

The Effect of Digital Mindfulness Interventions on Depressive, Anxiety, and Stress Symptoms in Pregnant Women: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
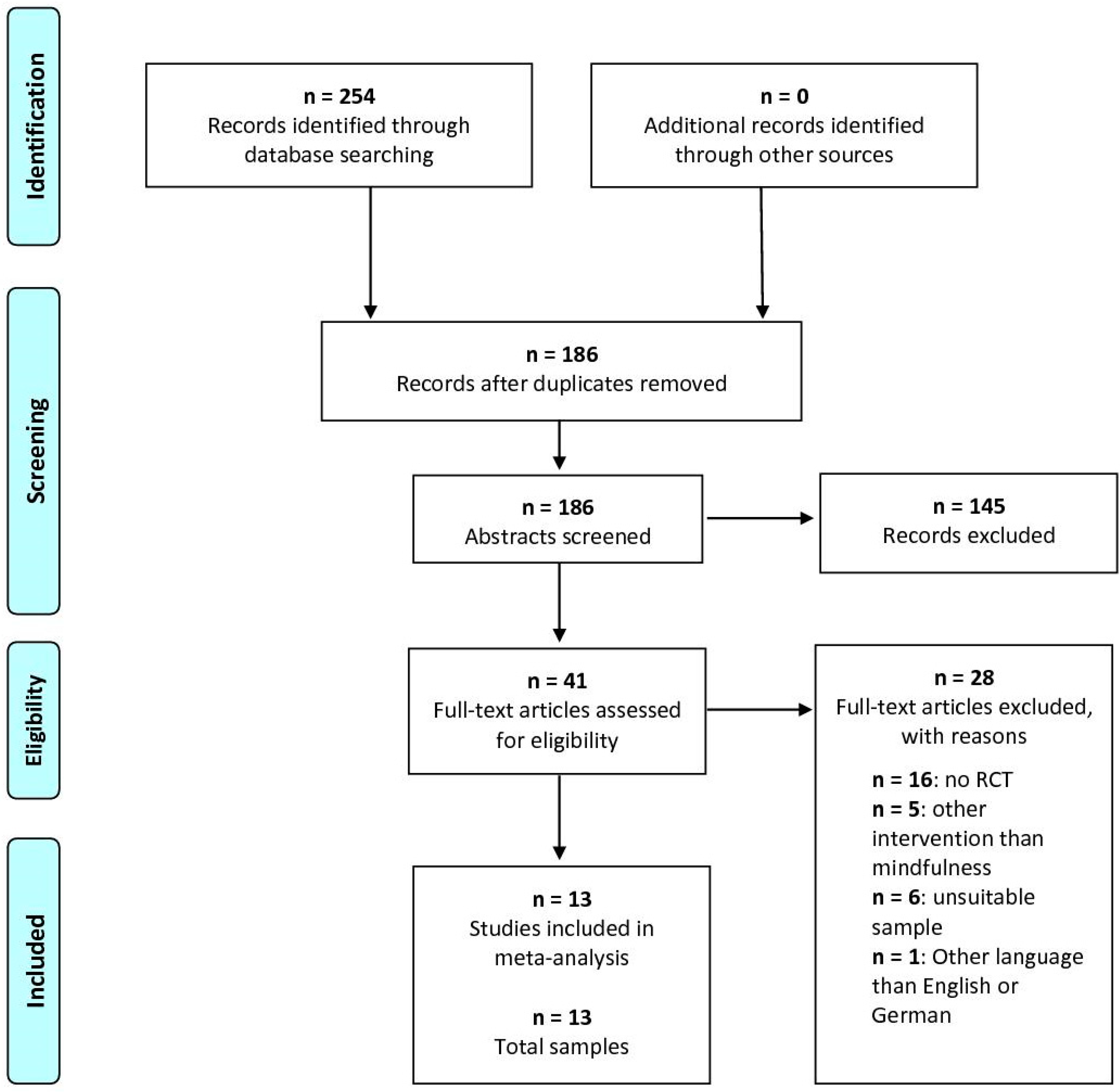
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Eligible Studies
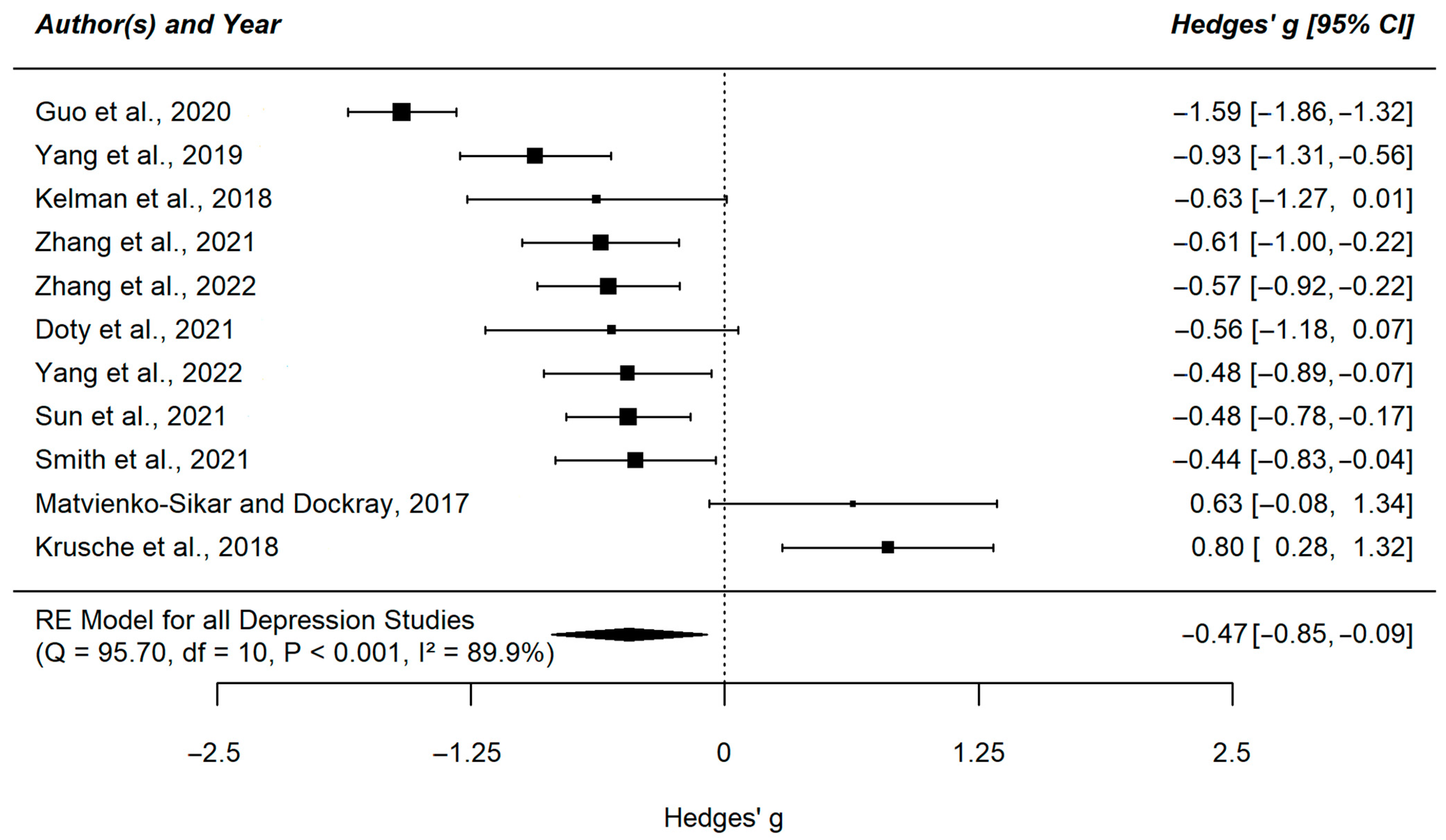
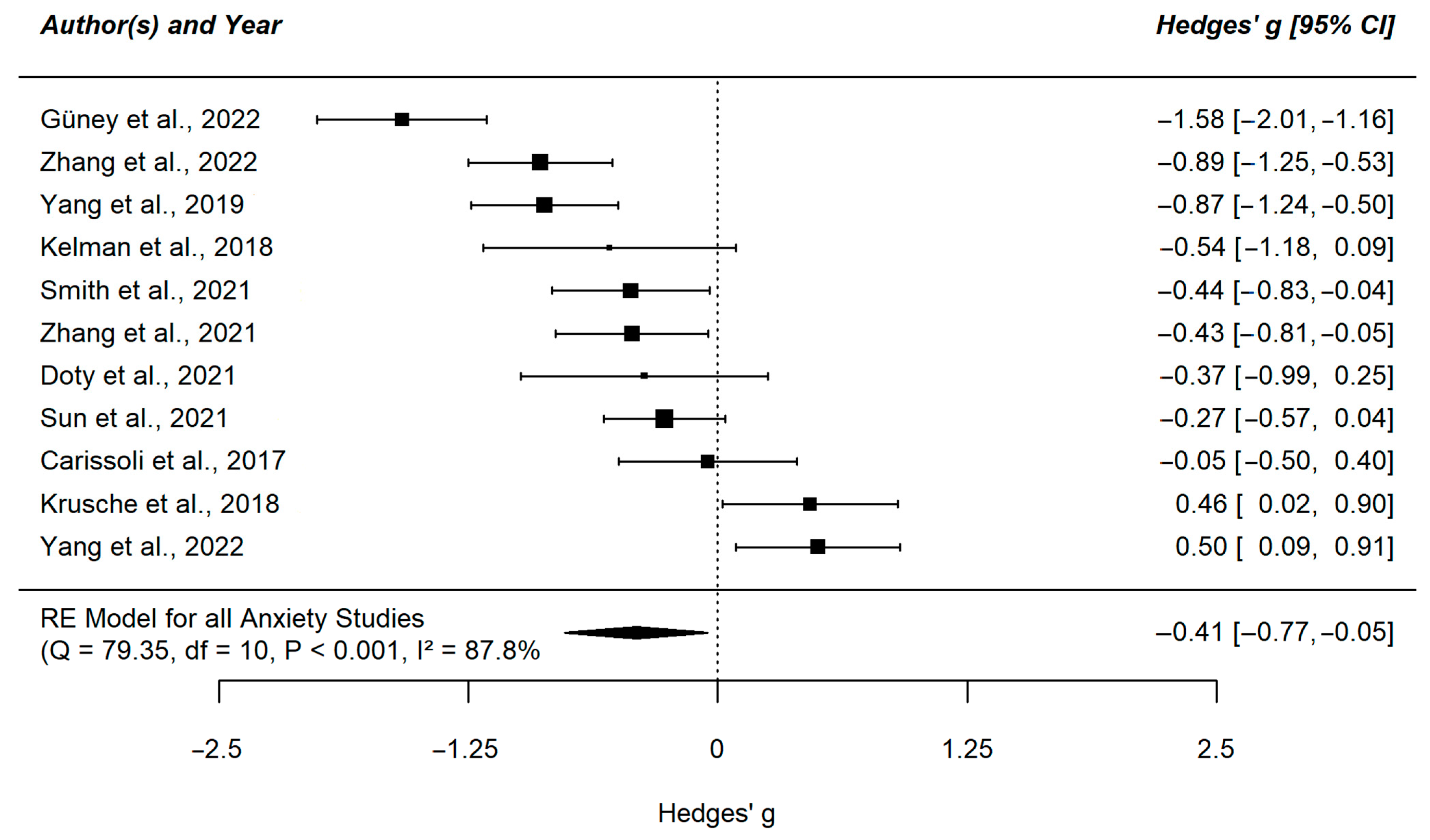
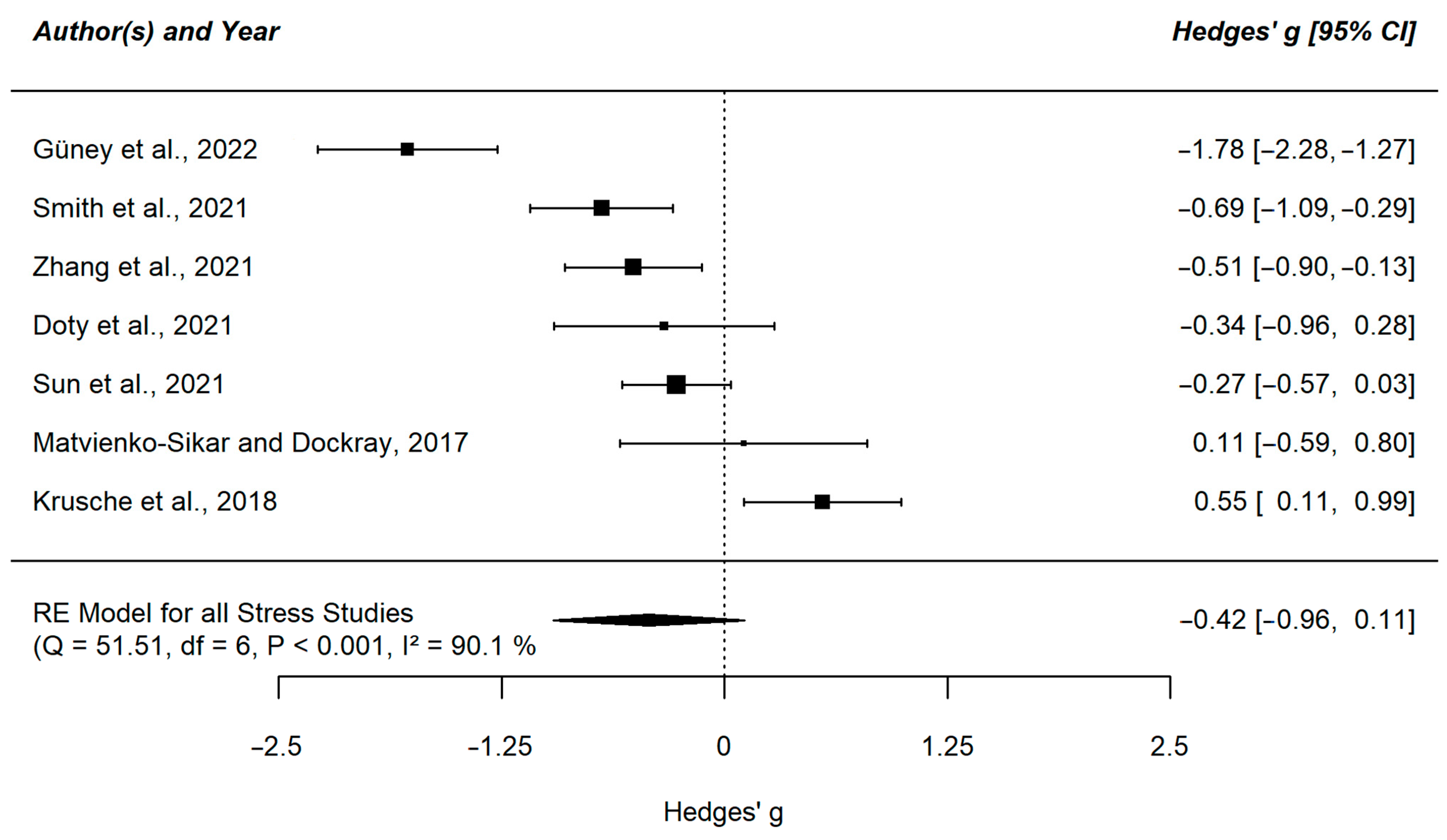
3.2. Meta-Analytic Results
3.3. Meta-Regression and Subgroup Analyses
3.4. Risk of Bias
3.5. Small Study Effects and Sensitivity Analyses
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Fairbrother, N.; Young, A.H.; Janssen, P.; Antony, M.M.; Tucker, E. Depression and anxiety during the perinatal period. BMC Psychiatry 2015, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Stone, S.L.; Diop, H.; Declercq, E.; Cabral, H.J.; Fox, M.P.; Wise, L.A. Stressful events during pregnancy and postpartum depressive symptoms. J. Women’s Health 2015, 24, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Agius, A.; Xuereb, R.B.; Carrick-Sen, D.; Sultana, R.; Rankin, J. The co-existence of depression, anxiety and post-traumatic stress symptoms in the perinatal period: A systematic review. Midwifery 2016, 36, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Lilliecreutz, C.; Larén, J.; Sydsjö, G.; Josefsson, A. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth 2016, 16, 5. [Google Scholar] [CrossRef]
- van Niel, M.S.; Payne, J.L. Perinatal depression: A review. Clevel. Clin. J. Med. 2020, 87, 273–277. [Google Scholar] [CrossRef]
- Baibazarova, E.; van de Beek, C.; Cohen-Kettenis, P.T.; Buitelaar, J.; Shelton, K.H.; van Goozen, S.H.M. Influence of prenatal maternal stress, maternal plasma cortisol and cortisol in the amniotic fluid on birth outcomes and child temperament at 3 months. Psychoneuroendocrinology 2013, 38, 907–915. [Google Scholar] [CrossRef]
- Davis, E.P.; Glynn, L.M.; Schetter, C.D.; Hobel, C.; Chicz-Demet, A.; Sandman, C.A. Prenatal exposure to maternal depression and cortisol influences infant temperament. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 737–746. [Google Scholar] [CrossRef]
- Huizink, A.C.; Medina, P.G.R.d.; Mulder, E.J.H.; Visser, G.H.A.; Buitelaar, J.K. Psychological measures of prenatal stress as predictors of infant temperament. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 1078–1085. [Google Scholar] [CrossRef]
- Lenz, B.; Müller, C.P.; Stoessel, C.; Sperling, W.; Biermann, T.; Hillemacher, T.; Bleich, S.; Kornhuber, J. Sex hormone activity in alcohol addiction: Integrating organizational and activational effects. Prog. Neurobiol. 2012, 96, 136–163. [Google Scholar] [CrossRef]
- Lenz, B.; Röther, M.; Bouna-Pyrrou, P.; Mühle, C.; Tektas, O.Y.; Kornhuber, J. The androgen model of suicide completion. Prog. Neurobiol. 2019, 172, 84–103. [Google Scholar] [CrossRef] [PubMed]
- Nolvi, S.; Karlsson, L.; Bridgett, D.J.; Korja, R.; Huizink, A.C.; Kataja, E.-L.; Karlsson, H. Maternal prenatal stress and infant emotional reactivity six months postpartum. J. Affect. Disord. 2016, 199, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.; Pearson, R.M.; Goodman, S.H.; Rapa, E.; Rahman, A.; McCallum, M.; Howard, L.M.; Pariante, C.M. Effects of perinatal mental disorders on the fetus and child. Lancet 2014, 384, 1800–1819. [Google Scholar] [CrossRef] [PubMed]
- Talge, N.M.; Neal, C.; Glover, V. Antenatal maternal stress and long-term effects on child neurodevelopment: How and why? J. Child Psychol. Psychiatry Allied Discip. 2007, 48, 245–261. [Google Scholar] [CrossRef]
- Forsell, E.; Bendix, M.; Holländare, F.; Szymanska von Schultz, B.; Nasiell, J.; Blomdahl-Wetterholm, M.; Eriksson, C.; Kvarned, S.; van der Lindau Linden, J.; Söderberg, E.; et al. Internet delivered cognitive behavior therapy for antenatal depression: A andomized controlled trial. J. Affect. Disord. 2017, 221, 56–64. [Google Scholar] [CrossRef]
- Green, S.M.; Donegan, E.; McCabe, R.E.; Streiner, D.L.; Agako, A.; Frey, B.N. Cognitive behavioral therapy for perinatal anxiety: A randomized controlled trial. Aust. N. Z. J. Psychiatry 2020, 54, 423–432. [Google Scholar] [CrossRef]
- Loughnan, S.A.; Sie, A.; Hobbs, M.J.; Joubert, A.E.; Smith, J.; Haskelberg, H.; Mahoney, A.E.J.; Kladnitski, N.; Holt, C.J.; Milgrom, J.; et al. A randomized controlled trial of ‘MUMentum Pregnancy’: Internet-delivered cognitive behavioral therapy program for antenatal anxiety and depression. J. Affect. Disord. 2019, 243, 381–390. [Google Scholar] [CrossRef]
- Bright, K.S.; Charrois, E.M.; Mughal, M.K.; Wajid, A.; McNeil, D.; Stuart, S.; Hayden, K.A.; Kingston, D. Interpersonal Psychotherapy to Reduce Psychological Distress in Perinatal Women: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8421. [Google Scholar] [CrossRef]
- Grote, N.K.; Swartz, H.A.; Geibel, S.L.; Zuckoff, A.; Houck, P.R.; Frank, E. A randomized controlled trial of culturally relevant, brief interpersonal psychotherapy for perinatal depression. Psychiatr. Serv. 2009, 60, 313–321. [Google Scholar] [CrossRef]
- Spinelli, M.G. Interpersonal psychotherapy for depressed antepartum women: A pilot study. Am. J. Psychiatry 1997, 154, 1028–1030. [Google Scholar] [CrossRef]
- Chan, K.L.; Leung, W.C.; Tiwari, A.; Or, K.L.; Ip, P. Using Smartphone-Based Psychoeducation to Reduce Postnatal Depression Among First-Time Mothers: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e12794. [Google Scholar] [CrossRef]
- Haga, S.M.; Drozd, F.; Lisøy, C.; Wentzel-Larsen, T.; Slinning, K. Mamma Mia—A randomized controlled trial of an internet-based intervention for perinatal depression. Psychol. Med. 2019, 49, 1850–1858. [Google Scholar] [CrossRef]
- Shen, Q.; Huang, C.-R.; Rong, L.; Ju, S.; Redding, S.R.; Ouyang, Y.-Q.; Wang, R. Effects of needs-based education for prenatal anxiety in advanced multiparas: A randomized controlled trial. BMC Pregnancy Childbirth 2022, 22, 301. [Google Scholar] [CrossRef] [PubMed]
- Bonacquisti, A.; Cohen, M.J.; Schiller, C.E. Acceptance and commitment therapy for perinatal mood and anxiety disorders: Development of an inpatient group intervention. Arch. Women’s Ment. Health 2017, 20, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Vakilian, K.; Zarei, F.; Majidi, A. Effect of Acceptance and Commitment Therapy (ACT) on Anxiety and Quality of Life During Pregnancy: A Mental Health Clinical Trial Study. Iran. Red Crescent Med. J. 2019, 21, e89489. [Google Scholar] [CrossRef]
- Waters, C.S.; Annear, B.; Flockhart, G.; Jones, I.; Simmonds, J.R.; Smith, S.; Traylor, C.; Williams, J.F. Acceptance and Commitment Therapy for perinatal mood and anxiety disorders: A feasibility and proof of concept study. Br. J. Clin. Psychol. 2020, 59, 461–479. [Google Scholar] [CrossRef]
- Callanan, F.; Tuohy, T.; Bright, A.-M.; Grealish, A. The effectiveness of psychological interventions for pregnant women with anxiety in the antenatal period: A systematic review. Midwifery 2022, 104, 103169. [Google Scholar] [CrossRef] [PubMed]
- Lever Taylor, B.; Cavanagh, K.; Strauss, C. The Effectiveness of Mindfulness-Based Interventions in the Perinatal Period: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0155720. [Google Scholar] [CrossRef] [PubMed]
- Neo, H.S.; Tan, J.H.; Ang, W.H.D.; Lau, Y. Internet-delivered psychological interventions for reducing depressive, anxiety symptoms and fear of childbirth in pregnant women: A meta-analysis and meta-regression. J. Psychosom. Res. 2022, 157, 110790. [Google Scholar] [CrossRef]
- Silang, K.A.; Sohal, P.R.; Bright, K.S.; Leason, J.; Roos, L.; Lebel, C.; Giesbrecht, G.F.; Tomfohr-Madsen, L.M. eHealth Interventions for Treatment and Prevention of Depression, Anxiety, and Insomnia during Pregnancy: Systematic Review and Meta-analysis. JMIR Ment. Health 2022, 9, e31116. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Coming to Our Senses: Healing Ourselves and the World through Mindfulness; Hachette: London, UK, 2005. [Google Scholar]
- Andersson, G. Internet interventions: Past, present and future. Internet Interv. 2018, 12, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.; Van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.L.; et al. Internet- and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health: A report of the efpa e-health taskforce. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Chen, Z.; Jiang, J.; Hu, T.; Luo, L.; Chen, C.; Xiang, W. The effect of mindfulness-based stress reduction therapy on maternal anxiety, depression, and sleep quality: A protocol for systematic review and meta-analysis. Medicine 2022, 101, e28849. [Google Scholar] [CrossRef]
- Dhillon, A.; Sparkes, E.; Duarte, R.V. Mindfulness-Based Interventions During Pregnancy: A Systematic Review and Meta-analysis. Mindfulness 2017, 8, 1421–1437. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Wu, Y.; Li, H. Effect of mindfulness-based interventions on mental health of perinatal women with or without current mental health issues: A systematic review and meta-analysis of randomized controlled trials. J. Affect. Disord. 2022, 305, 102–114. [Google Scholar] [CrossRef]
- Mao, F.; Sun, Y.; Li, Y.; Cui, N.; Cao, F. Internet-delivered mindfulness-based interventions for mental health outcomes among perinatal women: A systematic review. Asian J. Psychiatry 2023, 80, 103321. [Google Scholar] [CrossRef]
- Moshe, I.; Terhorst, Y.; Philippi, P.; Domhardt, M.; Cuijpers, P.; Cristea, I.; Pulkki-Råback, L.; Baumeister, H.; Sander, L.B. Digital interventions for the treatment of depression: A meta-analytic review. Psychol. Bull. 2021, 147, 749–786. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 25 October 2021).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Greenfield, B.L.; Roos, C.; Hagler, K.J.; Stein, E.; Bowen, S.; Witkiewitz, K.A. Race/ethnicity and racial group composition moderate the effectiveness of mindfulness-based relapse prevention for substance use disorder. Addict. Behav. 2018, 81, 96–103. [Google Scholar] [CrossRef]
- Greeson, J.M.; McBride, E.E.; Chin, G.R.; Lee, H.H.; Colangelo, A.P. Trait mindfulness and mind-body health in students: The role of gender, race, and ethnicity. J. Am. Coll. Health 2022, 1–12. [Google Scholar] [CrossRef]
- Bauer, A.E.; Liu, X.; Byrne, E.M.; Sullivan, P.F.; Wray, N.R.; Agerbo, E.; Nyegaard, M.; Grove, J.; Musliner, K.L.; Ingstrup, K.G.; et al. Genetic risk scores for major psychiatric disorders and the risk of postpartum psychiatric disorders. Transl. Psychiatry 2019, 9, 288. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Carissoli, C.; Gasparri, D.; Riva, G.; Villani, D. Mobile well-being in pregnancy: Suggestions from a quasi-experimental controlled study. Behav. Inf. Technol. 2022, 41, 1639–1651. [Google Scholar] [CrossRef]
- Doty, M.S.; Chen, H.-Y.; Ajishegiri, O.; Sibai, B.M.; Blackwell, S.C.; Chauhan, S.P. 251 Mindful meditation for anxiety in individuals admitted to the antepartum unit: A randomized controlled trial. Am. J. Obstet. Gynecol. 2021, 224, S166. [Google Scholar] [CrossRef]
- Güney, E.; Cengizhan, S.Ö.; Karataş Okyay, E.; Bal, Z.; Uçar, T. Effect of the Mindfulness-Based Stress Reduction program on stress, anxiety, and childbirth fear in pregnant women diagnosed with COVID-19. Complement. Ther. Clin. Pract. 2022, 47, 101566. [Google Scholar] [CrossRef]
- Guo, L.; Zhang, J.; Mu, L.; Ye, Z. Preventing Postpartum Depression with Mindful Self-Compassion Intervention: A Randomized Control Study. J. Nerv. Ment. Dis. 2020, 208, 101–107. [Google Scholar] [CrossRef]
- Kelman, A.R.; Evare, B.S.; Barrera, A.Z.; Muñoz, R.F.; Gilbert, P. A proof-of-concept pilot randomized comparative trial of brief Internet-based compassionate mind training and cognitive-behavioral therapy for perinatal and intending to become pregnant women. Clin. Psychol. Psychother. 2018, 25, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Krusche, A.; Dymond, M.; Murphy, S.E.; Crane, C. Mindfulness for pregnancy: A randomized controlled study of online mindfulness during pregnancy. Midwifery 2018, 65, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Matvienko-Sikar, K.; Dockray, S. Effects of a novel positive psychological intervention on prenatal stress and well-being: A pilot randomized controlled trial. Women Birth J. Aust. Coll. Midwives 2017, 30, e111–e118. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.B.; Mahnert, N.D.; Foote, J.; Saunders, K.T.; Mourad, J.; Huberty, J. Mindfulness Effects in Obstetric and Gynecology Patients During the Coronavirus Disease 2019 (COVID-19) Pandemic: A Randomized Controlled Trial. Obstet. Gynecol. 2021, 137, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Li, Y.; Wang, J.; Chen, Q.; Bazzano, A.N.; Cao, F. Effectiveness of Smartphone-Based Mindfulness Training on Maternal Perinatal Depression: Randomized Controlled Trial. J. Med. Internet Res. 2021, 23, e23410. [Google Scholar] [CrossRef]
- Yang, M.; Jia, G.; Sun, S.; Ye, C.; Zhang, R.; Yu, X. Effects of an Online Mindfulness Intervention Focusing on Attention Monitoring and Acceptance in Pregnant Women: A Randomized Controlled Trial. J. Midwifery Women’s Health 2019, 64, 68–77. [Google Scholar] [CrossRef]
- Yang, M.; Zhou, X.; Ye, C.; Li, J.; Sun, S.; Yu, X. Emphasizing mindfulness training in acceptance relieves anxiety and depression during pregnancy. Psychiatry Res. 2022, 312, 114540. [Google Scholar] [CrossRef]
- Zhang, X.; Lin, P.; Sun, J.; Sun, Y.; Di Shao Cao, D.; Cao, F. Prenatal stress self-help mindfulness intervention via social media: A randomized controlled trial. J. Ment. Health 2021, 32, 206–215. [Google Scholar] [CrossRef]
- Zhang, X.; Mao, F.; Li, Y.; Wang, J.; Wu, L.; Sun, J.; Cao, F. Effects of a maternal mindfulness intervention targeting prenatal psychological distress on infants’ meconium microbiota: A randomized controlled trial. Psychoneuroendocrinology 2022, 145, 105913. [Google Scholar] [CrossRef]
- Hilt, L.M.; Pollak, S.D. Getting out of rumination: Comparison of three brief interventions in a sample of youth. J. Abnorm. Child Psychol. 2012, 40, 1157–1165. [Google Scholar] [CrossRef]
- Perestelo-Perez, L.; Barraca, J.; Peñate, W.; Rivero-Santana, A.; Alvarez-Perez, Y. Mindfulness-based interventions for the treatment of depressive rumination: Systematic review and meta-analysis. Int. J. Clin. Health Psychol. IJCHP 2017, 17, 282–295. [Google Scholar] [CrossRef] [PubMed]
- Garland, E.L.; Geschwind, N.; Peeters, F.; Wichers, M. Mindfulness training promotes upward spirals of positive affect and cognition: Multilevel and autoregressive latent trajectory modeling analyses. Front. Psychol. 2015, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Noma, H.; Karyotaki, E.; Cipriani, A.; Furukawa, T.A. Effectiveness and Acceptability of Cognitive Behavior Therapy Delivery Formats in Adults with Depression: A Network Meta-analysis. JAMA Psychiatry 2019, 76, 700–707. [Google Scholar] [CrossRef]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; van Gemert-Pijnen, J.E.W.C. Persuasive system design does matter: A systematic review of adherence to web-based interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef]
- Duong, H.T.; Hoyt, A.T.; Carmichael, S.L.; Gilboa, S.M.; Canfield, M.A.; Case, A.; McNeese, M.L.; Waller, D.K. Is maternal parity an independent risk factor for birth defects? Birth Defects Res. Part A Clin. Mol. Teratol. 2012, 94, 230–236. [Google Scholar] [CrossRef]
- Jaspinder Kaur, K.K. Obstetric complications: Primiparity Vs. Multiparity. Eur. J. Exp. Biol. 2012, 2, 1462–1468. [Google Scholar]
- Gameiro, S.; Moura-Ramos, M.; Canavarro, M.C. Maternal adjustment to the birth of a child: Primiparity versus multiparity. J. Reprod. Infant Psychol. 2009, 27, 269–286. [Google Scholar] [CrossRef]
- Fenwick, J.; Toohill, J.; Creedy, D.K.; Smith, J.; Gamble, J. Sources, responses and moderators of childbirth fear in Australian women: A qualitative investigation. Midwifery 2015, 31, 239–246. [Google Scholar] [CrossRef]
- O’Connell, M.A.; Leahy-Warren, P.; Kenny, L.C.; O’Neill, S.M.; Khashan, A.S. The prevalence and risk factors of fear of childbirth among pregnant women: A cross-sectional study in Ireland. Acta Obstet. Et Gynecol. Scand. 2019, 98, 1014–1023. [Google Scholar] [CrossRef]
- Shakarami, A.; Mirghafourvand, M.; Abdolalipour, S.; Jafarabadi, M.A.; Iravani, M. Comparison of fear, anxiety and self-efficacy of childbirth among primiparous and multiparous women. BMC Pregnancy Childbirth 2021, 21, 642. [Google Scholar] [CrossRef]
- Andrews, G.; Basu, A.; Cuijpers, P.; Craske, M.G.; McEvoy, P.; English, C.L.; Newby, J.M. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: An updated meta-analysis. J. Anxiety Disord. 2018, 55, 70–78. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year of Publication | N | Country of Conduct | nIG | nCG | Outcome (Measure) | M ± SD | M ± SD | Intervention Group | Control Group | Duration of Intervention (in Weeks) | Number of Sessions | Attrition Rate (IG), % |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Carissoli et al., 2017 [50] b,d,g | 78 | Italy | 35 | 43 | Anxiety (W-DEQ) | 26.76 ± 5.95 | 27.09 ± 6.74 | App BenEssere Mamma (daily relaxation, guided imagery exercises, mood journal) | Treatment as usual | 4.00 | 20 | NA |
| Matvienko-Sikar and Dockray, 2017 [56] c,d,g | 36 | Ireland | 24 | 12 | Depression (EPDS) | 26.71 ± 7.47 | 22.17 ± 5.98 | Gratitude diary and mindfulness listening | Treatment as usual | 3.00 | 12 | 25.00 |
| Stress (PDQ) | 15.50 ± 3.91 | 15.08 ± 3.72 | ||||||||||
| Kelman et al., 2018 [54] a,c,d,h | 40 | USA | 22 | 18 | Depression (PHQ-2) | NA l | NA l | Internet-based compassionate mind training (CMT) | Internet-based cognitive–behavioral therapy (CBT) | 2.00 | 4 | 40.58 |
| Anxiety (GAD-2) | NA l | NA l | ||||||||||
| Krusche et al., 2018 [55] c,e,h | 72 | UK | 22 | 50 | Depression (EPDS) | NA m | NA m | www.bemindfulonline.com (guided meditation and mindfulness-based exercises) | Wait-list | 4.00 | 10 | 79.44 |
| Anxiety (GAD-7) | NA m | NA m | ||||||||||
| Anxiety (OWLS) | NA m | NA m | ||||||||||
| Stress (PSS) | NA m | NA m | ||||||||||
| Stress (TPDS) | NA m | NA m | ||||||||||
| Yang et al., 2019 [59] b,e,f | 123 | China | 62 | 61 | Depression (PHQ-9) | 3.58 ± 2.32 | 6.26 ± 3.31 | Mindfulness, attention monitoring and acceptance | Treatment as usual | 8.00 | 4 | 16.13 |
| Anxiety (GAD-7) | 2.97 ± 2.34 | 5.26 ± 2.88 | ||||||||||
| Guo et al., 2020 [53] c,e,h,i | 284 | China | 144 | 140 | Depression (EPDS) | 7.56 ± 1.77 | 10.38 ± 1.77 | Mindful Self-Compassion | Wait-list | 6.00 | 36 | 8.28 |
| Doty et al., 2021 [51] a,c,d,g | 41 | USA | 20 | 21 | Depression (EPDS) | 7.00 ± 4.90 j | 9.90 ± 5.30 | App Calm (mindfulness meditation program) | Treatment as usual | 0.57 | 6 | 28.57 |
| Anxiety (STAI) | 37.50 ± 13.10 | 42.00 ± 10.80 | ||||||||||
| Stress (PSS) | 16.60 ± 6.80 | 19.10 ± 7.60 | ||||||||||
| Smith et al., 2021 [57] a,b,d,g | 101 | USA | 50 | 51 | Depression (HADS) | 4.00 ± 2.90 | 5.40 ± 3.40 | App Calm (mindfulness meditation program) | Treatment as usual | 4.30 | 30 | 14.00 |
| Anxiety (HADS) | 5.00 ± 3.90 | 6.90 ± 4.70 | ||||||||||
| Stress (PSS) | 12.70 ± 5.60 | 17.00 ± 6.70 | ||||||||||
| Sun et al., 2021 [58] a,b,e,g | 168 | China | 84 | 84 | Depression (EPDS) | 6.49 ± 4.50 | 9.09 ± 6.24 | Smartphone-based mindfulness training | Text-based health consultations | 8.00 | 8 | 25.00 |
| Anxiety (GAD-7) | 4.46 ± 2.95 | 5.56 ± 4.97 | ||||||||||
| Stress (PSS) | 5.22 ± 2.73 | 6.09 ± 3.63 | ||||||||||
| Zhang et al., 2021 [61] a,b,e,f | 108 | China | 54 | 54 | Depression (EPDS) | 7.17 ± 3.81 | 9.54 ± 3.90 | Mindfulness-based intervention (MBI) | Health education | 4.00 | 4 | 33.33 |
| Anxiety (GAD-7) | 4.56 ± 2.74 | 5.98 ± 3.74 | ||||||||||
| Stress (PSS-4) | 4.38 ± 2.45 | 6.59 ± 5.53 | ||||||||||
| Güney et al., 2022 [52] c,d,i | 84 | Turkey | 42 | 42 | Anxiety (BAI) | 6.50 ± 5.98 | 14.47 ± 5.58 | Mindfulness-Based Stress Reduction (MBSR) program | Wait-list | 4.00 | 8 | 12.50 |
| Anxiety (CAQ) | 26.38 ± 5.04 | 36.11 ± 5.67 | ||||||||||
| Stress (NuPDQ) | 7.47 ± 3.89 | 13.97 ± 3.33 | ||||||||||
| Yang et al., 2022 [60] c,e,f | 108 | China | 74 | 34 | Depression (PHQ-9) | 4.99 ± 3.09 | 6.52 ± 3.36 | Monitoring (MT) or monitoring with an emphasis on acceptance training (MAT) | Emotional regulation course | 4.00 | 4 | 27.52 |
| Anxiety (GAD-7) | 8.08 ± 3.22 | 6.50 ± 2.91 | ||||||||||
| Zhang et al., 2022 [62] a,c,e,f,k | 130 | China | 66 | 64 | Depression (EPDS) | 4.97 ± 4.35 | 7.69 ± 5.08 | Guided self-help mindfulness-based intervention (MBI) | Treatment as usual | 6.00 | 6 | 17.50 |
| Anxiety (GAD-7) | 2.98 ± 2.70 | 5.61 ± 3.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mefrouche, M.L.; Siegmann, E.-M.; Böhme, S.; Berking, M.; Kornhuber, J. The Effect of Digital Mindfulness Interventions on Depressive, Anxiety, and Stress Symptoms in Pregnant Women: A Systematic Review and Meta-Analysis. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1694-1706. https://doi.org/10.3390/ejihpe13090122
Mefrouche ML, Siegmann E-M, Böhme S, Berking M, Kornhuber J. The Effect of Digital Mindfulness Interventions on Depressive, Anxiety, and Stress Symptoms in Pregnant Women: A Systematic Review and Meta-Analysis. European Journal of Investigation in Health, Psychology and Education. 2023; 13(9):1694-1706. https://doi.org/10.3390/ejihpe13090122
Chicago/Turabian StyleMefrouche, Monique L., Eva-Maria Siegmann, Stephanie Böhme, Matthias Berking, and Johannes Kornhuber. 2023. "The Effect of Digital Mindfulness Interventions on Depressive, Anxiety, and Stress Symptoms in Pregnant Women: A Systematic Review and Meta-Analysis" European Journal of Investigation in Health, Psychology and Education 13, no. 9: 1694-1706. https://doi.org/10.3390/ejihpe13090122
APA StyleMefrouche, M. L., Siegmann, E.-M., Böhme, S., Berking, M., & Kornhuber, J. (2023). The Effect of Digital Mindfulness Interventions on Depressive, Anxiety, and Stress Symptoms in Pregnant Women: A Systematic Review and Meta-Analysis. European Journal of Investigation in Health, Psychology and Education, 13(9), 1694-1706. https://doi.org/10.3390/ejihpe13090122