


Influence of Prefabricated Construction on the Mental Health of Workers: Systematic Review




Abstract
1. Introduction
- Identify and classify mental health stressors in accordance with their sources.
- Assess the relevance of prefabricated construction techniques in improving the mental health of construction workers.
2. Materials and Methods
2.1. Phase 1—Mental Health Stressors in Construction
2.1.1. Literature Search Strategies and Terms
2.1.2. Exclusion and Inclusion Criteria
- Articles that studied either the causes of or intervention for mental health among construction workers;
- Articles that studied common mental health disorders (such as anxiety, depression, behavioural disorders, and posttraumatic stress disorder) among construction workers of all ages, gender, occupations, professions, and cadres;
- Conducted the study and made decisions based on empirical data collected. Where pilot studies were considered, such studies must have conducted full-scale data collection and included in the whole analysis and findings;
- Studies based on scoping review, systematic review, and any other forms of reviews of the literature were excluded;
- Articles must have been published in English. Articles published in other languages other than English but with official English versions available were included;
- Articles published in peer-reviewed journals were included. Other articles, such as conference papers, book chapters, reviews, white papers, etc., were excluded even in cases where they met other inclusion requirements. Apart from the fact that journal publications undergo a stringent peer-review process, it is widely confirmed among researchers that they are the most reliable and comprehensive source of knowledge in a research area.
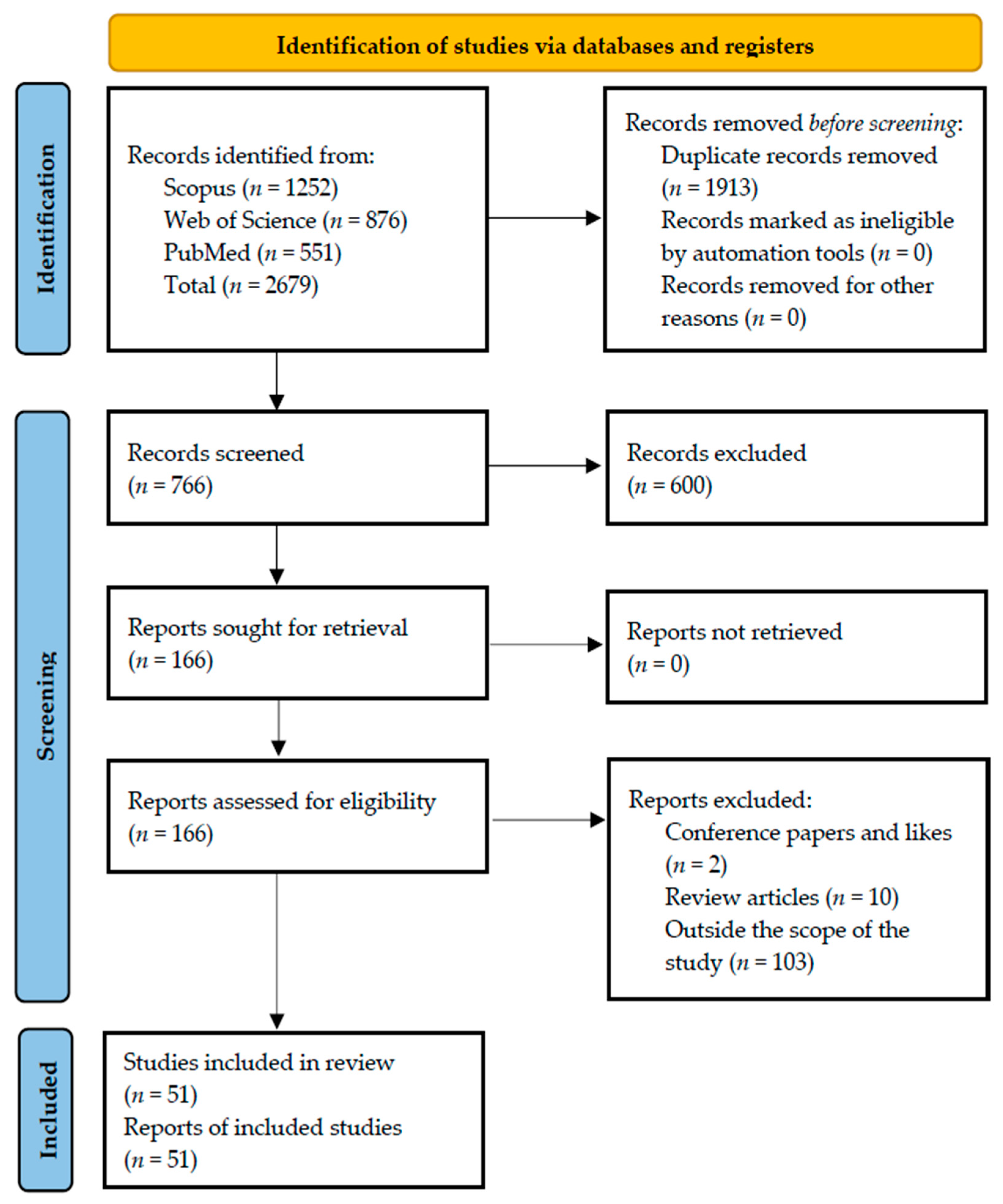
2.1.3. Data Extraction and Final Article Selection
2.2. Phase 2—Prefabricated Construction and Health and Safety
2.2.1. Literature Search Strategies and Terms
2.2.2. Exclusion and Inclusion Criteria
- Articles that studied the health and safety problems in the context of prefabricated construction;
- Articles that based their studies on empirical qualitative and quantitative data and not data collected with pilot studies. Where pilot studies were considered, such studies must have conducted full-scale data collection and been included in the whole analysis and findings;
- Studies based on scoping review, systematic review, and any other forms of reviews of the literature were excluded;
- Articles must have been published in English. Articles published in other languages other than English but with official English versions available were included;
- Articles published in peer-reviewed journals were included. Other articles, such as conference papers, book chapters, reviews, white papers, etc., were excluded even in cases where they met other inclusion requirements.
2.2.3. Data Extraction and Final Article Selection
3. Results
3.1. Overview of the Articles Selected on Mental Health Stressors
3.2. Mental Health Stressors of Construction Workers
3.2.1. Industry-related Stressors
3.2.2. Management/Organisational Stressors
3.2.3. Personal Stressors
3.2.4. Preventive Measures of Poor Mental Health among Construction Workers
3.3. Prefabricated Construction
Health and Safety Performance of Prefabricated Construction
4. Discussion: Prefabricated Construction as a Tool for Good Mental Health
5. Limitations
6. Conclusions
7. Recommendation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lingard, H.; Turner, M. Improving the Health of Male, Blue Collar Construction Workers: A Social Ecological Perspective. Constr. Manag. Econ. 2015, 33, 18–34. [Google Scholar] [CrossRef]
- Lim, S.; Chi, S.; Lee, J.D.; Lee, H.J.; Choi, H. Analyzing Psychological Conditions of Field-Workers in the Construction Industry. Int. J. Occup. Environ. Health 2017, 23, 261–281. [Google Scholar] [CrossRef]
- Turner, M.; Lingard, H. Examining the Interaction between Bodily Pain and Mental Health of Construction Workers. Constr. Manag. Econ. 2020, 38, 1009–1023. [Google Scholar] [CrossRef]
- Milner, A.; Maheen, H.; Currier, D.; LaMontagne, A.D. Male Suicide among Construction Workers in Australia: A Qualitative Analysis of the Major Stressors Precipitating Death. BMC Public Health 2017, 17, 584. [Google Scholar] [CrossRef] [PubMed]
- King, T.L.; Batterham, P.J.; Lingard, H.; Gullestrup, J.; Lockwood, C.; Harvey, S.B.; Kelly, B.; Lamontagne, A.D.; Milner, A. Are Young Men Getting the Message? Age Differences in Suicide Prevention Literacy among Male Construction Workers. Int. J. Environ. Res. Public Health 2019, 16, 475. [Google Scholar] [CrossRef] [PubMed]
- Heller, T.S.; Hawgood, J.L.; de Leo, D. Correlates of Suicide in Building Industry Workers. Arch. Suicide Res. 2007, 11, 105–117. [Google Scholar] [CrossRef]
- Gullestrup, J.; Lequertier, B.; Martin, G. MATES in Construction: Impact of a Multimodal, Community-Based Program for Suicide Prevention in the Construction Industry. Int. J. Environ. Res. Public Health 2011, 8, 4180–4196. [Google Scholar] [CrossRef]
- Love, P.E.D.; Edwards, D.J.; Irani, Z. Work Stress, Support, and Mental Health in Construction. J. Constr. Eng. Manag. 2010, 136, 650–658. [Google Scholar] [CrossRef]
- Egege, C.O. Off-Site Modular Construction as a Method of Improving Construction Quality and Safety. Int. J. Struct. Civ. Eng. Res. 2018, 259–268. [Google Scholar] [CrossRef]
- Melia, J.P.; Becerril, M. Psychosocial Sources of Stress and Burnout in the Construction Sector A Structural Equation Model. Psicothema 2007, 19, 679–686. [Google Scholar]
- Hashemi, A. Offsite Manufacturing: A Survey on the Current Status and Risks of Offsite Construction in Iran. J. Civ. Eng. Archit. 2015, 9, 141–152. [Google Scholar] [CrossRef]
- Boschman, J.S.; van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H.W. Psychosocial Work Environment and Mental Health among Construction Workers. Appl. Ergon. 2013, 44, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Pirzadeh, P.; Lingard, H.; Zhang, R.P. Job Quality and Construction Workers’ Mental Health: Life Course Perspective. J. Constr. Eng. Manag. 2022, 148, 04022132. [Google Scholar] [CrossRef]
- Ahn, S.; Crouch, L.; Kim, T.W.; Rameezdeen, R. Comparison of Worker Safety Risks between Onsite and Offsite Construction Methods: A Site Management Perspective. J. Constr. Eng. Manag. 2020, 146, 05020010. [Google Scholar] [CrossRef]
- Chen, Y.; Okudan, G.E.; Riley, D.R. Sustainable Performance Criteria for Construction Method Selection in Concrete Buildings. Autom. Constr. 2010, 19, 235–244. [Google Scholar] [CrossRef]
- Blismas, N.; Pasquire, C.; Gibb, A. Benefit Evaluation for Off-Site Production in Construction. Constr. Manag. Econ. 2006, 24, 121–130. [Google Scholar] [CrossRef]
- Burdorf, A.; Govaert, G.; Elders, L. Postural Load and Back Pain of Workers in the Manufacturing of Prefabricated Concrete Elements. Ergonomics 1991, 34, 909–918. [Google Scholar] [CrossRef]
- Rwamamara, R.A. Risk Assessment and Analysis of Workload in an Industrialised Construction Process. Constr. Inf. Q. 2007, 9, 80–85. [Google Scholar]
- Kim, S.; Seol, H.; Ikuma, L.H.; Nussbaum, M.A. Knowledge and Opinions of Designers of Industrialized Wall Panels Regarding Incorporating Ergonomics in Design. Int. J. Ind. Ergon. 2008, 38, 150–157. [Google Scholar] [CrossRef]
- Rwamamara, R.A.; Lagerqvist, O.; Olofsson, T.; Johansson, B.M.; Kaminskas, K.A. Evidence-Based Prevention of Work-Related Musculoskeletal Injuries in Construction Industry. J. Civ. Eng. Manag. 2010, 16, 499–509. [Google Scholar] [CrossRef]
- Pidd, K.; Duraisingam, V.; Roche, A.; Trifonoff, A. Young Construction Workers: Substance Use, Mental Health, and Workplace Psychosocial Factors. Adv. Dual Diagn. 2017, 10, 155–168. [Google Scholar] [CrossRef]
- Gibb, A.G.F.; Isack, F. Client Drivers for Construction Projects: Implications for Standardisation. Eng. Constr. Archit. Manag. 2001, 8, 46–58. [Google Scholar] [CrossRef]
- Alryalat, S.A.S.; Malkawi, L.W.; Momani, S.M. Comparing Bibliometric Analysis Using Pubmed, Scopus, and Web of Science Databases. J. Vis. Exp. 2019, 152, e58494. [Google Scholar] [CrossRef]
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: Strengths and Weaknesses. FASEB J. 2008, 22, 338–342. [Google Scholar] [CrossRef]
- Harris, J.D.; Quatman, C.E.; Manring, M.M.; Siston, R.A.; Flanigan, D.C. How to Write a Systematic Review. Am. J. Sports Med. 2014, 42, 2761–2768. [Google Scholar] [CrossRef]
- Frimpong, S.; Sunindijo, R.Y.; Wang, C.C. Mental Health Conditions among Young Construction Workers: A Systematic Narrative Review. Environ. Sci. Proc. 2022, 12, 21. [Google Scholar] [CrossRef]
- Frimpong, S.; Sunindijo, R.Y.; Wang, C.C.; Boadu, E.F. Domains of Psychosocial Risk Factors Affecting Young Construction Workers: A Systematic Review. Buildings 2022, 12, 335. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.; Osei-kyei, R. A Systematic Review of Mental Stressors in the Construction Industry. Int. J. Build. Pathol. Adapt. 2020, 39, 433–460. [Google Scholar] [CrossRef]
- Liu, Q.; Feng, Y.; London, K. Theorizing to Improve Mental Health in Multicultural Construction Industries: An Intercultural Coping Model. Buildings 2021, 11, 662. [Google Scholar] [CrossRef]
- Chan, A.P.C.; Nwaogu, J.M.; Naslund, J.A. Mental Ill-Health Risk Factors in the Construction Industry. J. Constr. Eng. Manag. 2020, 146, 04020004. [Google Scholar] [CrossRef]
- Sutherland, V.; Davidson, M.J. Using a Stress Audit: The Construction Site Manager Experience in the UK. Work. Stress 1993, 7, 273–286. [Google Scholar] [CrossRef]
- Sunindijo, R.Y.; Kamardeen, I. Work Stress Is a Threat to Gender Diversity in the Construction Industry. J. Constr. Eng. Manag. 2017, 143, 71–80. [Google Scholar] [CrossRef]
- Ahmed, K.; Leung, M.; Ojo, L.D. An Exploratory Study to Identify Key Stressors of Ethnic Minority Workers in the Construction Industry. J. Constr. Eng. Manag. 2022, 148, 04022014. [Google Scholar] [CrossRef]
- Flannery, J.; Ajayi, S.O.; Oyegoke, A.S. Alcohol and Substance Misuse in the Construction Industry. Int. J. Occup. Saf. Ergon. 2021, 27, 472–487. [Google Scholar] [CrossRef]
- Sushanthi, S.; Doraikannan, S.; Indiran, M.A. Assessment of Anxiety, Depression and Nicotine Dependence among Construction Workers in Chennai—A Cross Sectional Study. J. Oral. Biol. Craniofac. Res. 2022, 12, 263–267. [Google Scholar] [CrossRef]
- Curtis, H.M.; Meischke, H.; Stover, B.; Simcox, N.J.; Seixas, N.S. Gendered Safety and Health Risks in the Construction Trades. Ann. Work. Expo. Health 2018, 62, 404–415. [Google Scholar] [CrossRef]
- Kotera, Y.; Green, P.; Sheffield, D. Work-Life Balance of UK Construction Workers: Relationship with Mental Health. Constr. Manag. Econ. 2020, 38, 291–303. [Google Scholar] [CrossRef]
- Bowen, P.; Zhang, R.P. Cross-Boundary Contact, Work-Family Conflict, Antecedents, and Consequences: Testing an Integrated Model for Construction Professionals. J. Constr. Eng. Manag. 2020, 146, 04020005. [Google Scholar] [CrossRef]
- Langdon, R.R.; Sawang, S. Construction Workers’ Well-Being: What Leads to Depression, Anxiety, and Stress? J. Constr. Eng. Manag. 2018, 144, 040171002–0401710015. [Google Scholar] [CrossRef]
- Eyllon, M.; Vallas, S.P.; Dennerlein, J.T.; Garverich, S.; Weinstein, D.; Owens, K.; Lincoln, A.K. Mental Health Stigma and Wellbeing Among Commercial Construction Workers: A Mixed Methods Study. J. Occup. Environ. Med. 2020, 62, e423–e430. [Google Scholar] [CrossRef]
- Hulls, P.M.; de Vocht, F.; Martin, R.M.; Langford, R.M. We Are Our Own Worst Enemy: A Qualitative Exploration of Work-Related Stress in the Construction Industry. Int. J. Workplace Health Manag. 2022, 15, 609–622. [Google Scholar] [CrossRef]
- Jacobsen, H.B.; Caban-Martinez, A.; Onyebeke, L.C.; Sorensen, G.; Dennerlein, J.T.; Reme, S.E. Construction Workers Struggle with a High Prevalence of Mental Distress, and This Is Associated with Their Pain and Injuries. J. Occup. Environ. Med. 2013, 55, 1197–1204. [Google Scholar] [CrossRef]
- Dong, S.; He, Q.; Li, H.; Yin, Q. Automated PPE Misuse Identification and Assessment for Safety Performance Enhancement. In ICCREM; ASCE: Reston, VA, USA, 2015; pp. 204–214. [Google Scholar]
- Dong, X.S.; Brooks, R.D.; Brown, S.; Harris, W. Psychological Distress and Suicidal Ideation among Male Construction Workers in the United States. Am. J. Ind. Med. 2022, 65, 396–408. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.S.; Liang, Y.X.; Hu, X.Y.; Long, Y.F.; Ge, L.N. Posttraumatic Stress Disorder in Co-Workers Following Exposure to a Fatal Construction Accident in China. Int. J. Occup. Environ. Health 2000, 6, 203–207. [Google Scholar] [CrossRef]
- Nwaogu, J.M.; Chan, A.P.C.; Akinyemi, T.A. Conceptualizing the Dynamics of Mental Health among Construction Supervisors. Int. J. Constr. Manag. 2022, 1–21. [Google Scholar] [CrossRef]
- Nwaogu, J.M.; Chan, A.P.C.; Naslund, J.A. Measures to Improve the Mental Health of Construction Personnel Based on Expert Opinions. J. Manag. Eng. 2022, 38, 04022019. [Google Scholar] [CrossRef]
- Bowen, P.; Govender, R.; Edwards, P. Structural Equation Modeling of Occupational Stress in the Construction Industry. J. Constr. Eng. Manag. 2014, 140, 04020013. [Google Scholar] [CrossRef]
- Dennerlein, J.T.; Eyllon, M.; Garverich, S.; Weinstein, D.; Manjourides, J.; Vallas, S.P.; Lincoln, A.K. Associations between Work-Related Factors and Psychological Distress among Construction Workers. J. Occup. Environ. Med. 2021, 63, 1052–1057. [Google Scholar] [CrossRef]
- Bowen, P.; Peihua Zhang, R.; Edwards, P. An Investigation of Work-Related Strain Effects and Coping Mechanisms among South African Construction Professionals. Constr. Manag. Econ. 2021, 39, 298–322. [Google Scholar] [CrossRef]
- Bowers, J.; Lo, J.; Miller, P.; Mawren, D.; Jones, B. Psychological Distress in Remote Mining and Construction Workers in Australia. Med. J. Aust. 2018, 208, 391–397. [Google Scholar] [CrossRef]
- Zaniboni, S.; Truxillo, D.M.; Rineer, J.R.; Bodner, T.E.; Hammer, L.B.; Krainer, M. Relating Age, Decision Authority, Job Satisfaction, and Mental Health: A Study of Construction Workers. Work. Aging Retire 2016, 2, 428–435. [Google Scholar] [CrossRef]
- Kamardeen, I.; Sunindijo, R.Y. Personal Characteristics Moderate Work Stress in Construction Professionals. J. Constr. Eng. Manag. 2017, 143, 040170721–040170728. [Google Scholar] [CrossRef]
- Chapman, J.; Roche, A.M.; Duraisingam, V.; Ledner, B.; Finnane, J.; Pidd, K. Exploring the Relationship between Psychological Distress and Likelihood of Help Seeking in Construction Workers: The Role of Talking to Workmates and Knowing How to Get Help. Work 2020, 67, 47–54. [Google Scholar] [CrossRef]
- Bowen, P.; Edwards, P.; Lingard, H.; Cattell, K. Workplace Stress, Stress Effects, and Coping Mechanisms in the Construction Industry. J. Constr. Eng. Manag. 2014, 140, 04013059. [Google Scholar] [CrossRef]
- Ross, V.; Mathieu, S.L.; Wardhani, R.; Gullestrup, J.; Kõlves, K. Factors Associated With Workplace Bullying and the Mental Health of Construction Industry Apprentices: A Mixed Methods Study. Front. Psychiatry 2021, 12, 629262. [Google Scholar] [CrossRef] [PubMed]
- Saroglou, V.; Cohen, A.B. Psychology of Culture and Religion. J. Cross Cult. Psychol. 2011, 42, 1309–1319. [Google Scholar] [CrossRef]
- Palaniappan, K.; Natarajan, R.; Dasgupta, C. Prevalence and Risk Factors for Depression, Anxiety and Stress among Foreign Construction Workers in Singapore—A Cross-Sectional Study. Int. J. Constr. Manag. 2022, 1–9. [Google Scholar] [CrossRef]
- Liu, Q.; Feng, Y.; London, K.; Zhang, P. Influence of Personal Characteristics and Environmental Stressors on Mental Health for Multicultural Construction Workplaces in Australia. Constr. Manag. Econ. 2022, 41, 116–137. [Google Scholar] [CrossRef]
- King, T.L.; Gullestrup, J.; Batterham, P.J.; Kelly, B.; Lockwood, C.; Lingard, H.; Harvey, S.B.; Lamontagne, A.D.; Milner, A. Shifting Beliefs about Suicide: Pre-Post Evaluation of the Effectiveness of a Program for Workers in the Construction Industry. Int. J. Environ. Res. Public Health 2018, 15, 2106. [Google Scholar] [CrossRef]
- Ross, V.; Caton, N.; Gullestrup, J.; Kõlves, K. A Longitudinal Assessment of Two Suicide Prevention Training Programs for the Construction Industry. Int. J. Environ. Res. Public Health 2020, 17, 803. [Google Scholar] [CrossRef]
- Doran, C.M.; Wittenhagen, L.; Heffernan, E.; Meurk, C. The Mates Case Management Model: Presenting Problems and Referral Pathways for a Novel Peer-Led Approach to Addressing Suicide in the Construction Industry. Int. J. Environ. Res. Public Health 2021, 18, 6740. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, R.; Papadopoulos, T. Improving Mental Health and Wellbeing for Young Men in the Building and Construction Industry. J. Child Adolesc. Ment. Health 2014, 26, 217–227. [Google Scholar] [CrossRef]
- Ajayi, S.O.; Jones, W.; Unuigbe, M. Occupational Stress Management for UK Construction Professionals: Understanding the Causes and Strategies for Improvement. J. Eng. Des. Technol. 2019, 17, 819–832. [Google Scholar] [CrossRef]
- Nwaogu, J.M.; Chan, A.P.C. Evaluation of Multi-Level Intervention Strategies for a Psychologically Healthy Construction Workplace in Nigeria. J. Eng. Des. Technol. 2021, 19, 509–536. [Google Scholar] [CrossRef]
- Milner, A.; Aitken, Z.; Law, P.C.F.; Lamontagne, A.D.; Mann, C.; Cooper, T.; Witt, K. The Relationship between an Electronic Mental Health Stigma Campaign and Suicidal Thoughts and Behaviours: A Two-Arm Randomized Controlled Trial in the Australian Construction Industry. Health Promot. Int. 2019, 35, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Ye, G.; Feng, Y. Workers’ Safety Behaviors in the off-Site Manufacturing Plant. Eng. Constr. Archit. Manag. 2020, 27, 765–784. [Google Scholar] [CrossRef]
- Nussbaum, M.A.; Shewchuk, J.P.; Kim, S.; Seol, H.; Guo, C. Development of a Decision Support System for Residential Construction Using Panellised Walls: Approach and Preliminary Results. Ergonomics 2009, 52, 87–103. [Google Scholar] [CrossRef]
- Kim, S.; Nussbaum, M.A.; Jia, B. The Benefits of an Additional Worker Are Task-Dependent: Assessing Low-Back Injury Risks during Prefabricated (Panelized) Wall Construction. Appl. Ergon. 2012, 43, 843–849. [Google Scholar] [CrossRef]
- Court, P.F.; Pasquire, C.L.; Gibb, A.G.F.; Bower, D. Modular Assembly with Postponement to Improve Health, Safety and Productivity in Construction. Pract. Period. Struct. Des. Constr. 2009, 14, 81–89. [Google Scholar] [CrossRef]
- Peñaloza, G.A.; Formoso, C.T.; Saurin, T.A. Resilience Skills Used by Front-Line Workers to Assemble Precast Concrete Structures: An Exploratory Study. Ambiente Construído 2017, 17, 25–43. [Google Scholar] [CrossRef]
- Fard, M.M.; Terouhid, S.A.; Kibert, C.J.; Hakim, H. Safety Concerns Related to Modular/Prefabricated Building Construction. Int. J. Inj. Contr. Saf. Promot. 2017, 24, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lu, M.; Chan, G.; Skitmore, M. Proactive Training System for Safe and Efficient Precast Installation. Autom. Constr. 2015, 49, 163–174. [Google Scholar] [CrossRef]
- Rubio-Romero, J.C.; Suárez-Cebador, M.; Abad, J. Modeling Injury Rates as a Function of Industrialized versus On-Site Construction Techniques. Accid. Anal. Prev. 2014, 66, 8–14. [Google Scholar] [CrossRef]
- Pan, W.; Gibb, A.G.F.; Dainty, A.R.J. Leading UK Housebuilders’ Utilization of Offsite Construction Methods. Build. Res. Inf. 2008, 36, 56–67. [Google Scholar] [CrossRef]
- James, J.; Ikuma, L.H.; Nahmens, I.; Aghazadeh, F. The Impact of Kaizen on Safety in Modular Home Manufacturing. Int. J. Adv. Manuf. Technol. 2014, 70, 725–734. [Google Scholar] [CrossRef]
- Jaillon, L.; Poon, C.S. Sustainable Construction Aspects of Using Prefabrication in Dense Urban Environment: A Hong Kong Case Study. Constr. Manag. Econ. 2008, 26, 953–966. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SN | Mental Health Stressors | Reference(s) |
|---|---|---|
| A | Industry-related Stressors | |
| 1 | Work pressure | [6,31,32,33] |
| 2 | Long working hours | [1,6,32,33,34,35] |
| 3 | Psycho–social isolation | [36] |
| 4 | Business culture | [6,13,31,33,34,39,40,41] |
| 5 | Bodily or musculoskeletal pain | [3,42] |
| 6 | Physical injuries from site accidents | [4,42,43,44,45] |
| 7 | Fatigue | [50] |
| 8 | Unhealthy increase in work speed | [12,13] |
| 9 | Work-related physical illness | [4,44] |
| 10 | Job insecurity | [31,33,34,39,41] |
| 11 | Poor working condition | [33] |
| 12 | Nature of work | [34,39] |
| 13 | The stigma attached to mental health | [40] |
| 14 | Job mental (cognitive) demand | [12,13,46,47,48,49] |
| B | Management/Organisational Stressors | |
| 1 | Interpersonal conflicts | [34,48,50] |
| 2 | Inadequate job resources | [33] |
| 3 | Unclear directions from supervisors and management | [10,31,33] |
| 4 | Poor communication | [33,58] |
| 5 | Unfavourable shift rosters | [51] |
| 6 | Technology overload, e.g., BIM, drones, etc. | [31] |
| 7 | Work overload | [31,32] |
| 8 | Undue and excessive criticism | [32] |
| 9 | Lack of task autonomy | [52] |
| 10 | Lack of participation in decision-making | [12] |
| 11 | Poor workers’ support mechanism | [49] |
| 12 | Poor feedback mechanism | [33] |
| C | Personal Stressors | |
| 1 | Age discrimination | [48] |
| 2 | Gender discrimination | [32] |
| 3 | Workplace harassment | [32,36] |
| 4 | Marital status | [51,53] |
| 5 | Financial difficulties | [4,34] |
| 6 | Low socio–economic status | [41] |
| 7 | Opportunities for further learning | [12] |
| 8 | Poor work–life balance | [1,6,36,37] |
| 9 | Language barriers | [33] |
| 10 | Racial discrimination | [33,58] |
| 11 | Cultural/Religious values conflicts | [33,58,59] |
| SN | Benefits of Prefabrication | Reference(s) |
|---|---|---|
| 1 | Construction process standardisation | [9] |
| 2 | Safety risks become easier to identify and control | [75] |
| 3 | Reduction in trade overlap and site congestion | [70] |
| 4 | Reduction in people working in dangerous positions | [14] |
| 5 | Reduction in the frequency of dangerous works on site | [14] |
| 6 | Cleaner construction and less exposure to harm | [20] |
| 7 | Ample space for safe preassembly of components | [20] |
| 8 | Reduction in physically demanding on-site tasks | [18] |
| 9 | Less time spent on site and exposure to weather | [14] |
| 10 | Reduced chances of occurrence of falls, struck-by, etc. | [18,76] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fagbenro, R.K.; Sunindijo, R.Y.; Illankoon, C.; Frimpong, S. Influence of Prefabricated Construction on the Mental Health of Workers: Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 345-363. https://doi.org/10.3390/ejihpe13020026
Fagbenro RK, Sunindijo RY, Illankoon C, Frimpong S. Influence of Prefabricated Construction on the Mental Health of Workers: Systematic Review. European Journal of Investigation in Health, Psychology and Education. 2023; 13(2):345-363. https://doi.org/10.3390/ejihpe13020026
Chicago/Turabian StyleFagbenro, Rasaki Kolawole, Riza Yosia Sunindijo, Chethana Illankoon, and Samuel Frimpong. 2023. "Influence of Prefabricated Construction on the Mental Health of Workers: Systematic Review" European Journal of Investigation in Health, Psychology and Education 13, no. 2: 345-363. https://doi.org/10.3390/ejihpe13020026
APA StyleFagbenro, R. K., Sunindijo, R. Y., Illankoon, C., & Frimpong, S. (2023). Influence of Prefabricated Construction on the Mental Health of Workers: Systematic Review. European Journal of Investigation in Health, Psychology and Education, 13(2), 345-363. https://doi.org/10.3390/ejihpe13020026