

The HOMESIDE Music Intervention: A Training Protocol for Family Carers of People Living with Dementia

 , , , , , , , , and
, , , , , , , , and
Abstract
1. Introduction
2. Methods
- (1)
- a series of case vignettes illustrating how dyads may benefit from the HOMESIDE intervention
- (2)
- rationale and benefits of the HOMESIDE music activities
- (3)
- music therapists’ perceptions of delivering the HOMESIDE music intervention
2.1. The HOMESIDE Music Intervention (MI)
2.1.1. Aims and Mechanisms
- provide caregivers with music resources to meet and support the psychosocial and functional care needs of their family member;
- enhance reciprocal verbal, non-verbal, and musical communications and human connection;
- reduce behavioural and psychological symptoms of dementia (e.g., agitation, apathy, depression);
- promote mental stimulation and meaningful experiences “in the here and now” for both members of the dyad;
- promote and maintain the person with dementia’s functional independence and engagement in personally satisfying and meaningful occupations; and
- validate both members of the dyad as individuals through recognition of their unique identity and history.
2.1.2. Indirect Music-Therapy Training Program
2.2. The HOMESIDE Music Activities
2.3. Data Collection
2.4. Method for Sub-Study 1: Case Vignettes
2.5. Method for Sub-Study 2: Rationale and Benefits of Music Activities (This Sub-Study Was Completed as Part of Sarah Crabtree’s PhD Research at Anglia Ruskin University)
2.5.1. Diary Method
2.5.2. Semi-Structured Interview Method
- What musical methods worked best for you?
- What (if any) benefits did you feel you got from this music program?
2.6. Method for Sub-Study 3: Music Therapists’ Perceptions of Delivering the HOMESIDE Music Intervention (This Sub-Study Was Completed as Part of Nina Wollersberger’s PhD Research at Anglia Ruskin University)
3. Results
3.1. Sub-Study 1 Results: Case Study Vignettes
3.1.1. Beth and Stephanie
“It’s brought me and my mam closer. There’s a connection there; it’s a non-verbal connection. It’s brought something back that we’d lost, that we used to find in doing other activities.”
“As she rested in bed, I massaged her feet and hands while we listened to a relaxation CD … I thought that she was asleep, but when I stopped … she said that it was lovely. She was just resting and relaxing with her eyes closed not asleep. Spending time with my mam this way was special. I felt emotional at one point as I thought about how much I would miss her when she passes.”
3.1.2. Jack and Lucy
“We now have music most of the time. [Jack] now joins in spontaneously, or initiates clapping, swaying, foot tapping, often smiling and laughing.” Later entries show that this developed into something they “wouldn’t be without”.
3.1.3. Julie and Kate
“Another good session. Definitely has a positive effect on mum. Seems to calm her down and cheer her up if she’s a bit down. I never thought that she would respond so positively.”
3.2. Sub-Study 2 Results: Rationale and Benefits of the HOMESIDE Music Activities
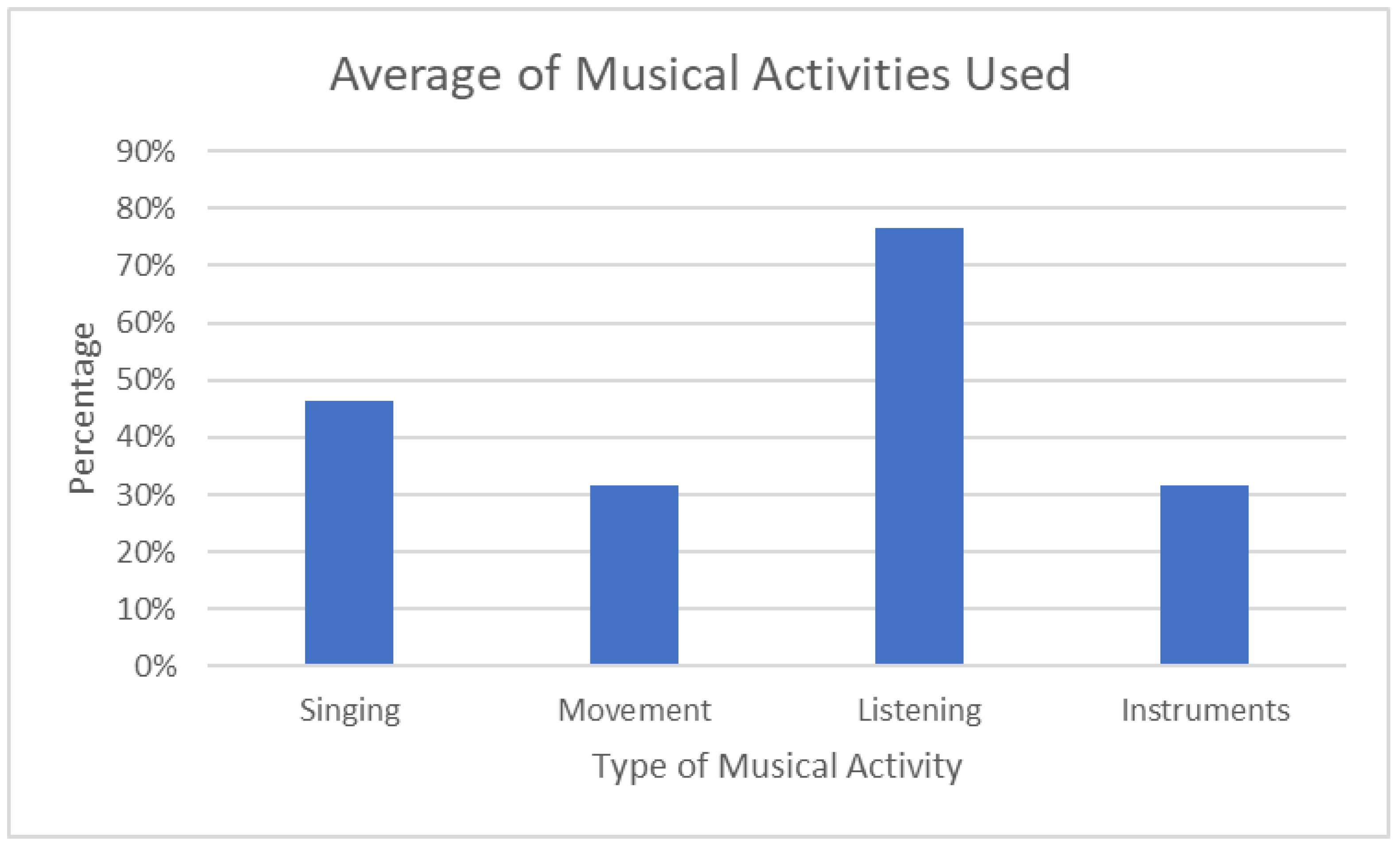
3.2.1. What Musical Methods Worked Best for You?
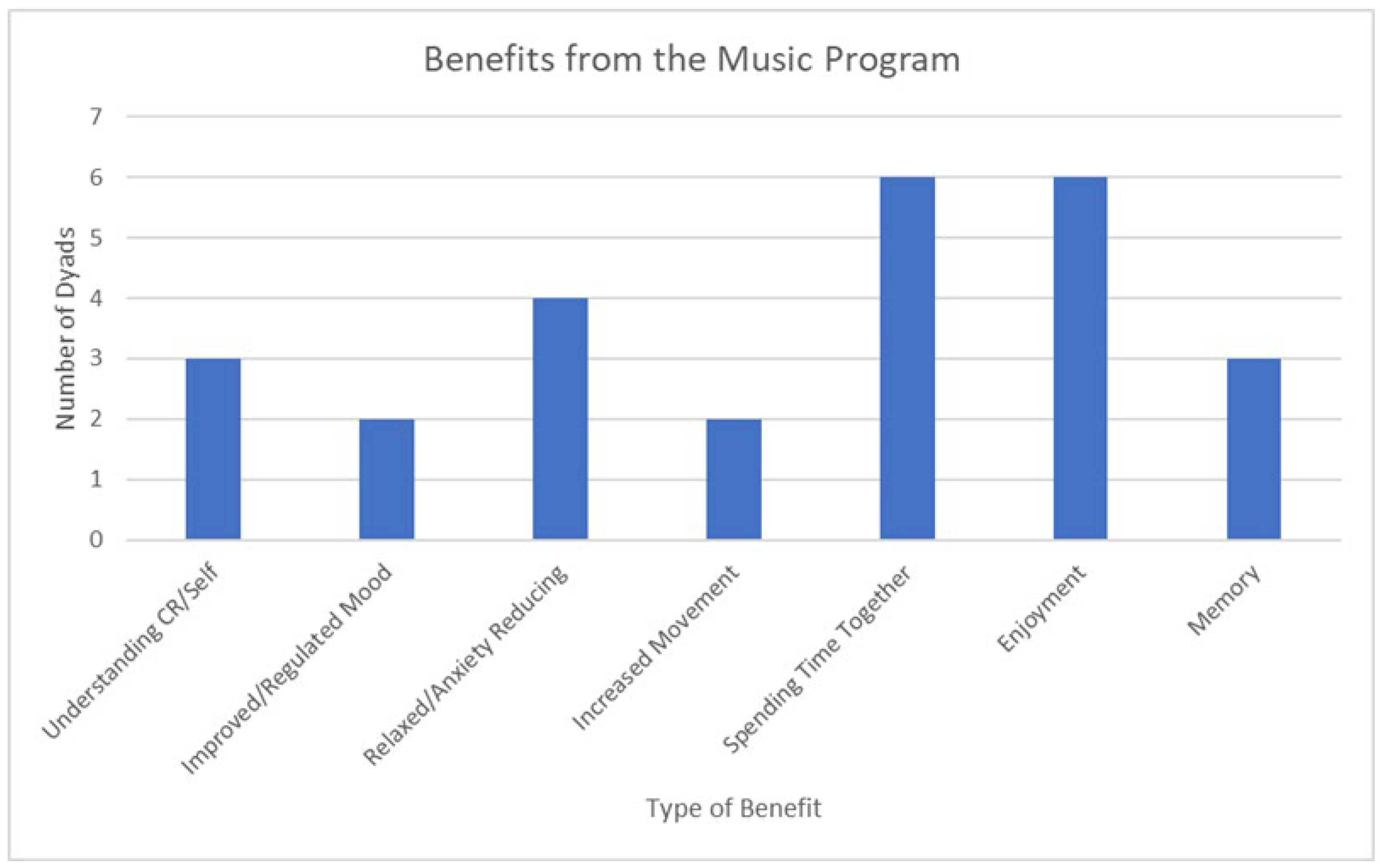
3.2.2. What (if Any) Benefits Did You Feel You Got from This Music Program?
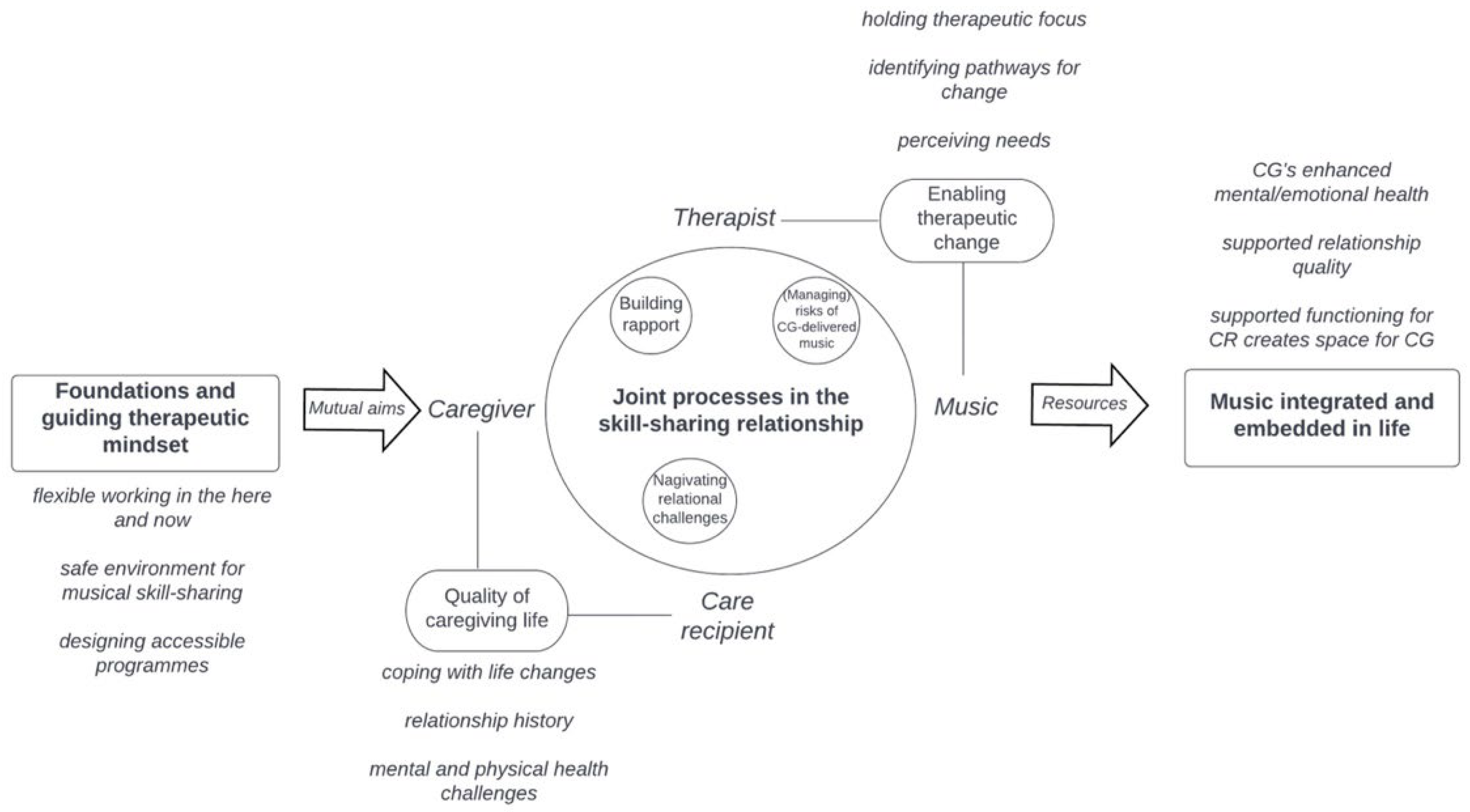
3.3. Sub-Study 3 Results: Music Therapists’ Perceptions of Delivering the HOMESIDE Music Intervention
4. Discussion
- Long sessions online may not be feasible for either member of the dyad. It can be easier and more acceptable to offer two to three shorter training sessions within the same week.
- Dyads are asked to prepare a place where they are comfortable and also able to see/hear the video/audio apparatus ahead of training sessions with the music therapist. The room should be free from any noise or disturbances and allow for movement without interference from obstacles such as furniture or rugs on the floor. It is also important the space is comfortable, and that the dyad can sit near one another, preferably opposite one another so they can make eye contact. Music equipment, pillows, blankets, and drinks/food should also be accessible.
- It is advisable to make a contingency plan with the dyad, such as having phones nearby in case internet connectivity or other technology issues interfere with the sessions.
- In some instances, it can be helpful for dyads to have a practice session before the first training to focus on technology issues related to music. This helps to reduce technology disruptions during the training.
- To protect privacy, music therapists should ensure that they are in a private location so that other people in their location are unable to overhear or see the session.
- When training sessions become unmanageable for the caregiver and/or PwD, the session is ended, and the music therapist follows up with a phone call later that day or the following day.
4.1. Strengths of the Intervention Noted by Music Interventionists So Far
4.2. Challenges Experienced So Far in Delivering the Music Intervention
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [PubMed]
- WHO. Dementia. Available online: https://www.who.int/health-topics/dementia#tab=tab_2 (accessed on 13 June 2022).
- WHO. Reveals Leading Causes of Death and Disability Worldwide: 2000–2019. Available online: https://www.who.int/news/item/09-12-2020-who-reveals-leading-causes-of-death-and-disability-worldwide-2000-2019 (accessed on 13 June 2022).
- Guerchet, M.; Ali, G.-C.; Prince, M.; Wu, Y.-T. The Incidence of dementia. In World Alzheimer Report 2015: The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2016; Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf (accessed on 5 January 2022).
- Arvanitakis, Z.; Bennett, D.A. What Is Dementia? JAMA 2019, 322, 1728. [Google Scholar] [CrossRef] [PubMed]
- Friedman, E.M.; Shih, R.A.; Langa, K.M.; Hurd, M.D. US prevalence and predictors of informal caregiving for dementia. Health Aff. 2015, 34, 1637–1641. [Google Scholar] [CrossRef] [PubMed]
- Jutkowitz, E.; Gaugler, J.E.; Trivedi, A.N.; Mitchell, L.L.; Gozalo, P. Family caregiving in the community up to 8-years after onset of dementia. BMC Geriatr. 2020, 20, 216. [Google Scholar] [CrossRef] [PubMed]
- Lewis, F.; Schaffer, S.K.; Sussex, J.; O’Neill, P.; Cockcroft, L. The Trajectory of Dementia in the UK-Making a Difference; Office of Health Economics Consulting Reports: London, UK, 2014. [Google Scholar]
- Ross, C.; Beattie, E. Caring for Someone with Dementia: The Economic, Social, and Health Impacts of Caring for and Evidence Based Supports for Carers. Talking about Alzheimer’s across Australia. 2014. Available online: https://www.fightdementia.org.au/files/NATIONAL/documents/Alzheimers-Australia-Numbered-Publication-42.pdf (accessed on 20 February 2022).
- Meyer, J.; Cullough, J.M.; Berggren, I. A phenomenological study of living with a partner affected with dementia. Br. J. Community Nurs. 2016, 21, 24–30. [Google Scholar] [CrossRef]
- Gorska, S.; Forsyth, K.; Maciver, D. Living with Dementia: A Meta-synthesis of Qualitative Research on the Lived Experience. Gerontologist 2018, 58, e180–e196. [Google Scholar] [CrossRef]
- Egilstrod, B.; Ravn, M.B.; Petersen, K.S. Living with a partner with dementia: A systematic review and thematic synthesis of spouses’ lived experiences of changes in their everyday lives. Aging Ment. Health 2019, 23, 541–550. [Google Scholar] [CrossRef]
- Greenblat, C. Dementia caregiving and caregivers. In Dementia: A Public Health Priority; Bramley, D., Ed.; World Health Organisation: Geneva, Switzerland, 2012; pp. 67–80. Available online: http://apps.who.int/iris/bitstream/10665/75263/1/9789241564458_eng.pdf?ua=1 (accessed on 7 November 2021).
- Sheehan, O.C.; Haley, W.E.; Howard, V.J.; Huang, J.; Rhodes, J.D.; Roth, D.L. Stress, burden, and well-being in dementia and nondementia caregivers: Insights from the caregiving transitions study. Gerontologist 2020, 61, 670–679. [Google Scholar] [CrossRef]
- Van Bruggen, S.; Gussekloo, J.; Bode, C.; Touwen, D.P.; Engberts, D.P.; Blom, J.W. Problems experienced by informal caregivers with older care recipients with and without cognitive impairment. Home Health Care Serv. Q. 2016, 35, 11–24. [Google Scholar] [CrossRef]
- McGillick, J.; Murphy-White, M. Experiences and perspectives of family caregivers of the person with dementia. In Dementia Care: An Evidence-Based Approach; Boltz, M., Galvin, J.E., Eds.; Springer International Publishing: New York, NY, USA, 2016; pp. 198–214. [Google Scholar] [CrossRef]
- Terum, T.M.; Testad, I.; Rongve, A.; Aarsland, D.; Svendsboe, E.; Andersen, J.R. The association between aspects of carer distress and time until nursing home admission in persons with Alzheimer’s disease and dementia with Lewy bodies. Int. Psychogeriatr. 2021, 33, 337–345. [Google Scholar] [CrossRef]
- Toot, S.; Swinson, T.; Devine, M.; Challis, D.; Orell, M. Causes of nursing home placement for older people with dementia: A systematic review and meta-analysis. Int. Psychogeriatr. 2017, 29, 195–208. [Google Scholar] [CrossRef]
- Groen-van de Ven, L.; Smits, C.; Oldewarris, K.; Span, M.; Jukema, J.; Eefsting, J.; Vernooij-Dassen, M. Decision Trajectories in Dementia Care Networks: Decisions and Related Key Events. Res. Aging 2017, 39, 1039–1071. [Google Scholar] [CrossRef]
- Rippon, I.; Quinn, C.; Martyr, A.; Morris, R.; Nelis, S.M.; Jones, R.I.; Victor, C.R.; Clare, L. The impact of relationship quality on life satisfaction and well-being in dementia caregiving dyads: Findings from the IDEAL study. Aging Ment. Health 2020, 24, 1411–1420. [Google Scholar] [CrossRef]
- Wadham, O.; Simpson, J.; Rust, J.; Murray, C. Couples’ shared experiences of dementia: A meta-synthesis of the impact upon relationships and couplehood. Aging Ment. Health 2016, 20, 463–473. [Google Scholar] [CrossRef]
- Cheng, S.T.; Li, K.K.; Losada, A.; Zhang, F.; Au, A.; Thompson, L.W.; Gallagher-Thompson, D. The effectiveness of nonpharmacological interventions for informal dementia caregivers: An updated systematic review and meta-analysis. Psychol. Aging. 2020, 35, 55–77. [Google Scholar] [CrossRef]
- Alves, G.S.; Casali, M.E.; Veras, A.B.; Carrilho, C.G.; Costa, E.B.; Rodrigues, V.M.; Dourado, M.C.N. A systematic review of home-setting psychoeducation interventions for behavioral changes in dementia: Some lessons for the COVID-19 pandemic and post-pandemic assistance. Front. Psychiatry 2020, 11, 577871. [Google Scholar] [CrossRef]
- Lee, D.-C.A.; Tirlea, L.; Haines, T.P. Non-pharmacological interventions to prevent hospital or nursing home admissions among community-dwelling older people with dementia: A systematic review and meta-analysis. Health Soc. Care Community 2020, 28, 1408–1429. [Google Scholar] [CrossRef]
- McDermott, O.; Ridder, H.M.; Baker, F.A.; Wosch, T.; Ray, K.; Stige, B. Indirect Music Therapy Practice and Skill-Sharing in Dementia Care. J. Music Ther. 2018, 55, 255–279. [Google Scholar] [CrossRef]
- Odell-Miller, H.; Ridder, H.M.O.; Schmid, W. The many futures of music therapy in dementia care and neurorehabilitation. Approaches Interdiscip. J. Music. Ther. 2017, 9, 25–27. [Google Scholar]
- Hsu, M.H.; Flowerdew, R.; Parker, M.; Fachner, J.; Odell-Miller, H. Individual music therapy for managing neuropsychiatric symptoms for people with dementia and their carers: A cluster randomised controlled feasibility study. BMC Geriatr. 2015, 15, 84. [Google Scholar] [CrossRef]
- Hammar, L.M.; Emami, A.; Gotell, E.; Engstrom, G. The impact of caregivers’ singing on expressions of emotion and resistance during morning care situations in persons with dementia: An intervention in dementia care. J. Clin. Nurs. 2011, 20, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.; Dassa, A.; Maier, J.; Davis, R.; Ogunlade, O. Caring for individuals with dementia on a continuum: An interdisciplinary approach between music therapy and nursing. In Update on Dementia; Intechopen: London, UK, 2016. [Google Scholar] [CrossRef]
- Hammar, L.M.; Emami, A.; Engstrom, G.; Gotell, E. Reactions of persons with dementia to caregivers singing in morning care situations. Open Nurs. J. 2010, 4, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Swall, A.; Hammar, L.M.; Gransjon Craftman, A. Like a bridge over troubled water—A qualitative study of professional caregiver singing and music as a way to enable person-centred care for persons with dementia. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1735092. [Google Scholar] [CrossRef]
- Baker, F.A.; Grocke, D.; Pachana, N.A. Connecting through music: A study of a spousal caregiver-directed music intervention designed to prolong fulfilling relationships in couples where one person has dementia. Aust. J. Music. Ther. 2012, 23, 4–21. [Google Scholar]
- Hanser, S.B.; Butterfield-Whitcomb, J.; Kawata, M.; Collins, B.E. Home-based music strategies with individuals who have dementia and their family caregivers. J. Music. Ther. 2011, 48, 2–27. [Google Scholar] [CrossRef]
- Baker, F.A.; Bloska, J.; Braat, S.; Bukowska, A.; Clark, I.N.; Hsu, M.H.; Kvamme, T.; Lautenschlager, N.; Lee, Y.C.; Smrokowska-Reichmann, A.; et al. HOMESIDE: Home-based family caregiver-delivered music and reading interventions for people living with dementia: Protocol of a randomised controlled trial. BMJ Open 2019, 9, e031332. [Google Scholar] [CrossRef]
- Jacobsen, J.-H.; Stelzer, J.; Fritz, T.H.; Chételat, G.; La Joie, R.; Turner, R. Why musical memory can be preserved in advanced Alzheimer’s disease. Brain 2015, 138, 2438–2450. [Google Scholar] [CrossRef]
- Muthesius, D.; Sonntag, J.; Warme, B.; Falk, J. Musik–Demenz–Begegnung; Mabuse-Verlag: Frankfurt, Germany, 2019. [Google Scholar]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Maidenhead, UK, 1997. [Google Scholar]
- Feil, N. Validation; Ernst Reinhardt Verlag: Frankfurt, Germany, 2015. [Google Scholar]
- Ridder, H.M.O. Singing Dialogue: Music Therapy with Persons in Advanced Stages of Dementia. A Case Study Research Design. Ph.D. Thesis, Aalborg Universitet, Aalborg, Denmark, 2003. Available online: https://vbn.aau.dk/ws/portalfiles/portal/316419630/ridder_2003.pdf (accessed on 22 June 2019).
- Wosch, T. Musik und Alter in Therapie und Pflege. Grundlagen, Institutionen und Praxis der Musiktherapie im Alter und bei Demenz; Kohlhammer: Stuttgart, Germany, 2011. [Google Scholar]
- Werner, J.; Wosch, T.; Gold, C. Effectiveness of group music therapy versus recreational group singing for depressive symptoms of elderly nursing home residents: Pragmatic trial. Aging Ment. Health 2017, 21, 147–155. [Google Scholar] [CrossRef]
- Odell-Miller, H. Embedding music and music therapy in care pathways for people with dementia in the 21st Century—A position paper. Music Sci. 2021, 4. [Google Scholar] [CrossRef]
- Clark, I.N.; Tamplin, J.; Baker, F.A. Community-dwelling people living with dementia and their family caregivers’ experiences of therapeutic group singing: A qualitative thematic analysis. Front. Psychol. 2018, 9, 1332. [Google Scholar] [CrossRef]
- Tamplin, J.; Clark, I.N.; Lee, Y.C.; Baker, F.A. Remini-Sing: A Feasibility Study of Therapeutic Group Singing to Support Relationship Quality and Wellbeing for Community-Dwelling People Living with Dementia and Their Family Caregivers. Front. Med. 2018, 5, 245. [Google Scholar] [CrossRef]
- Kales, H.C.; Gitlin, L.N.; Lyketsos, C.G. Management of neuropsychiatric symptoms of dementia in clinical settings: Recommendations from a multidisciplinary expert panel. J. Am. Geriatr. Soc. 2014, 62, 762–769. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Crabtree, S. The Rationale for the Use of Singing, Listening, Playing Instruments, and Movement with Music for People Living with Dementia. Ph.D. Thesis, Anglia Ruskin University, Cambridge, UK, 2022. [Google Scholar]
- Wollersberger, N. Exploring the Impact of an Indirect Music Therapy Intervention on Quality of Life for Informal Caregivers of People Living with Dementia in the Community. Ph.D. Thesis, Anglia Ruskin University, Cambridge, UK, 2022. [Google Scholar]
- Bowell, S.; Bamford, S.M. What Would Life Be–Without a Song or a Dance, What Are We? A Report from the Commission on Dementia and Music; The International Longevity Centre: London, UK, 2018. [Google Scholar]
- Fancourt, D.; Finn, S. What is the Evidence on the Role of the Arts in Improving Health and Well-Being? A Scoping Review. Nord. J. Arts Cult. Health 2018, 2, 77–83. Available online: https://www.euro.who.int/en/publications/abstracts/what-is-the-evidence-on-the-role-of-the-arts-in-improving-health-andwell-being-a-scoping-review-2019 (accessed on 15 August 2021).
- World Dementia Council. Global Dialogue on Care. The Dementia Landscape Project. 2021. (Transcript). Available online: https://worlddementiacouncil.org/sites/default/files/2021-04/DLP%20-%20Transcript%20-%20Care.pdf (accessed on 5 June 2022).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Increasing and maintaining engagement | Combining two activities, for example, singing and dancing/movement, may provide additional stimulation and encourage increased engagement Music that orients to activities such as songs about cooking, showering, etc., can assist in task engagement Repeat or extend activities that are evidently enjoyed or creating a meaningful response (for example, replaying a song) |
| Regulating arousal and managing agitation | If the PwD is agitated, try to choose music that matches the energy of the agitation Stereotypical movements can be regulated by engaging the person with dementia’s attention to the sound of an instrument (e.g., striking a drum) and inviting them to play During moments of frustration, the caregiver could initiate active music interventions such as singing, dancing/movement to music, instrument playing, or body percussion to expel agitated energy and regulate arousal When behaviours are verbally or physically aggressive, it may indicate that the music is too stimulating, loud, emotionally disturbing, or disliked. In such cases, introduce a different music selection or gently terminate the musical activity. If the aggression continues, they might move to another activity, preferably relaxation with music, or consider taking a break from the music intervention. |
| Safe reminiscence | When music evokes painful memories and causes distress, stop or change the music/activity, and/or be as supportive as possible throughout Photographs or images are invaluable resources to support memory recall and reminiscence |
| Dyad Number | Number of Diary Entries | Number of Sessions Dyad Used Singing | Number of Sessions Dyad Used Movement | Number of Sessions Dyad Used Listening | Number of Sessions Dyad Used Instruments | Percentage of Positive Shared Experiences | Percentage of Positive Effects over the Day |
|---|---|---|---|---|---|---|---|
| 1 | 34 | 0 | 0 | 33 | 0 | 68% | 56% |
| 2 | 38 | 2 | 6 | 34 | 3 | 89% | 79% |
| 3 | 33 | 51 | 21 | 59 | 30 | 100% | 100% |
| 4 | 62 | 39 | 43 | 57 | 24 | 60% | 65% |
| 5 | 71 | 20 | 4 | 26 | 22 | 93% | 85% |
| 6 | 28 | 58 | 59 | 60 | 38 | 93% | 89% |
| 7 | 79 | 5 | 7 | 38 | 0 | 90% | 89% |
| 8 | 50 | 31 | 24 | 31 | 23 | 76% | 56% |
| 9 | 76 | 11 | 14 | 30 | 5 | 43% | 34% |
| 10 | 31 | 71 | 3 | 71 | 68 | 71% | 71% |
| 11 | 98 | 14 | 6 | 10 | 10 | 82% | 81% |
| 12 | 58 | 29 | 23 | 48 | 23 | 97% | 83% |
| 13 | 84 | 41 | 70 | 73 | 13 | 82% | 69% |
| 14 | 67 | 30 | 11 | 36 | 12 | 78% | 55% |
| 15 | 67 | 22 | 6 | 54 | 7 | 84% | 64% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odell-Miller, H.; Blauth, L.; Bloska, J.; Bukowska, A.A.; Clark, I.N.; Crabtree, S.; Engen, R.B.; Knardal, S.; Kvamme, T.K.; McMahon, K.; et al. The HOMESIDE Music Intervention: A Training Protocol for Family Carers of People Living with Dementia. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1812-1832. https://doi.org/10.3390/ejihpe12120127
Odell-Miller H, Blauth L, Bloska J, Bukowska AA, Clark IN, Crabtree S, Engen RB, Knardal S, Kvamme TK, McMahon K, et al. The HOMESIDE Music Intervention: A Training Protocol for Family Carers of People Living with Dementia. European Journal of Investigation in Health, Psychology and Education. 2022; 12(12):1812-1832. https://doi.org/10.3390/ejihpe12120127
Chicago/Turabian StyleOdell-Miller, Helen, Laura Blauth, Jodie Bloska, Anna A. Bukowska, Imogen N. Clark, Sarah Crabtree, Runa B. Engen, Solgunn Knardal, Tone K. Kvamme, Kate McMahon, and et al. 2022. "The HOMESIDE Music Intervention: A Training Protocol for Family Carers of People Living with Dementia" European Journal of Investigation in Health, Psychology and Education 12, no. 12: 1812-1832. https://doi.org/10.3390/ejihpe12120127
APA StyleOdell-Miller, H., Blauth, L., Bloska, J., Bukowska, A. A., Clark, I. N., Crabtree, S., Engen, R. B., Knardal, S., Kvamme, T. K., McMahon, K., Petrowitz, C., Smrokowska-Reichmann, A., Stensæth, K., Tamplin, J., Wosch, T., Wollersberger, N., & Baker, F. A. (2022). The HOMESIDE Music Intervention: A Training Protocol for Family Carers of People Living with Dementia. European Journal of Investigation in Health, Psychology and Education, 12(12), 1812-1832. https://doi.org/10.3390/ejihpe12120127