
COVID-19 Lockdown-Related Changes in Mood, Health and Academic Functioning

 , , , and
, , , and 
Abstract
:1. Introduction
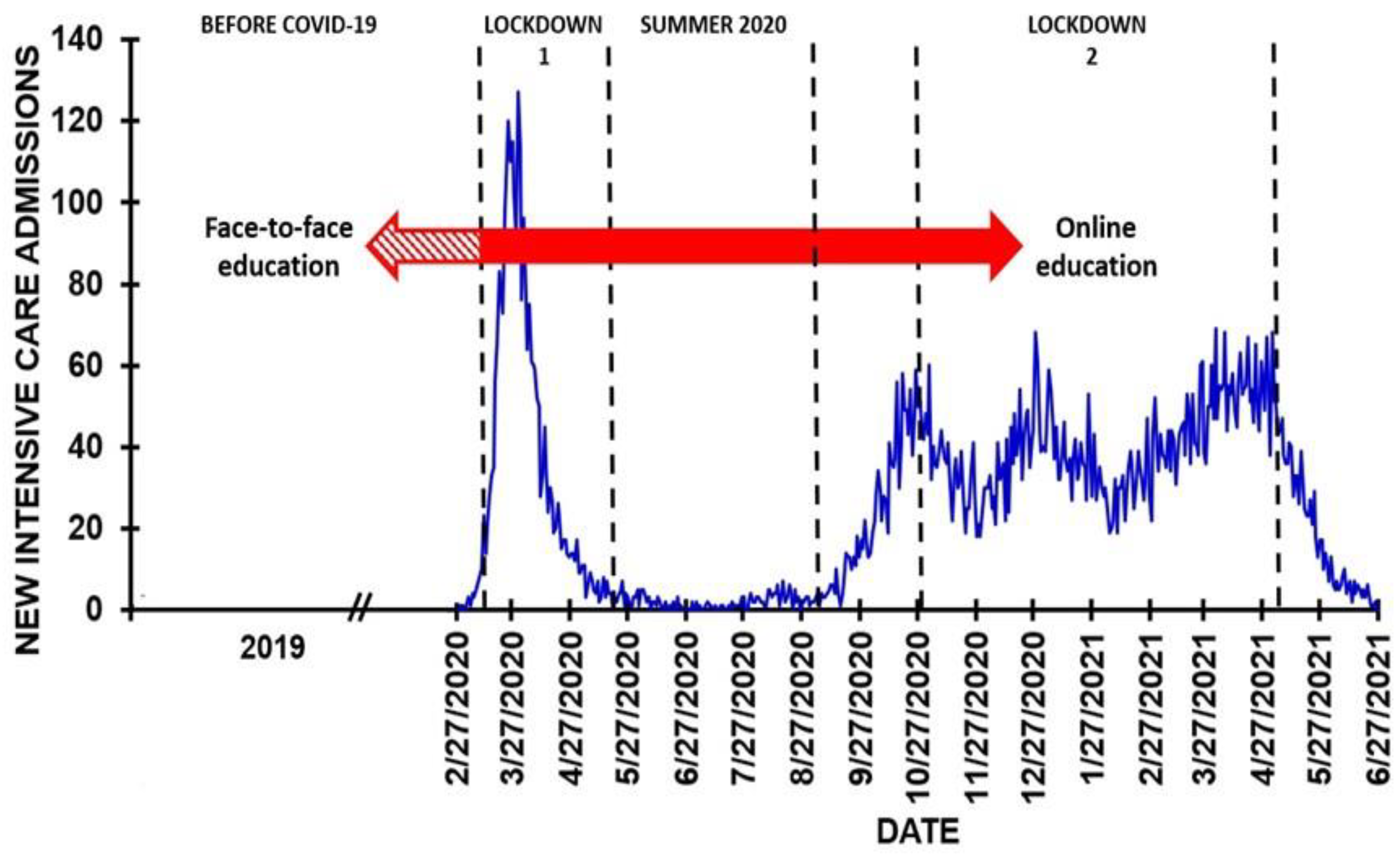
1.1. The COVID-19 Pandemic in the Netherlands
1.2. Education at the Department of Pharmaceutical Sciences
1.3. Aims of the Study
2. Materials and Methods
2.1. Survey Content
2.1.1. Demographics
2.1.2. Mood
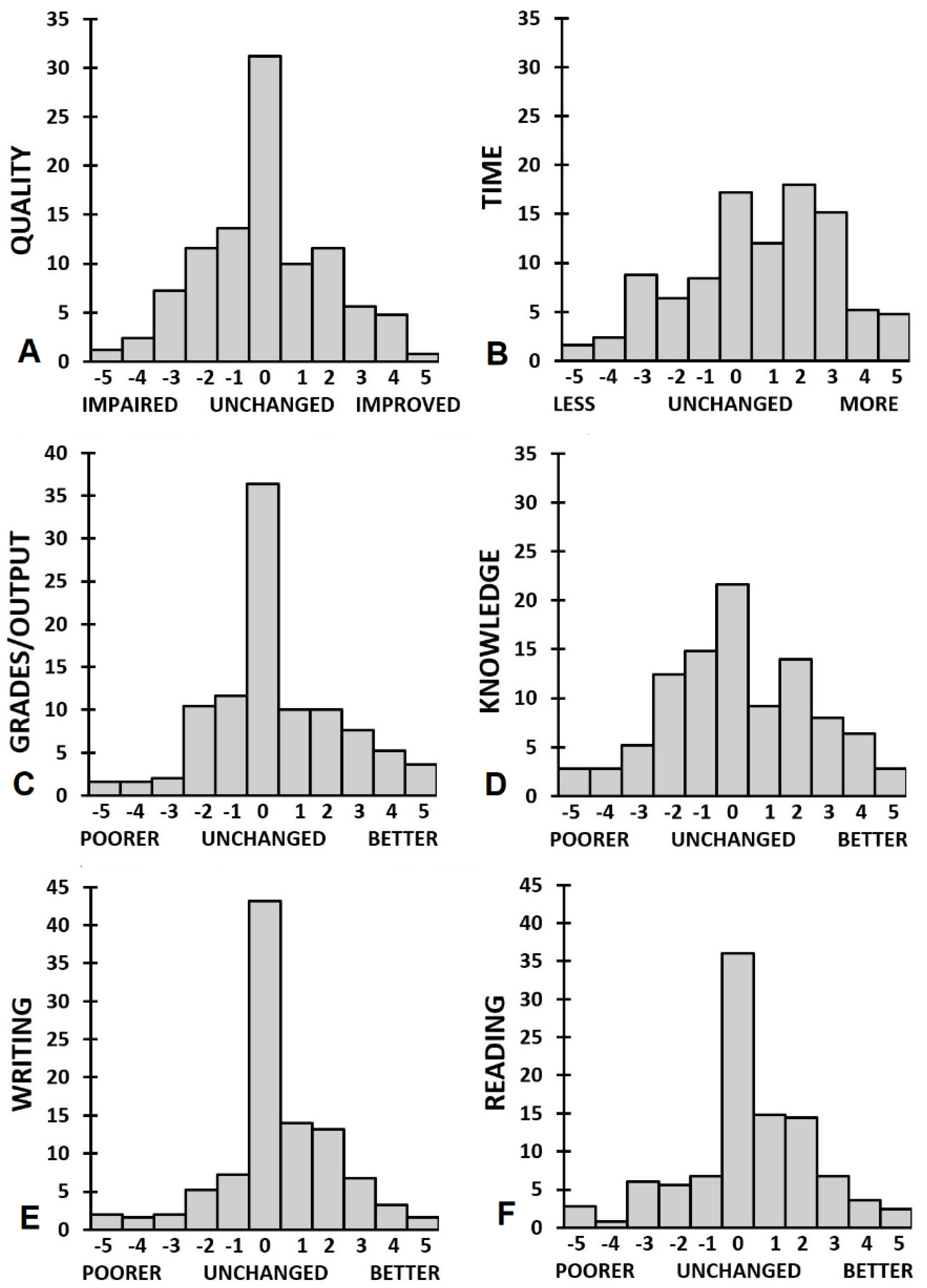
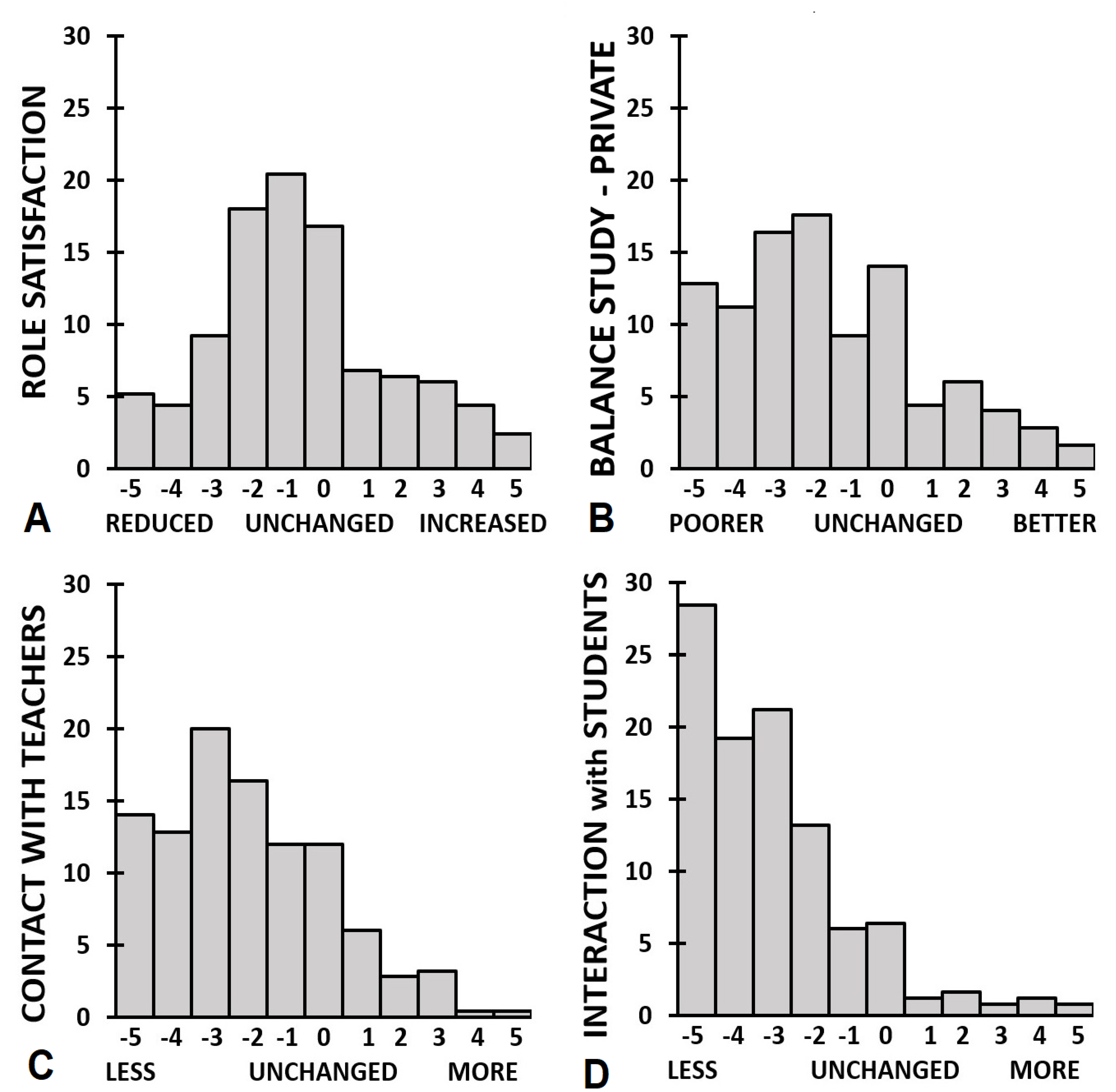
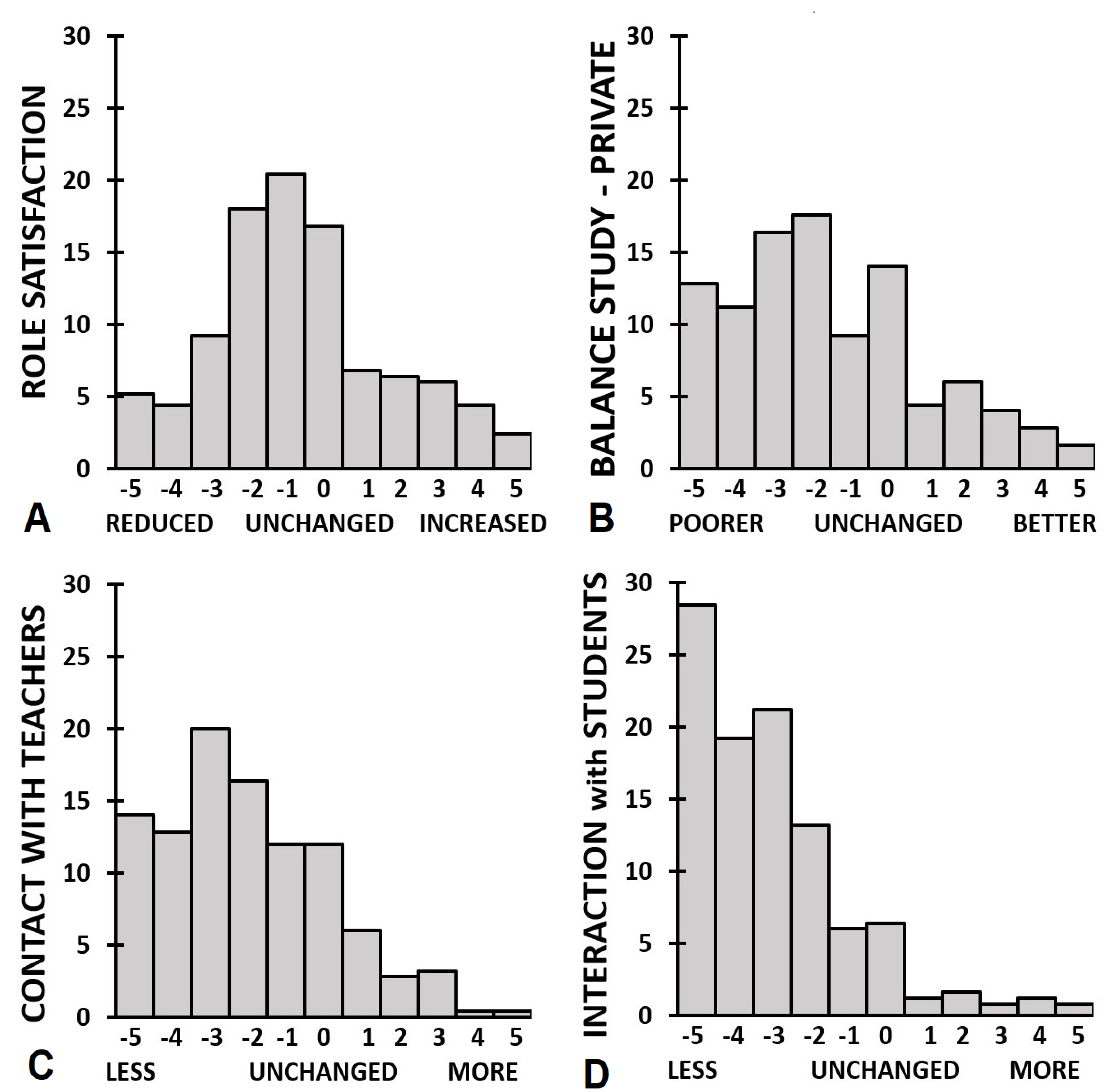
2.1.3. Academic Functioning
2.1.4. Sleep and Being Active
2.1.5. Quality of Life
2.1.6. Perceived Immune Fitness
2.2. Statistical Analysis
3. Results
3.1. Sex Differences
3.2. Ethnicity
3.3. Living Situation
3.4. Health Correlates
3.5. Predicting Improved Versus Poorer Academic Functioning
4. Discussion
4.1. Limitations
4.2. Implications
4.3. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- Crawford, J.; Butler-Henderson, K.; Rudolph, J.; Malkawi, B.; Glowatz, M.; Burton, R.; Magni, P.A.; Lam, S. COVID-19: 20 countries’ higher education intra-period digital pedagogy responses. J. Appl. Learn. Teach. 2020, 3, 9–28. [Google Scholar]
- UNESCO. COVID-19 Educational Disruption and Response. Available online: https://en.unesco.org/news/covid-19-educational-disruption-and-response (accessed on 25 June 2021).
- Nurunnabi, M.; Almusharraf, N.; Aldeghaither, D. Mental health and well-being during the COVID-19 pandemic in higher education: Evidence from G20 countries. J. Publ. Health Res. 2021, 9, 2010. [Google Scholar] [CrossRef]
- Tasso, A.F.; Hisli Sahin, N.; San Roman, G.J. COVID-19 disruption on college students: Academic and socioemotional implications. Psychol. Trauma 2021, 13, 9–15. [Google Scholar] [CrossRef]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenèvre, P.; et al. Factors associated with mental health disorders among university students in France confined during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiat. Res. 2021, 301, 113863. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Patten, S.B. Age of onset of mental disorders. Can. J. Psychiat. 2017, 62, 235–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prowse, R.; Sherratt, F.; Abizaid, A.; Gabrys, R.L.; Hellemans, K.G.C.; Patterson, Z.R.; McQuaid, R.J. Coping with the COVID-19 pandemic: Examining gender differences in stress and mental health among university students. Front. Psychiat. 2021, 12, 439. [Google Scholar] [CrossRef]
- Bolatov, A.K.; Seisembekov, T.Z.; Askarova, A.Z.; Baikanova, R.K.; Smailova, D.S.; Fabbro, E. Online-learning due to COVID-19 improved mental health among medical students. Med. Sci. Educ. 2020, 31, 183–192. [Google Scholar] [CrossRef]
- Gallego-Gómez, J.I.; Campillo-Cano, M.; Carrión-Martínez, A.; Balanza, S.; Rodríguez-González-Moro, M.T.; Simonelli-Muñoz, A.J.; Rivera-Caravaca, J.M. The COVID-19 pandemic and its impact on homebound nursing students. Int. J. Environ. Res. Public Health 2020, 17, 7383. [Google Scholar] [CrossRef]
- Radu, M.-C.; Schnakovszky, C.; Herghelegiu, E.; Ciubotariu, V.-A.; Cristea, I. The impact of the COVID-19 pandemic on the quality of educational process: A student survey. Int. J. Environ. Res. Public Health 2020, 17, 7770. [Google Scholar] [CrossRef] [PubMed]
- Sundarasen, S.; Chinna, K.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Khoshaim, H.B.; Hossain, S.F.A.; Sukayt, A. Psychological impact of COVID-19 and lockdown among university students in Malaysia: Implications and policy recommendations. Int. J. Environ. Res. Public Health 2020, 17, 6206. [Google Scholar] [CrossRef]
- Rohmani, N.; Andriani, R. Correlation between academic self-efficacy and burnout originating from distance learning among nursing students in Indonesia during the coronavirus disease 2019 pandemic. J. Educ. Eval. Health Prof. 2021, 18, 9. [Google Scholar] [CrossRef]
- Hanafy, S.M.; Jumaa, M.I.; Arafa, M.A. A comparative study of online learning in response to the coronavirus disease 2019 pandemic versus conventional learning. Saudi Med. J. 2021, 42, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Liguori, E.; Winkler, C. From offline to online: Challenges and opportunities for entrepreneurship education following the COVID-19 pandemic. Entrep. Educ. Pedagog. 2020, 3, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Sani, I.; Hamza, Y.; Chedid, Y.; Amalendran, J.; Hamza, N. Understanding the consequence of COVID-19 on undergraduate medical education: Medical students’ perspective. Ann. Med. Surg. 2020, 58, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Kebritchi, M.; Lipschuetz, A.; Santiague, L. Issues and challenges for teaching successful online courses in higher education: A literature review. J. Educ. Technol. Syst. 2017, 46, 4–29. [Google Scholar] [CrossRef]
- De Haas, M.; Faber, R.; Hamersma, M. How COVID-19 and the Dutch “intelligent lockdown” change activities, work, and travel behaviour: Evidence from longitudinal data in the Netherlands. Transp. Res. Interdiscip. Perspect. 2020, 6, 100150. [Google Scholar] [CrossRef]
- Elzainy, A.; El Sadik, A.; Al Abdulmonem, W. Experience of e-learning and online assessment during the COVID-19 pandemic at the College of Medicine, Qassim University. J. Taibah Univ. Med. Sci. 2020, 15, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, T.; de la Rubia, M.A.; Hincz, K.P.; Comas-Lopez, M.; Subirats, L.; Fort, S.; Sacha, G.M. Influence of COVID-19 confinement on students’ performance in higher education. PLoS ONE 2020, 15, e0239490. [Google Scholar] [CrossRef]
- Clarke, C.; Mullin, M.; McGrath, D.; Farrelly, N. University students and study habits. Ir. J. Psychol. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Foo, C.-C.; Cheung, B.; Chu, K.-M. A comparative study regarding distance learning and the conventional face-to-face approach conducted problem-based learning tutorial during the COVID-19 pandemic. BMC Med. Educ. 2021, 21, 141. [Google Scholar] [CrossRef] [PubMed]
- Brockfeld, T.; Muller, B.; de Laffolie, J. Video versus live lecture courses: A comparative evaluation of lecture types and results. Med. Educ. Online 2018, 23, 1555434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlesselman, L.S.; Cain, J.; DiVall, M. The COVID-19 pandemic across the academy. Improving and restoring the well-being and resilience of pharmacy students during a pandemic. Am. J. Pharm. Educ. 2020, 84, 8144. [Google Scholar] [CrossRef]
- Wilczewski, M.; Gorbaniuk, O.; Giuri, P. The psychological and academic effects of studying from the home and host country during the COVID-19 pandemic. Front. Psychol. 2021, 12, 644096. [Google Scholar] [CrossRef]
- John, R.R.; John, R.P. Impact of lockdown on the attitude of university students in South India -A cross-sectional observational study. J. Maxillofac. Oral Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- McQuaid, R.J.; Cox, S.; Ogunlana, A.; Jaworska, N. The burden of loneliness: Implications of the social determinants of health during COVID-19. Psychiat. Res. 2020, 296, 113648. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- RIVM. COVID-19 Intensive Care-Opnames (IC) in Nederland per IC-Opnamedatum en Meldingsdatum (Volgens NICE Registratie). Available online: https://data.rivm.nl/geonetwork/srv/dut/catalog.search#/metadata/45f911c4-3a62-42f1-b594-524a75db2c94 (accessed on 29 June 2021).
- Hsiao, Y.-C. Impacts of course type and student gender on distance learning performance: A case study in Taiwan. Educ. Inf. Technol. 2021, 26, 6807–6822. [Google Scholar] [CrossRef]
- Elfferich, A.; Geurts, M.; Thravalou, E.; van Tuijl, P. The Experience of International Students at Dutch Higher Education Institutions during the COVID-19 Pandemic; Nuffic: The Hague, The Netherlands, 2021. [Google Scholar]
- Hendriksen, P.A.; Merlo, A.; Bijlsma, E.Y.; Engels, F.; Garssen, J.; Bruce, G.; Verster, J.C. COVID-19 Lockdown Effects on Academic Functioning, Mood, and Health Correlates: Data from Dutch Pharmacy Students, PhD Candidates and Postdocs. Data 2021, 6, 120. [Google Scholar] [CrossRef]
- Statistics Netherlands (Centraal Bureau voor de Statistiek, CBS). Wat Is Het Verschil Tussen EenWesterse en Niet-Westerse Allochtoon? Available online: https://www.cbs.nl/nl-nl/faq/specifiek/wat-is-het-verschil-tussen-een-westerse-en-niet-westerse-allochtoon (accessed on 26 June 2021).
- Verster, J.C.; Sandalova, E.; Garssen, J.; Bruce, G. The use of single-item ratings versus traditional multiple-item questionnaires to assess mood and health. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 183–198. [Google Scholar] [CrossRef]
- Kiani, P.; Merlo, A.; Saeed, H.M.; Benson, S.; Bruce, G.; Hoorn, R.; Kraneveld, A.D.; Severeijns, N.R.; Sips, A.S.M.; Scholey, A.; et al. Immune fitness, and the psychosocial and health consequences of the COVID-19 pandemic lockdown in The Netherlands: Methodology and design of the CLOFIT study. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 199–218. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Arnoldy, L.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. The impact of mood and subjective intoxication on hangover severity. J. Clin. Med. 2020, 9, 2462. [Google Scholar] [CrossRef] [PubMed]
- Baars, T.; Berge, C.; Garssen, J.; Verster, J.C. Effect of raw milk consumption on perceived health, mood and immune functioning among US adults with a poor and normal health: A retrospective questionnaire based study. Complement. Ther. Med. 2019, 47, 102196. [Google Scholar] [CrossRef] [PubMed]
- Donners, A.A.M.T.; Tromp, M.D.P.; Garssen, J.; Roth, T.; Verster, J.C. Perceived immune status and sleep: A survey among Dutch students. Sleep Disord. 2015, 2015, 721607. [Google Scholar] [CrossRef] [Green Version]
- Tromp, M.D.P.; Donners, A.A.M.T.; Garssen, J.; Verster, J.C. Sleep, eating disorder symptoms, and daytime functioning. Nat. Sci. Sleep 2016, 8, 35–40. [Google Scholar]
- Wilod Versprille, L.J.F.; van de Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.A.; Abdulahad, S.; Huls, H.; Baars, T.; Kraneveld, A.D.; et al. Development and validation of the Immune Status Questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, 4743. [Google Scholar] [CrossRef] [Green Version]
- Van Schrojenstein Lantman, M.; Otten, L.S.; Mackus, M.; de Kruijff, D.; van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Mental resilience, perceived immune functioning, and health. J. Multidiscip. Healthc. 2017, 10, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Abdulahad, S.; Huls, H.; Balikji, S.; van de Loo, A.J.A.E.; Roth, T.; Verster, J.C. Irritable bowel syndrome, immune fitness and insomnia: Results from an online survey among people with sleep complaints. Sleep Vigil. 2019, 3, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Azeiteiro, U.M.; Bacelar-Nicolau, P.; Caetano, F.J.P.; Caeiro, S. Education for sustainable development through elearning in higher education: Experiences from Portugal. J. Clean. Prod. 2015, 106, 308–319. [Google Scholar] [CrossRef]
- Lee, J.; Song, H.D.; Hong, J.A. Exploring factors, and indicators for measuring students’ sustainable engagement in e-learning. Sustainability 2019, 11, 985. [Google Scholar] [CrossRef] [Green Version]
- Dubey, A.D.; Tripathi, S. Analysing the Sentiments towards work-from-home experience during COVID-19 Pandemic. J. Innov. Manag. 2020, 8, 13–19. [Google Scholar] [CrossRef]
- Brown, B.W.; Liedholm, C.E. Can web courses replace the classroom in principles of microeconomics? Am. Econ. Rev. 2002, 92, 444–448. [Google Scholar] [CrossRef]
- Bernard, R.M.; Abrami, P.C.; Lou, Y.; Borokhovski, E.; Wade, A.; Wozney, L.; Wallet, P.A.; Fiset, M.; Huang, B. How does distance education compare to classroom instruction? A meta-analysis of the empirical literature. Rev. Educ. Res. 2004, 74, 379–439. [Google Scholar] [CrossRef] [Green Version]
- Wagner, S.C.; Garippo, S.J.; Lovaas, P. A longitudinal comparison of online versus traditional instruction. MERLOT J. Online Learn. Teach. 2011, 7, 68–73. [Google Scholar]
- Georgoulias, P.; Angelidis, G.; Valotassiou, V.; Tsougos, I. COVID-19 crisis: Will online learning have negative consequences to our students? Cardiol. Young 2021, 31, 511. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Key Figures on Europe. Luxembourg: Publications Office of the European Union. 2021. Available online: https://ec.europa.eu/eurostat/documents/3217494/13394938/KS-EI-21-001-EN-N.pdf/ad9053c2-debd-68c0-2167-f2646efeaec1?t=1632300620367 (accessed on 9 October 2021).
- Bozkurt, A.; Sharma, R.C. On the verge of a new renaissance: Care and empathy oriented, human-centered pandemic pedagogy. Asian J. Distance Educ. 2021, 16, i–vii. [Google Scholar]
- Karakaya, K. Design considerations in emergency remote teaching during the COVID-19 pandemic: A human-centered approach. Educ. Technol. Res. Dev. 2021, 69, 295–299. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Study Outcome |
|---|---|
| n | 341 |
| Male/Female | 85 (24.9%)/256 (75.1%) |
| Age (years) | 23.0 (4.2) |
| Ethnicity | |
| —Dutch | 223 (65.8%) |
| —Western migration background | 37 (10.9%) |
| —Non-Western migration background | 79 (23.3%) |
| Living situation | |
| Alone | 41 (12.0%) |
| Together with others (students, friends) | 131 (38.4%) |
| Together with family | 169 (49.6%) |
| Educational level | |
| —Bachelor pharmacy or CPS | 179 (52.5%) |
| —Master pharmacy | 117 (34.3%) |
| —PhD candidate | 39 (11.4%) |
| —Postdoctoral researcher | 6 (1.8%) |
| Variable | Before COVID-19 | First Lockdown | Summer 2020 (No Lockdown) | Second Lockdown |
|---|---|---|---|---|
| Stress | 5.0 (2.2) | 5.6 (2.6) a | 3.7 (2.5) a,b | 6.1 (2.5) a,b,c |
| Anxiety | 2.5 (2.6) | 3.8 (3.0) a | 2.7 (2.6) a,b | 3.7 (3.2) a,c |
| Depression | 2.1 (2.5) | 2.9 (2.9) a | 2.0 (2.5) b | 3.6 (3.1) a,b,c |
| Fatigue | 4.2 (2.6) | 4.3 (2.7) | 3.1 (2.6) a,b | 5.5 (2.7) a,b,c |
| Lonely | 1.7 (2.1) | 3.7 (2.9) a | 2.3 (2.4) a,b | 4.4 (3.2) a,b,c |
| Optimistic | 7.1 (1.9) | 5.9 (2.1) a | 6.7 (1.8) b | 5.4 (2.1) a,b,c |
| Happy | 7.1 (1.8) | 5.8 (2.0) | 7.1 (1.8) | 5.4 (2.0) |
| Academic Functioning | Overall | Bachelor Students | Master Students | PhD Students |
|---|---|---|---|---|
| Quality | 0.0 (2.0) | 0.3 (2.0) | −0.2 (2.0) | −0.9 (1.8) a |
| Time | 0.7 (2.4) * | 0.9 (2.5) * | 0.6 (2.2) | 0.5 (2.5) |
| Grades/Output | 0.4 (2.0) * | 0.8 (2.0) * | 0.1 (2.0) | −0.6 (1.9) a |
| Knowledge | 0.2 (2.3) | 0.3 (2.5) | 0.0 (2.2) | 0.2 (1.7) |
| Reading | 0.4 (2.0) * | 0.3 (2.1) | 0.3 (2.2) | 0.7 (1.2) |
| Writing | 0.4 (1.8) * | 0.6 (1.8) * | 0.2 (1.8) | 0.2 (1.6) |
| Contact with teachers | −2.1 (2.2) * | −2.3 (2.3) * | −2.0 (2.0) * | −1.0 (1.6) *,a,b |
| Interactions with students | −3.0 (2.1) * | −2.9 (2.2) * | −3.3 (1.9) * | −2.6 (1.6) * |
| Balance study-private life | −1.5 (2.5) * | −1.5 (2.6) * | −1.4 (2.5) * | −2.0 (2.4) * |
| Role satisfaction | −0.6 (2.4) * | −0.5 (2.5) | −0.6 (2.2) | −1.0 (2.2) |
| Variable | Stress | Anxiety | Depression | Fatigue | Lonely | Optimistic | Happy |
|---|---|---|---|---|---|---|---|
| Quality | −0.261 * | −0.198 | −0.159 | −0.321 * | −0.114 | 0.188 | 0.210 |
| Time | −0.122 | 0.066 | −0.023 | −0.167 | 0.015 | 0.084 | 0.053 |
| Grades/Output | −0.234 * | −0.096 | −0.070 | −0.252 * | −0.003 | 0.051 | 0.076 |
| Knowledge | −0.079 | −0.035 | −0.004 | −0.197 | −0.099 | 0.137 | 0.083 |
| Reading | −0.051 | −0.111 | −0.025 | −0.043 | −0.063 | 0.094 | 0.089 |
| Writing | −0.019 | 0.040 | −0.035 | −0.078 | −0.116 | 0.131 | 0.105 |
| Contact with teachers | −0.107 | −0.112 | −0.043 | −0.079 | −0.131 | 0.163 | 0.114 |
| Interactions with students | −0.089 | −0.118 | −0.001 | 0.088 | −0.107 | 0.068 | 0.117 |
| Balance study-private life | −0.259 * | −0.358 * | −0.214 | −0.155 | −0.245 * | 0.222 * | 0.257 * |
| Role satisfaction | −0.314 * | −0.291 * | −0.203 | −0.277 * | −0.241 | 0.273 * | 0.272 * |
| Mood | Before COVID-19 | First Lockdown | Summer 2020 | Second Lockdown | ||||
|---|---|---|---|---|---|---|---|---|
| Variable | Men | Women | Men | Women | Men | Women | Men | Women |
| Stress | 4.7 (2.3) | 5.2 (2.1) | 5.0 (2.6) | 5.8 (2.6) a | 3.5 (2.2) b | 3.8 (2.6) a,b | 5.5 (2.6) a,c | 6.3 (2.4) a,b,c |
| Anxiety | 2.1 (2.6) | 2.6 (2.6) | 2.9 (2.8) a | 4.1 (3.0) *,a | 2.2 (2.3) | 2.9 (2.6) b | 2.8 (3.0) | 4.0 (3.2) a,c |
| Depression | 2.1 (2.7) | 2.1 (2.5) | 2.8 (2.9) | 2.9 (2.9) a | 2.0 (2.5) | 1.9 (2.5) b | 3.6 (3.1) a,c | 3.6 (3.1) a,b,c |
| Fatigue | 3.5 (2.7) | 4.4 (2.5) | 3.4 (2.5) | 4.6 (2.7) * | 2.7 (2.2) | 3.3 (2.7) a,b | 4.7 (3.0) a,b,c | 5.8 (2.5) a,b,c |
| Lonely | 1.6 (2.0) | 1.8 (2.1) | 3.4 (2.9) a | 3.8 (2.9) a | 2.1 (2.4) b | 2.3 (2.5) b | 4.3 (3.2) a,c | 4.4 (3.2) a,c |
| Optimistic | 6.9 (2.2) | 7.1 (1.8) | 6.0 (2.2) a | 5.8 (2.1) a | 6.5 (2.1) | 6.8 (1.7) b | 5.4 (2.4) a,c | 5.4 (2.0) a,b,c |
| Happy | 6.6 (2.1) | 7.2 (1.7) | 5.7 (2.0) a | 5.8 (2.0) a | 6.6 (2.2) a | 7.3 (1.6) b | 5.1 (2.2) a,c | 5.5 (1.9) a,c |
| Academic Functioning | Men | Women |
|---|---|---|
| Quality | −0.1 (1.9) | 0.0 (2.0) |
| Time | 0.1 (2.5) | 1.0 (2.3) * |
| Grades/Output | 0.3 (1.9) | 0.4 (2.1) |
| Knowledge | 0.2 (2.3) | 0.2 (2.3) |
| Reading | 0.3 (2.0) | 0.4 (2.0) |
| Writing | 0.2 (2.0) | 0.5 (1.7) * |
| Contact with teachers | −2.0 (2.2) * | −2.0 (2.2) * |
| Interactions with students | −2.9 (2.2) * | −3.0 (2.0) * |
| Balance study-private life | −1.0 (2.8) | −1.7 (2.4) * |
| Role satisfaction | −0.6 (2.3) | −0.6 (2.4) * |
| Variable | Ethnicity | Before COVID-19 | First Lockdown | Summer 2020 | Second Lockdown |
|---|---|---|---|---|---|
| Stress | Dutch | 4.9 (2.1) | 5.3 (2.5) | 3.5 (2.3) a,b | 6.0 (2.4) a,b,c |
| Western | 5.6 (2.0) | 6.4 (2.5) | 4.3 (2.9) b | 6.9 (2.4) a,c | |
| Non-Western | 5.1 (2.5) | 5.9 (3.0) a | 4.0 (2.7) b | 6.0 (2.5) a,c | |
| Anxiety | Dutch | 2.2 (2.5) | 3.3 (2.8) a | 2.3 (2.3) b | 3.1 (2.9) a,c |
| Western | 3.9 (2.6) * | 5.4 (2.9) *,a | 4.2 (2.5) *,b | 6.0 (3.3) *,a,c | |
| Non-Western | 2.6 (2.7) | 4.3 (3.3) a | 3.2 (2.9) b | 4.0 (3.2) †,a | |
| Depression | Dutch | 1.8 (2.5) | 2.4 (2.8) a | 1.8 (2.4) b | 3.1 (3.0) a,b,c |
| Western | 2.5 (2.4) | 3.4 (2.4) | 2.0 (2.3) | 4.6 (3.3) a,c | |
| Non-Western | 2.7 (2.7) * | 3.8 (3.2) *,a | 2.5 (2.8) b | 4.5 (3.1) *,a,c | |
| Fatigue | Dutch | 3.9 (2.5) | 4.0 (2.5) | 2.9 (2.5) a,b | 5.2 (2.6) a,b,c |
| Western | 4.6 (2.6) | 4.7 (2.8) | 3.2 (2.6) | 6.3 (2.6) c | |
| Non-Western | 4.7 (2.7) | 5.1 (3.1) * | 3.9 (2.8) b | 6.2 (2.7) *,a,c | |
| Lonely | Dutch | 1.4 (1.8) | 3.5 (2.8) a | 2.2 (2.3) a,b | 4.1 (3.1) a,c |
| Western | 2.4 (2.2) * | 4.3 (3.1) a | 2.5 (2.8) | 5.5 (3.3) a,c | |
| Non-Western | 2.3 (2.5) * | 4.0 (3.2) a | 2.3 (2.8) b | 4.7 (3.2) a,c | |
| Optimistic | Dutch | 7.4 (1.7) | 6.2 (2.0) a | 6.9 (1.8) b | 5.5 (1.9) a,b,c |
| Western | 6.5 (2.2) | 5.3 (2.0) *,a | 6.5 (1.9) | 4.9 (2.6) a,c | |
| Non-Western | 6.5 (2.2) * | 5.3 (2.4) *,a | 6.4 (1.8) | 5.3 (2.2) a,c | |
| Happy | Dutch | 7.4 (1.6) | 6.2 (1.8) a | 7.3 (1.6) b | 5.7 (1.8) a,b,c |
| Western | 6.4 (2.1) * | 4.9 (1.7) *,a | 6.5 (2.0) b | 4.6 (2.6) a,c | |
| Non-Western | 6.5 (2.1) * | 5.1 (2.2) *,a | 6.8 (2.1) b | 5.0 (2.0) *,a,c |
| Academic Functioning | Dutch | Western Migration Background | Non-Western Migration Background |
|---|---|---|---|
| Quality | 0.0 (1.9) | −0.7 (2.0) | 0.2 (2.3) |
| Time | 0.7 (2.3) * | 1.0 (2.2) | 0.7 (2.8) |
| Grades/Output | 0.4 (1.8) | 0.1 (2.0) | 0.6 (2.6) |
| Knowledge | 0.1 (2.1) | 0.5 (2.0) | 0.3 (2.9) |
| Reading | 0.4 (1.8) | 1.2 (2.2) | 0.0 (2.4) |
| Writing | 0.3 (1.7) | 1.0 (1.6) | 0.3 (2.2) |
| Contact with teachers | −2.2 (2.0) * | −1.0 (2.0) | −1.9 (2.6) * |
| Interactions with students | −3.2 (1.9) * | −2.3 (2.3) * | −2.8 (2.4) * |
| Balance study-private life | −1.6 (2.4) * | −1.6 (3.1) | −1.4 (2.6) * |
| Role satisfaction | −0.6 (2.2) * | −1.0 (2.5) | −0.4 (2.6) |
| Variable | Living Situation | Before COVID-19 | First Lockdown | Summer 2020 | Second Lockdown |
|---|---|---|---|---|---|
| Stress | Alone | 5.1 (2.5) | 5.1 (3.0) | 3.5 (2.8) | 6.3 (2.8) |
| With others | 4.8 (2.1) | 5.2 (2.6) | 3.5 (2.3) | 5.9 (2.6) | |
| With family | 5.3 (2.2) | 6.0 (2.5) | 3.9 (2.6) | 6.2 (2.3) | |
| Anxiety | Alone | 3.4 (3.0) | 4.1 (3.2) | 3.3 (3.0) | 4.2 (3.8) |
| With others | 2.3 (2.5) | 3.4 (2.9) | 2.4 (2.5) | 3.4 (3.0) | |
| With family | 2.4 (2.5) | 4.0 (3.0) | 2.8 (2.5) | 3.8 (3.2) | |
| Depression | Alone | 3.0 (2.7) | 3.4 (3.0) | 2.7 (2.8) | 4.5 (3.4) |
| With others | 1.7 (2.4) * | 2.3 (2.6) | 1.6 (2.4) | 3.4 (3.0) | |
| With family | 2.2 (2.6) | 3.2 (3.1) | 2.1 (2.5) | 3.6 (3.1) | |
| Fatigue | Alone | 4.5 (2.4) | 4.2 (2.8) | 2.9 (2.4) | 5.5 (2.8) |
| With others | 3.9 (2.6) | 3.9 (2.5) | 3.0 (2.5) | 5.6 (2.7) | |
| With family | 4.4 (2.6) | 4.7 (2.8) | 3.3 (2.7) | 5.6 (2.7) | |
| Lonely | Alone | 2.5 (2.5) | 3.8 (3.1) | 2.5 (2.9) | 5.0 (3.5) |
| With others | 1.3 (1.7) | 3.4 (2.7) | 1.8 (2.1) | 4.0 (3.0) | |
| With family | 1.8 (2.2) | 3.9 (3.0) | 2.6 (2.5) | 4.6 (3.2) | |
| Optimistic | Alone | 7.2 (1.8) | 6.3 (2.3) | 7.1 (1.6) | 5.6 (2.3) |
| With others | 7.4 (1.9) | 6.1 (2.1) | 7.0 (1.7) | 5.5 (1.9) | |
| With family | 6.8 (2.0) | 5.6 (2.1) | 6.5 (2.0) | 5.2 (2.2) | |
| Happy | Alone | 7.0 (1.6) | 5.9 (2.0) | 7.2 (2.0) | 5.8 (2.1) |
| With others | 7.4 (1.8) | 6.1 (1.8) | 7.5 (1.5) | 5.5 (1.9) | |
| With family | 6.8 (1.9) † | 5.5 (2.1) | 6.8 (1.9) † | 5.2 (2.0) |
| Academic Functioning | Alone (n = 30) | With Others (n = 99) | With Family (n = 121) |
|---|---|---|---|
| Quality | −0.9 (2.2) | −0.2 (1.7) | 0.4 (2.1) † |
| Time | 0.0 (2.5) | 0.8 (2.2) * | 0.8 (2.5) * |
| Grades/Output | −0.3 (2.3) | 0.2 (1.6) | 0.7 (2.2) * |
| Knowledge | −0.2 (2.5) | 0.1 (1.9) | 0.4 (2.6) |
| Reading | 0.3 (1.9) | 0.5 (1.7) * | 0.2 (2.3) |
| Writing | 0.4 (2.0) | 0.5 (1.4) * | 0.3 (2.0) |
| Contact with teachers | −1.4 (2.5) | −2.0 (2.0) * | −2.1 (2.2) * |
| Interactions with students | −3.3 (1.8) * | −3.0 (1.9) * | −2.9 (2.2) * |
| Balance study-private life | −0.6 (2.9) | −1.8 (2.2) * | −1.6 (2.7) * |
| Role satisfaction | −0.6 (2.7) | −0.8 (1.8) * | −0.4 (2.7) |
| Variable | Before COVID-19 | First Lockdown | Summer 2020 (No Lockdown) | Second Lockdown |
|---|---|---|---|---|
| Perceived immune fitness | 7.5 (1.7) | 7.2 (1.9) | 7.4 (1.7) | 6.9 (1.9) a,b,c |
| Sleep quality | 7.0 (1.8) | 6.8 (2.0) | 7.2 (1.7) b | 6.2 (2.1) a,b,c |
| Being active | 6.2 (2.6) | 4.7 (2.9) a | 5.4 (2.7) a,b | 4.5 (2.8) a,c |
| Quality of life | 7.7 (1.4) | 6.2 (1.9) a | 7.4 (1.5) b | 5.9 (2.0) a,c |
| Variable | ISQ | Perceived Immune Fitness | Sleep Quality | Being Active | Quality of Life |
|---|---|---|---|---|---|
| Stress | 0.025 | −0.119 | −0.302 * | −0.035 | −0.295 * |
| Anxiety | −0.104 | −0.038 | −0.261 * | −0.026 | −0.276 * |
| Depression | −0.024 | −0.225 * | −0.224 * | −0.169 | −0.305 * |
| Fatigue | −0.033 | −0.241 * | −0.406 * | −0.022 | −0.267 * |
| Lonely | −0.139 | −0.213 * | −0.197 * | −0.194 * | −0.291 * |
| Optimistic | 0.047 | 0.132 | 0.187 | 0.076 | 0.459 * |
| Happy | 0.010 | 0.164 | 0.268 * | 0.134 | 0.134 |
| Variable | ISQ | Perceived Immune Fitness | Sleep Quality | Being Active | Quality of Life |
|---|---|---|---|---|---|
| Quality | −0.111 | 0.073 | 0.295 * | −0.052 | 0.219 * |
| Time | −0.088 | 0.007 | 0.108 | −0.060 | 0.107 |
| Grades/Output | −0.154 | 0.060 | 0.127 | −0.068 | 0.108 |
| Knowledge | 0.040 | 0.070 | 0.123 | 0.020 | 0.153 |
| Reading | 0.089 | −0.050 | −0.091 | −0.039 | 0.055 |
| Writing | −0.020 | −0.039 | −0.036 | −0.196 * | 0.076 |
| Contact with teachers | 0.139 | 0.036 | 0.043 | 0.057 | 0.129 |
| Interactions with students | 0.123 | −0.047 | −0.027 | −0.002 | 0.161 |
| Balance study-private life | 0.061 | −0.038 | 0.154 | −0.044 | 0.221 * |
| Role satisfaction | 0.052 | 0.067 | 0.231 * | −0.049 | 0.282 * |
| 95% Confidence Interval for Odds Ratio | ||||
|---|---|---|---|---|
| Model | B | Lower | Odds Ratio | Upper |
| Academic Performance Quality | ||||
| Improvement | ||||
| Constant | 2.42 | |||
| Age | −0.12 * | 0.81 | 0.89 | 0.97 |
| Non-Western ethnicity | −1.50 ** | 0.10 | 0.32 | 0.99 |
| R2 = 0.05 (Cox-Snell) 0.07 (Nagelkerke). Model X2 (3) = 12.7 p = 0.005 | ||||
| Impairment | ||||
| Constant | −1.08 | |||
| Stress | 0.26 ** | 1.08 | 1.29 | 1.54 |
| Fatigue | 0.26 ** | 1.30 | 1.30 | 1.52 |
| R2 = 0.13 (Cox-Snell), 0.18 (Nagelkerke). Model X2 (2) = 34.63, p < 0.001 | ||||
| Study grades/output | ||||
| Increased | ||||
| Constant | 1.69 | |||
| Age | −0.10 * | 0.84 | 0.91 | 0.98 |
| R2 = 0.03 (Cox-Snell), 0.04 (Nagelkerke). Model X2 (1) = 6.92, p = 0.009 | ||||
| Lower | ||||
| Constant | −1.47 | |||
| Stress | 0.24 * | 1.06 | 1.27 | 1.53 |
| Fatigue | 0.22 ** | 1.06 | 1.25 | 1.46 |
| R2 = 0.10(Cox-Snell), 0.15 (Nagelkerke). Model X2 (2) = 25.88, p < 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendriksen, P.A.; Garssen, J.; Bijlsma, E.Y.; Engels, F.; Bruce, G.; Verster, J.C. COVID-19 Lockdown-Related Changes in Mood, Health and Academic Functioning. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1440-1461. https://doi.org/10.3390/ejihpe11040103
Hendriksen PA, Garssen J, Bijlsma EY, Engels F, Bruce G, Verster JC. COVID-19 Lockdown-Related Changes in Mood, Health and Academic Functioning. European Journal of Investigation in Health, Psychology and Education. 2021; 11(4):1440-1461. https://doi.org/10.3390/ejihpe11040103
Chicago/Turabian StyleHendriksen, Pauline A., Johan Garssen, Elisabeth Y. Bijlsma, Ferdi Engels, Gillian Bruce, and Joris C. Verster. 2021. "COVID-19 Lockdown-Related Changes in Mood, Health and Academic Functioning" European Journal of Investigation in Health, Psychology and Education 11, no. 4: 1440-1461. https://doi.org/10.3390/ejihpe11040103
APA StyleHendriksen, P. A., Garssen, J., Bijlsma, E. Y., Engels, F., Bruce, G., & Verster, J. C. (2021). COVID-19 Lockdown-Related Changes in Mood, Health and Academic Functioning. European Journal of Investigation in Health, Psychology and Education, 11(4), 1440-1461. https://doi.org/10.3390/ejihpe11040103