Abstract
Introduction: Patients with burn wounds are more susceptible to develop healthcare associated (HA) infection. Bacterial isolates from HA burn wound infection vary from one place to the other and also differ in terms of antimicrobial susceptibility pattern. The aim of our study was to assess the incidence of HA burn wound infection, risk factors and to determine the microbiological profile and antimicrobial susceptibility pattern of isolated pathogens. Methods: This was a one-year retrospective descriptive study conducted between January 2017 and December 2017, in Al-Babtain Burn and Plastic Surgery center, Kuwait. The identification of bacterial isolates was conducted by conventional biochemical methods according to standard microbiological techniques and commercially available kits using analytical profile index procedure. Results: Total body surface area >35% affected and length of stay more than 14 days were statistically significant risk factors for HA burn infection (RR of 10.057 and 5.912, respectively). Analysis of microbiological profile of these positive cultures indicated that the most common isolated organism was Acinetobacter baumannii followed by Klebsiella pneumoniae. Multidrug resistant organisms composed 65.85% of the positive isolates. Vancomycin, tigecycline, teicoplanin and linezolid showed 100% effectiveness for all Gram positive isolates. For Gram negative organisms, imipenem and meropenem showed 38.71% and 41.93% efficacy, respectively. Conclusion: Identification of antimicrobial susceptibility patterns helps to tailor the required antibiotic policy to minimize the acquired infections among these vulnerable patients.
Introduction
Burn injuries are part of the most common and serious types of trauma, representing a major public health concern all over the world [1]. Hospitalized patients with burn wounds are more vulnerable to infection due to a variety of factors such as the loss of the normal protective skin barrier, impaired immune system and the presence of dead and necrotic tissues that provide an environment conducive to the growth and proliferation of pathogens [2]. About 75% of all deaths after burn injuries are related to infections, with a high rate of healthcare associated infection in burn units [3].
As bacterial isolates from burn patients change with time, it is essential to update the microbiological profile of burn wound infection periodically with identification of the most common isolated pathogens and their antimicrobial sensitivity pattern in order to improve management and outcome [4].
Antibiotic resistance is an emerging concern among patients with healthcare associated infection (HAI) in this era, increasing rapidly and becoming a public health threat; this resistance is in part due to misuse and over use of antibiotic prescription [5]. The emergence of highly drug resistant bacteria in HAI of burn patients, with limited therapeutic options, is an alarming new concern with subsequent morbidity and mortality. Therefore, in depth knowledge of the microbiological profile and antibiotic susceptibility pattern of HAI in patients with burn injuries is essential because many patients with wound infection need to receive antibiotic therapy before availability of the results of microbiological cultures as this is particularly important to reduce morbidity and mortality related to infection [6].
The aim of our study was to assess the incidence of health care associated burn wound infection, risk factors and determination of microbiological profile and antimicrobial susceptibility pattern of isolated pathogens focusing on the distribution of multidrug resistant organisms (MDRO) that can be helpful in the design of empirical antibiotic policy for this category of patient in our setting.
Methods
Study design
This was a one-year prospective study conducted between January 2017 and December 2017, in Al-Babtain Burn and Plastic surgery center, Kuwait.
The study protocol was reviewed and approved by the research committee of the Ministry of Health Kuwait (887/30 Oct 2018).
Study setting
Al-Babtain Burn and Plastic Surgery center is the only referral center for burn patients in Kuwait City, State of Kuwait. Data were retrieved from patients’ medical record and infection control surveillance sheets.
Inclusion criteria
All patients presented with burn injury and requiring admission were included.
Exclusion criteria
Patients with minor burn injury treated on outpatient department basis.
Patients transferred from plastic surgery ward to burn ward and not presenting with burn injury.
Identification of healthcare associated burn wound infection was based on the Centers for Disease Control and Prevention (CDC) criteria for year 2017, which is “a change in burn wound appearance or character, such as rapid eschar separation, or dark brown, black, or violaceous discoloration of the eschar”, with “organism(s) identified from blood by a culture or non-culture based microbiologic testing method which is performed for purposes of clinical diagnosis or treatment” [7].
Microbiological analysis; sample collection and inoculation
Blood cultures were processed using manual standard method (Vitek, Marcy-l’Étoile, France). All blood specimens were put into thioglycolate broth and subcultured after overnight incubation on 5% blood agar, Mac Conkey agar and Chocolate agar plates and incubated overnight at 37 °C aerobically.
The identification of bacterial isolates was conducted by conventional biochemical methods according to standard microbiological techniques and commercially available kits, using the analytical profile index procedure (API; Vitek, bioMérieux, Hazelwood, MO, USA) [8].
Antibiotic susceptibility was determined by using classical Kirby Bauer disc diffusion method on Mueller-Hinton agar according to Clinical and Laboratory Standards Institute (CLSI) guidelines [9]. Interpretation of antimicrobial resistance and susceptibility was determined using CLSI 2015 recommendations [10].
For identification of MDRO we used the definitions outlined by Magiorakos et al. to define multidrug-resistant (MDR) as “acquired non-susceptibility to at least one agent in three or more antimicrobial categories” [11].
Statistical analysis
Different risk factors were assessed to identify the risk of developing healthcare associated burn wound infection. For total body surface area (TBSA) patients were divided according to affected TBSA percentage into two groups: the first group with TBSA% > 35% and the second group with TBSA% ≤ 35%. Regarding the length of hospital stay (LOS), patients were divided into two groups: patients above the mean hospital stay for the studied sample and patients who stayed equally or below the mean calculated length of stay.
Relative risks were calculated to show significance in developing healthcare associated burn wound infection and acquiring multidrug resistant organism. Fischer’s exact test was used to identify significance at p value < 0.05. Statistical analysis was performed using SPSS version 18, (IBM, Chicago, IL, USA).
Results
The study population was composed of 201 patients. Male patients represented 61.19% of the study sample. The flame burn was the most common type of injury among our studied population (62.69%), while scald came second common (27.86%) and all other injuries represented only 9.45% (Table 1).

Table 1.
Distribution of studied risk factors among patients with burn injuries in Al Babtain center during 2017.
For the 201 patients who constituted 2834 patient days, the affected TBSA ranged from 1–98% with a mean of 19.7 ± 17.65%. The average length of hospital stay was 14 days ± 18.14 days, while for patients who developed healthcare associated burn infection the average length of stay was 31 days ± 25.48 days.
During the period of study, 17 patients developed healthcare associated burn wound infection with an incidence rate of 6/1000 patient days. Eleven male patients developed healthcare associated burn wound infection, and six patients were female. This distribution showed no statistical significance (p = 0.756). All patients who developed healthcare associated burn infection had a flame injury, and this was statistically significant (p < 0.001). Patients with burns covering more than 35% of TBSA were found to be statistically more likely to develop healthcare associated burn infection (p < 0.001). Patients who stayed more than the mean LOS of the study (14 days) were more prone to develop healthcare associated infection (p < 0.001). These data are presented in Table 2. Further statistical analysis for the TBSA and LOS by linear regression showed their statistical significance as risk factors to develop healthcare burn associated infection (p < 0.000).
Table 2.
Risk of acquiring healthcare associated burn wound infection in relation to studied risk factors in patients with burn injuries in Al Babtain center during 2017.
The 17 patients who developed healthcare associated burn wound infection revealed 41 positive blood cultures. These were repeated blood cultures collected at different time points for each patient within the infection period. On the other hand, TBSA of burn wound and LOS did not show any statistical significance among patients with healthcare associated burn infection regarding acquisition of multidrug resistant organisms in blood cultures. These data are presented in Table 3.
Table 3.
Risk of acquiring MDROs for patients with healthcare associated burn wound infection in relation to studied risk factors in patients with burn injuries in Al Babtain center during 2017.
Analysis of the microbiological profile of these positive cultures indicated that the most commonly isolated organism was Acinetobacter baumannii 17 (41.46%) followed by eight Klebsiella pneumoniae (19.51%). Multidrug resistant organisms composed 27 (65.85%) of the positive isolates. All Acinetobacter baumannii isolates were MDR (100%). These data are shown in Table 4.
Table 4.
Microbiological profile and distribution of MDRO among patients with healthcare associated burn infection in Al Babtain center in 2017.
Regarding the antimicrobial sensitivity pattern among Gram positive organisms we found that (66.67%) of the isolates of Staphylococcus aureus were MRSA and that both Enterococcus gallinarum and Enterococcus faecalis were sensitive to penicillins. Vancomycin, tigecycline, teicoplanin and linezolid showed 100% susceptibility in all Gram positive isolates. This is presented in Figure 1.
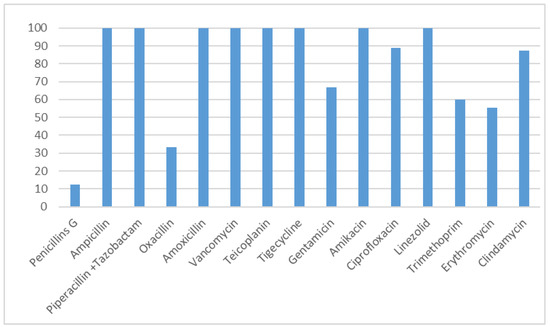
Figure 1.
Antimicrobial susceptibility pattern for Gram positive isolates in patients with healthcare associated burn wound infections in Al Babtain center during 2017.
For Gram negative organisms, tigecycline was 100% active on tested isolates, while imipenem and meropenem were active on 38.71% and 41.93% of the isolates, respectively. In our study we found one isolate (Acinetobacter baumannii) which showed resistance to colistin. This is shown in Figure 2.
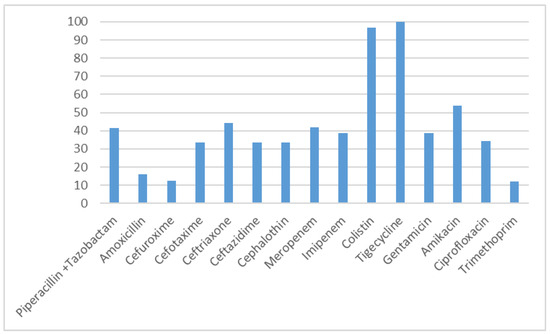
Figure 2.
Antimicrobial susceptibility pattern for Gram negative isolates in patients with healthcare associated burn infections in Al Babtain center during 2017.
Discussion
Healthcare associated infections represent a serious issue for health services all over the world, impacting the survival of high-risk patients, such as burn patients. Burn site infections can influence both the survival of the patient and the outcome of reconstructive treatment [12].
In our study, we revealed that the incidence rate of healthcare associated burn infection was 6/1000 patient days. This rate is higher than that of the study of Van Duin and his colleagues who identified a rate of 1.78/1000 patient days [13].
However, another comprehensive study of the epidemiology of burn infection showed that the rate among patients with TBSA > 30% exceeds 5/1000 patient days [14]. It is worth to mention that our setting is the only referral center for burn patients in the state of Kuwait, so any age group or degree of burn, type of burn injury or TBSA will be receiving management in our setting.
Our findings showed that flame burn is the most common (62.69%) cause of burn injury. This is similar to a systematic review of epidemiology of burn injuries in the east Mediterranean Region and reports from India and Nepal [15,16,17]. Several factors may contribute to the predominance of flame burn injury. Diverse intentions for flame injuries have been reported, marital problems, family problems, psychological and psychiatric disorders as well as poverty. Low socioeconomic status with poorly secured liquefied petroleum gas cylinders, or cooking equipment, or using open fire for cooking are usually implicated in flame burn injuries [15,16,17].
A total body surface area affected above 35% was shown to be a significant risk factor for developing healthcare associated burn infection in our study. This is similar to different studies conducted in the USA, Turkey and Egypt, which showed that a TBSA above 30% is an independent risk factor for burn wound infection [14,18,19]. Increase in TBSA is usually associated with loss of natural physical defense, decrease in patient immune system, and these patients are usually in need of invasive devices. All these factors will lead to an increased risk of HAIs.
Patients who spend more time in the hospital are more vulnerable to develop HAIs. Our patients spent an average of 14 days in the hospital, this in accordance with an Iranian study and a systematic review of different countries in the eastern Mediterranean Region that showed similar duration of hospital stay [15,20]. Van Duin and his colleagues reported that half of the patients who spend 80 days from admission will experience at least one HAI [13]. Also Coetzee et al. reported that the risk of wound infection increases by time [21]. Burn wounds are known to be good media for bacterial growth, and colonization occurs shortly after the injury as virulent microorganism strains invade the skin and soft tissue; as the host defense is weak, an increase in the number of microorganisms will be able to reach the venous system to cause infection [22].
In the current study, the most commonly isolated microorganisms from healthcare associated burn wound infection were Acinetobacter baumannii (41.46%) followed by Klebsiella pneumoniae (19.51%) then Staphylococcus aureus and Pseudomonas aeruginosa (14.63% each). This result is in agreement with a Turkish study which revealed Acinetobacter baumannii as the most common pathogen isolated (23.6%); in the same study the percentage of S. aureus was near to our value (11.2%) [23].
The microbiological profile in our study is somewhat different from that shown in a related study done by Rathod et al., which showed Pseudomonas aeruginosa as the most frequent isolate (34.93%) [24].
Possible explanations to the difference in the microbiological profile may be due to differences in geographic location or patient age (children and adults), differences in hygienic measures applied in healthcare facilities and associated cross-infection by the hands of healthcare personnel.
In the current study, we found that MDROs represented 65.85% of the positive cultures; 100% of Acinetobacter baumannii strains were resistant, resistance in S. aureus strains was 66.67%, while for Klebsiella pneumoniae and Pseudomonas aeruginosa the percentage of resistant strains was 50% and 11.11%, respectively. These findings are in agreement with a related Egyptian study conducted in 2016 which showed that multidrug resistant Gram negative organisms represented about 60% of the isolates [25].
Regarding the antibiotic sensitivity pattern of the isolates from healthcare associated burn infections, Gram positive organisms were 100% sensitive to vancomycin, teicoplanin, tigecycline and linezolid 100% effectiveness, and to a lower extent to other antimicrobials such as clindamycin (88%) and gentamicin (66%). Similar results are shown in the study of Rathod et al. that revealed 100% sensitivity to vancomycin and linezolid followed by clindamycin (64.55%) [24].
In our study, sensitivity to imipenem was only 38.71% in Gram negative isolates; this may be explained by overuse of imipenem in our setting to improve the clinical outcome of such critically ill patients. This result is similar to that found by Mohammed in which sensitivity to imipenem was 35% [25]. In another study by Rathod VS et al., in which Pseudomonas aeruginosa was the most common isolate, the organism showed 75% resistance to ceftazidime [24].
Lack of compliance to the infection control measures, absence of an antimicrobial stewardship program, and patients’ characteristics, especially for this vulnerable category, all can lead to emergence of resistant microorganisms.
Among study limitations, the absence of an electronic file system has limited the collection of other potential risk factors such as degree of burn, time of injury and different source of flame burn. Also, the establishment of the MDRO profile depended on the disc diffusion method not on PCR for detection of resistance genes due to unavailability of these resources in the hospital lab.
Conclusion
Identification of the microbiological profile of HAI in burn wounds is of great importance both epidemiologically and to improve the clinical outcome, as this data may guide effective empirical antibiotic therapy. In our setting the most prevalent microorganism identified was Acinetobacter baumannii and all its isolates were found to be MDR. Proper compliance with infection control measures and development of an antibiotic stewardship program will help in reducing the number of infections and the emergence of resistant strains for the critically ill patient with burn wound injury.
Author Contributions
MA, EE, MAMR performed the literature review. MAMR designed the study, collected the data and performed the statistical analysis. EE and MAMR performed the data interpretation. All authors prepared the first draft, read and approved the final version of the manuscript.
Funding
None to declare.
Conflicts of Interest
All authors—none to declare.
References
- Mock, C.; Peck, M.; Peden, M.; et al. A WHO Plan for Burn Prevention and Care; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Bhat, V.G.; Vasaikar, S.D. Bacteriological profile and antibiogram of aerobic burn wound isolates in Mthatha, Eastern Cape, South Africa. South Afr J Epidemiol Infect 2010, 25, 16–19. [Google Scholar] [CrossRef]
- Fouzia, B.; Damle, A.S.; Maher, G. Changing patterns of burn infections IOSR. J Dent Med Sci 2013, 5, 11–14. [Google Scholar]
- Kumarasamy, K.K.; Toleman, M.A.; Walsh, T.R.; et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: A molecular, biological, and epidemiological study. Lancet Infect Dis 2010, 10, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Lushniak, B.D. Antibiotic resistance: A public health crisis. Public Health Rep 2014, 129, 314–316. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Vartak, A.M.; Patil, A.; Saldanha, J. Bacteriology of the burn wound at the Bai Jerbai Wadia Hospital for children, Mumbai, India—A 13 year study, Part I-Bacteriological profile. Indian J Plast Surg 2009, 42, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC/NHSN Surveillance Definitions for Specific Types of Infections. Available online: https://www.cdc.gov/nhsn/PDFs/pscManual/17pscNos InfDef_current.pdf (accessed on 12 August 2018).
- Immunochemical methods used for organism detection. In AS Bailey & Scott’s Diagnostic Microbiology, 12th ed.; Forbes, B.A., Sham, D.F., Weissfeld, A.S., Eds.; Mosby: St. Louis, MO, USA, 2007; pp. 147–158. [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Disk Susceptibility Tests. Approved Standard—Twelfth Edition. CLSI Document M02-A12. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. Twenty-Fifth Informational Supplement. CLSI Document M100-S25. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, S.E. The relationship between antimicrobial resistance and patient outcomes: Mortality, length of hospital stay, and health care costs. Clin Infect Dis 2006, 42 (Suppl. 2), S82–S89. [Google Scholar] [CrossRef] [PubMed]
- van Duin, D.; Strassle, P.D.; DiBiase, L.M.; et al. Timeline of healthcare-associated infections and pathogens after burn injuries. Am J Infect Control 2016, 44, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.; McManus, A.; Nursing Committee of the International Society for Burn Injuries. Infection control in burn patients. Burns 2004, 30, A16–A24. [Google Scholar] [CrossRef] [PubMed]
- Othman, N.; Kendrick, D. Epidemiology of burn injuries in the East Mediterranean Region: A systematic review. BMC Public Health 2010, 10, 83. [Google Scholar] [CrossRef] [PubMed]
- Maske, A.N.; Deshmukh, S.N. Clinico-epidemiological study of burns: Our experience with 500 patients. Int Surg J 2016, 3, 1234–1239. [Google Scholar] [CrossRef]
- Tripathee, S.; Basnet, S.J. Epidemiology of burn injuries in Nepal: A systemic review. Burns Trauma 2017, 5, 10. [Google Scholar] [PubMed]
- Güldoğan, C.E.; Kendirci, M.; Tikici, D.; Gündoğdu, E.; Yasti. Clinical infection in burn patients and its consequences. Ulus Travma Acil Cerrahi Derg 2017, 23, 466–471. [Google Scholar] [PubMed]
- El-Maghawry, H.A.M.M.; El Nem, W.; Sherif, N.; Hagag, S.A. An interventional study to decrease healthcare associated burn wound infections in the burn unit of Al Ahrar Hospital in Zagazig city, Sharkia Governorate. Int J Curr Microbiol Appp Sci 2016, 5, 566–578. [Google Scholar] [CrossRef][Green Version]
- Emami, S.A.; Karimi, H.; Alijanpour, A. Epidemiology of burn wound infection and its bacterial resistance, burn registry program. Merit Res J Med Med Sci 2015, 3, 135–139. [Google Scholar]
- Coetzee, E.; Rode, H.; Kahn, D. Pseudomonas aeruginosa burn wound infection in a dedicated paediatric burns unit. S Afr J Surg 2013, 51, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Essayagh, M.; Essayagh, T.; Essayagh, S.; El Hamzaoui, S. Epidemiology of burn wound infection in Rabat, Morocco: Three-year review. Med Sante Trop 2014, 24, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Bayram, Y.; Parlak, M.; Aypak, C.; Bayram, I. Three-year review of bacteriological profile and antibiogram of burn wound isolates in Van, Turkey. Int J Med Sci 2013, 10, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Rathod, V.S.; Kasturi, R.S. Emergence of multi-drug resistant strains among bacterial isolates in burn wound swabs in a tertiary care centre, Nanded, Maharashtra, India. Int J Res Med Sci 2017, 5, 973–977. [Google Scholar] [CrossRef]
- Mohamed, H. One year prevalence of critically ill burn wound bacterial infections in surgical ICU in Egypt: Retrospective study. Egypt J Anesth 2016, 32, 431–434. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).