operations Research and Management Science: Essays in Honor of Fusun Ulengin; Topcu, Y.I., Onsel Ekici, S., Kabak, O., Aktas, E., Ozaydin, O., Eds.; Springer: Cham, Switzerland, 2022; pp. 499–525. [Google Scholar]
- Nutt, P.C.; Wilson, D.C. Crucial Trends and Issues in Strategic Decision Making. In Handbook of Decision Making; Wiley: West Sussex, UK, 2010; p. 720. [Google Scholar]
- Mintzberg, H.; Raisinghani, D.; Theoret, A. The Structure of” Unstructured” Decision Processes. Adm. Sci. Q. 1976, 21, 246–275. [Google Scholar] [CrossRef]
- Carling, J.; Collins, F. Aspiration, Desire and Drivers of Migration. J. Ethn. Migr. Stud. 2018, 44, 909–926. [Google Scholar] [CrossRef]
- Van Hear, N.; Bakewell, O.; Long, K. Push-Pull plus: Reconsidering the Drivers of Migration. J. Ethn. Migr. Stud. 2018, 44, 927–944. [Google Scholar] [CrossRef]
- Domagała, A.; Kulbat, A.; Parzonka, K. Emigration from the Perspective of Polish Health Professionals–Insights from a Qualitative Study. Front. Public Health 2022, 10, 1075728. [Google Scholar] [CrossRef] [PubMed]
- Lawal, L.; Lawal, A.O.; Amosu, O.P.; Muhammad-Olodo, A.O.; Abdulrasheed, N.; Abdullah, K.-R.; Kuza, P.B.; Aborode, A.T.; Adebisi, Y.A.; Kareem, A.A. The COVID-19 Pandemic and Health Workforce Brain Drain in Nigeria. Int. J. Equity Health 2022, 21, 174. [Google Scholar] [CrossRef]
- Stilwell, B.; Diallo, K.; Zurn, P.; Vujicic, M.; Adams, O.; Dal Poz, M. Migration of Health-Care Workers from Developing Countries: Strategic Approaches to Its Management. Bull. World Health Organ. 2004, 82, 595–600. [Google Scholar]
- Diallo, K. Data on the Migration of Health-Care Workers: Sources, Uses, and Challenges. Bull. World Health Organ. 2004, 82, 601–607. [Google Scholar]
- Mu, E.; Stern, H. A Contingent/Assimilation Framework for Public Interorganizational Systems Decisions: Should the City of Pittsburgh and Allegheny County Consolidate Information Technology Services? Int. J. Inf. Technol. Decis. Mak. 2018, 17, 1611–1658. [Google Scholar] [CrossRef]
- Saaty, T.L. Decision Making for Leaders: The Analytical Hierarchy Process; McGraw-Hill: New York, NY, USA, 1980; ISBN 0-534-97959-9. [Google Scholar]
- Ishizaka, A.; Mu, E. What Is so Special about the Analytic Hierarchy and Network Process? Ann. Oper. Res. 2023, 326, 625–634. [Google Scholar] [CrossRef]
- Saaty, T.L. Fundamentals of Decision Making and Priority Theory with the Analytic Hierarchy Process; RWS Publications: Pittsburgh, PA, USA, 2000. [Google Scholar]
- Ishizaka, A.; Nemery, P. Multi-Criteria Decision Analysis: Methods and Software; John Wiley & Sons: West Sussex, UK, 2013; ISBN 978-1-119-97407-9. [Google Scholar]
- Saaty, T.L. Decision Making with Dependence and Feedback: The Analytic Network Process; RWS Publications: Pittsburgh, PA, USA, 1996. [Google Scholar]
- Kabbash, I.; El-Sallamy, R.; Zayed, H.; Alkhyate, I.; Omar, A.; Abdo, S. The Brain Drain: Why Medical Students and Young Physicians Want to Leave Egypt. East. Mediterr. Health J. 2021, 27, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Turkey Ministry of Health. 2017 Annual Report; The Ministry of Health: Ankara, Turkey, 2018. [Google Scholar]
- Turkey Ministry of Health. 2021 Annual Report; The Ministry of Health: Ankara, Turkey, 2022. [Google Scholar]
- Shi, L.; Li, G.; Hao, J.; Wang, W.; Chen, W.; Liu, S.; Yu, Z.; Shi, Y.; Ma, Y.; Fan, L. Psychological Depletion in Physicians and Nurses Exposed to Workplace Violence: A Cross-Sectional Study Using Propensity Score Analysis. Int. J. Nurs. Stud. 2020, 103, 103493. [Google Scholar] [CrossRef] [PubMed]
- International Labour Office ILO. Framework Guidelines for Addressing Workplace Violence in the Health Sector; International Council of Nurses ICN: Geneva, Switzerland; World Health Organization WHO: Geneva, Switzerland; Public Services International PSI: Geneva, Switzerland, 2002. [Google Scholar]
- The Centre for Assessment, Selection and Placement. Available online: https://www.osym.gov.tr/TR,23885/2022-yuksekogretim-kurumlari-sinavi-yks-yuksekogretim-programlari-ve-kontenjanlari-kilavuzu.html (accessed on 15 February 2023).
- Turkey Ministry of Health. The Ministry of Health Payment Regulation; The Ministry of Health: Ankara, Turkey, 2022. [Google Scholar]
- The Presidency of the Republic of Turkey, Legislation Information System. Available online: https://www.mevzuat.gov.tr/mevzuat?MevzuatNo=3359&MevzuatTur=1&MevzuatTertip=5 (accessed on 19 February 2023).
- Zoho Survey. Available online: https://www.zoho.com/survey/index.html (accessed on 12 May 2022).
- Saaty, T.L.; Peniwati, K. Group Decision Making: Drawing out and Reconciling Differences; RWS Publications: Pittsburgh, PA, USA, 2007; ISBN 978-1-888603-08-8. [Google Scholar]
- Migration and Home Affairs. Available online: https://home-affairs.ec.europa.eu/networks/european-migration-network-emn/emn-asylum-and-migration-glossary/glossary/emigration_en (accessed on 12 May 2023).
- Carling, J. Migration in the Age of Involuntary Immobility: Theoretical Reflections and Cape Verdean Experiences. J. Ethn. Migr. Stud. 2002, 28, 5–42. [Google Scholar] [CrossRef]
- Carling, J.; Schewel, K. Revisiting Aspiration and Ability in International Migration. J. Ethn. Migr. Stud. 2018, 44, 945–963. [Google Scholar] [CrossRef]
- Incekas, A.B.; Kadaifci, C. Brain Drain: A Multi-Criteria Decision Model. In Proceedings of the Industrial Engineering in the Internet-of-Things World: Selected Papers from the Virtual Global Joint Conference on Industrial Engineering and Its Application Areas, GJCIE 2020, Antalya, Turkey, 14–15 August 2020; Calisir, F., Ed.; Springer: Cham, Switzerland, 2022; pp. 271–282, ISBN 3-030-76723-X. [Google Scholar]
- Al Husein, N.; Wagner, N. Determinants of Intended Return Migration among Refugees: A Comparison of Syrian Refugees in Germany and Turkey. Int. Migr. Rev. 2023, 57, 1771–1805. [Google Scholar] [CrossRef]
- Mensah, J.; Owusu Ansah, A. Reflections on Return Migration: Understanding How African Immigrants in Canada Contemplate Return. Int. Migr. 2022, 60, 198–216. [Google Scholar] [CrossRef]
- De Haas, H.; Fokkema, T.; Fihri, M.F. Return Migration as Failure or Success? The Determinants of Return Migration Intentions among Moroccan Migrants in Europe. J. Int. Migr. Integr. 2015, 16, 415–429. [Google Scholar] [CrossRef]
- Super Decisions Software. Available online: https://www.superdecisions.com/ (accessed on 22 February 2023).
- Creative Decisions Foundation. Available online: https://www.creativedecisions.net/resources/ (accessed on 8 May 2023).
- Tüketici Fiyat Endeksi, Aralık 2022. Available online: https://data.tuik.gov.tr/Bulten/Index?p=Tuketici-Fiyat-Endeksi-Aralik-2022-49651 (accessed on 23 February 2023).
- ENAGRUP—Enflasyon Araştırma Grubu. Available online: https://enagrup.org/ (accessed on 23 February 2023).
- Kaya, R.R.; Alkan, A. A Study on The Proile of Physicians Who Work in Administrative Positions in the Public Hospitals in Turkey. Manisa Celal Bayar Univ. J. Inst. Health Sci. 2021, 8, 254–262. [Google Scholar] [CrossRef]
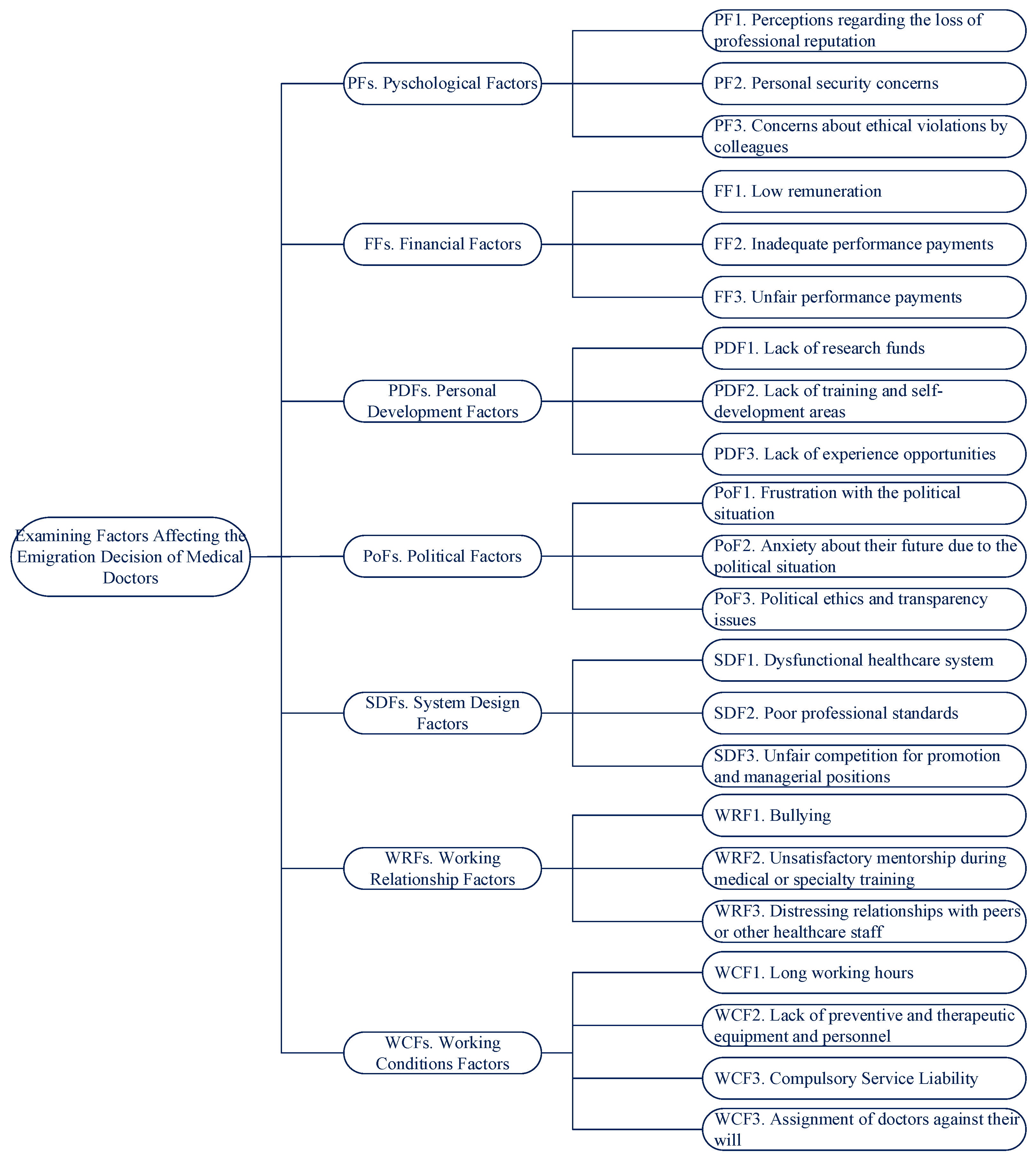


| ID | Factors | Sources | |
|---|---|---|---|
| Psychological Factors (PFs) | PF1 | Perceptions regarding the loss of professional reputation | [8] |
| PF2 | Personal security concerns (violence and harassment) | [3] | |
| PF3 | Concerns about ethical violations by colleagues | Experts | |
| Financial Factors (FFs) | FF1 | Low remuneration | [3,4,5,6,7,8,23,24,25,26] |
| FF2 | Inadequate performance payments | [26] | |
| FF3 | Unfair performance payments | Experts | |
| Personal Development Factors (PDFs) | PDF1 | Lack of research funds (research projects, conference participation, etc.) | Experts |
| PDF2 | Lack of training and self-development | [3,4,5,7,26] | |
| PDF3 | Lack of experience opportunities | [5,25] | |
| Political Factors (PoFs) | PoF1 | Frustration with the political situation | [3,7] |
| PoF2 | Anxiety about their future | Experts | |
| PoF3 | Political ethics and transparency issues | [3] | |
| System Design Factors (SDFs) | SDF1 | Dysfunctional healthcare system | [3] |
| SDF2 | Poor professional standards | [3] | |
| SDF3 | Unfair competition for promotion and managerial positions | [3] | |
| Working Relationship Factors (WRFs) | WRF1 | Bullying | Experts |
| WRF2 | Unsatisfactory mentorship during medical or specialty training | [3] | |
| WRF3 | Distressing relationships with peers or other healthcare staff | [3] | |
| Working Conditions Factors (WCFs) | WCF1 | Long working hours | [3,6,8,24] |
| WCF2 | Lack of preventive and therapeutic equipment and healthcare personnel | [3,4,24] | |
| WCF3 | Compulsory service liability | Experts | |
| WCF4 | Assignment of doctors against their will (inability of medical practitioners to choose the unit where they will work, etc.) | Experts |
| Frequency | % | |
|---|---|---|
| Gender | ||
| Female | 41 | 56.16% |
| Male | 32 | 43.84% |
| Age | ||
| 18–25 | 3 | 4.11% |
| 26–33 | 28 | 38.36% |
| 34–41 | 15 | 20.55% |
| 42–49 | 4 | 5.48% |
| ≥50 | 23 | 31.51% |
| Year of Graduation | ||
| Before 1980 | 1 | 1.37% |
| 1980–1989 | 6 | 8.22% |
| 1990–1999 | 17 | 23.29% |
| 2000–2009 | 6 | 8.22% |
| 2010–2019 | 36 | 49.32% |
| After 2020 | 7 | 9.59% |
| Current Position | ||
| Specialty Trainee | 9 | 12.33% |
| Medical Practitioner | 33 | 45.21% |
| Medical Specialist | 31 | 42.47% |
| Emigration Intention | ||
| I definitely do not want to study/work abroad. | 6 | 8.22% |
| I do not want to study/work abroad. | 11 | 15.07% |
| I want to study/work abroad. | 20 | 27.40% |
| I definitely want to study/work abroad. | 16 | 21.92% |
| I haven’t decided about studying/working abroad yet. | 17 | 23.29% |
| I am currently studying/working abroad. | 3 | 4.11% |
| Area of Specialty | # | % |
|---|---|---|
| Family Medicine | 4 | 10.00% |
| Gynecology and Obstetrics | 4 | 10.00% |
| General Surgery | 3 | 7.50% |
| Anesthesiology and Reanimation | 2 | 5.00% |
| ENT (Ear, Nose, and Throat) | 2 | 5.00% |
| Ophthalmology | 2 | 5.00% |
| Pediatric Health and Diseases | 2 | 5.00% |
| Psychiatry | 2 | 5.00% |
| Cardiology | 1 | 2.50% |
| Chest Diseases | 1 | 2.50% |
| Emergency Medicine | 1 | 2.50% |
| Endocrinology | 1 | 2.50% |
| Forensic Medicine | 1 | 2.50% |
| Hematology | 1 | 2.50% |
| Infectious Diseases | 1 | 2.50% |
| Internal Medicine | 1 | 2.50% |
| Neurology | 1 | 2.50% |
| Neurosurgery | 1 | 2.50% |
| Orthopedics | 1 | 2.50% |
| Pediatric Surgery | 1 | 2.50% |
| Physical Therapy and Rehabilitation | 1 | 2.50% |
| Plastic, Reconstructive and Aesthetic Surgery | 1 | 2.50% |
| Public Health | 1 | 2.50% |
| Thoracic Surgery | 1 | 2.50% |
| Urology | 1 | 2.50% |
| Not Available | 2 | 5.00% |
| Total | 40 | 100.00% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadaifci, C.; Topcu, Y.I.; Mu, E. An Analytic Hierarchy Process Contingency Analysis of Factors Affecting the Emigration Decision of Medical Doctors in Turkey. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 623-647. https://doi.org/10.3390/ejihpe14030041
Kadaifci C, Topcu YI, Mu E. An Analytic Hierarchy Process Contingency Analysis of Factors Affecting the Emigration Decision of Medical Doctors in Turkey. European Journal of Investigation in Health, Psychology and Education. 2024; 14(3):623-647. https://doi.org/10.3390/ejihpe14030041
Chicago/Turabian StyleKadaifci, Cigdem, Y. Ilker Topcu, and Enrique Mu. 2024. "An Analytic Hierarchy Process Contingency Analysis of Factors Affecting the Emigration Decision of Medical Doctors in Turkey" European Journal of Investigation in Health, Psychology and Education 14, no. 3: 623-647. https://doi.org/10.3390/ejihpe14030041
APA StyleKadaifci, C., Topcu, Y. I., & Mu, E. (2024). An Analytic Hierarchy Process Contingency Analysis of Factors Affecting the Emigration Decision of Medical Doctors in Turkey. European Journal of Investigation in Health, Psychology and Education, 14(3), 623-647. https://doi.org/10.3390/ejihpe14030041