
Clinical Evaluation of Reduced-Thickness Monolithic Lithium-Disilicate Crowns: One-Year Follow-Up Results

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aquilino, S.A.; Caplan, D.J. Relationship between crown placement and the survival of endodontically treated teeth. J. Prosthet. Dent. 2002, 87, 256–263. [Google Scholar] [CrossRef]
- Dammaschke, T.; Steven, D.; Kaup, M.; Ott, K.H.R. Long-term survival of root-canal-treated teeth: A retrospective study over 10 years. J. Endod. 2003, 29, 638–643. [Google Scholar] [CrossRef]
- Sorensen, J.A.; Martinoff, J.T. Intracoronal reinforcement and coronal coverage: A study of endodontically treated teeth. J. Prosthet. Dent. 1984, 5, 780–784. [Google Scholar] [CrossRef]
- Eckerbom, M.; Magnusson, T.; Martinsson, T. Reasons for and incidence of tooth mortality in a Swedish population. Endod. Dent. Traumatol. 1992, 8, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Torbjörner, A.; Fransson, B. Biomechanical aspects of prosthetic treatment of structurally compromised teeth. Int. J. Prosthodont. 2004, 17, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Fokkinga, W.A.; Kreulen, C.M.; Bronkhorst, E.; Creugers, N.H. Up to 17-year controlled clinical study on post-and-cores and covering crowns. J. Dent. 2007, 35, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Etman, M.K.; Woolford, M.J. Three-year clinical evaluation of two ceramic crown systems: A preliminary study. J. Prosthet. Dent. 2010, 103, 80–90. [Google Scholar] [CrossRef]
- Tysowsky, G.W. The science behind lithium disilicate: A metal-free alternative. Dent. Today 2009, 28, 112–113. [Google Scholar] [PubMed]
- Reich, S.; Schierz, O. Chair-side generated posterior lithium disilicate crowns after 4 years. Clin. Oral Investig. 2013, 17, 1765–1772. [Google Scholar] [CrossRef]
- Giordano, R. Materials for chairside CAD/CAM-produced restorations. J. Am. Dent. Assoc. 2006, 137, 14–21. [Google Scholar] [CrossRef]
- Guess, P.C.; Zavanelli, R.A.; Silva, N.R.; Bonfante, E.A.; Coelho, P.G.; Thompson, V.P. Monolithic CAD/CAM lithium disilicate versus veneered Y-TZP crowns: Comparison of failure modes and reliability after fatigue. Int. J. Prosthodont. 2010, 23, 434–442. [Google Scholar] [PubMed]
- Zhao, K.; Pan, Y.; Guess, P.C.; Zhang, X.-P.; Swain, M.V. Influence of veneer application on fracture behavior of lithium-disilicate-based ceramic crowns. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2012, 28, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.; Bonfante, E.; Martins, L.; Valverde, G.; Thompson, V.; Ferencz, J.; Coelho, P. Reliability of reduced-thickness and thinly veneered lithium disilicate crowns. J. Dent. Res. 2012, 91, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Fasbinder, D.J.; Dennison, J.B.; Heys, D.; Neiva, G. A clinical evaluation of chairside lithium disilicate CAD/CAM crowns: A two-year report. J. Am. Dent. Assoc. Sup. 2010, 141, 10–14. [Google Scholar] [CrossRef]
- Reich, S.; Fischer, S.; Sobotta, B.; Klapper, H.U.; Gozdowski, S. A preliminary study on the short-term efficacy of chairside computer-aided design/computer-assisted manufacturing-generated posterior lithium disilicate crowns. Int. J. Prosthodont. 2010, 23, 214–216. [Google Scholar]
- Etemadi, S.; Smales, R.J.; Drummond, P.W.; Goodhart, J.R. Assessment of tooth preparation designs for posterior resin-bonded porcelain restorations. J. Oral Rehabil. 1999, 26, 691–697. [Google Scholar] [CrossRef]
- Blair, F.M.; Wassell, R.W.; Steele, J.G. Crowns and other extra-coronal restorations: Preparations for full veneer crowns. Br. Dent. J. 2002, 192, 567–571. [Google Scholar] [CrossRef]
- Shillingburg, H.T.; Hobo, S.; Whitsett, L.D.; Jacobi, R.; Brackett, S.E. Fundamentals of Fixed Prosthodontics, 3rd ed.; Carol Stream; Quintessence Publishing Co., Inc.: Carol Stream, IL, USA, 1997. [Google Scholar]
- Davis, G.R.; Tayeb, R.A.; Seymour, K.G.; Cherukara, G.P. Quantification of residual dentine thickness following crown preparation. J. Dent. 2012, 40, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Bayne, S.; Schmalz, G. Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin. Oral Investig. 2005, 9, 209–214. [Google Scholar] [CrossRef]
- Krämer, N.; Ebert, J.; Petschelt, A.; Frankenberger, R. Ceramic inlays bonded with two adhesives after 4 years. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2006, 22, 13–21. [Google Scholar] [CrossRef]
- Seydler, B.; Rues, S.; Müller, D.; Schmitter, M. In vitro fracture load of monolithic lithium disilicate ceramic molar crowns with different wall thicknesses. Clin. Oral Investig. 2014, 18, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Nawafleh, N.A.; Hatamleh, M.M.; Öchsner, A.; Mack, F. Fracture load and survival of anatomically representative monolithic lithium disilicate crowns with reduced tooth preparation and ceramic thickness. J. Adv. Prosthodont. 2017, 9, 416–422. [Google Scholar] [CrossRef] [Green Version]
- Sasse, M.; Krummel, A.; Klosa, K.; Kern, M. Influence of restoration thickness and dental bonding surface on the fracture resistance of full-coverage occlusal veneers made from lithium disilicate ceramic. Dent. Mater. 2015, 31, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Reinhardt, M.; Peschke, A. Fatigue resistance of CAD/CAM all-ceramic molar crowns of reduced thickness. Dent. Mater. 2017, 33, e38. [Google Scholar] [CrossRef]
- Sulaiman, T.A.; Delgado, A.J.; Donovan, T.E. Survival rate of lithium disilicate restorations at 4 years: A retrospective study. J. Prosthet. Dent. 2015, 114, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Malament, K.A.; Natto, Z.S.; Thompson, V.; Rekow, D.; Eckert, S.; Weber, H.P. Ten-year survival of pressed, acid-etched e.max lithium disilicate monolithic and bilayered complete-coverage restorations: Performance and outcomes as a function of tooth position and age. J. Prosthet. Dent. 2019, 121, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Longhini, D.; Rocha, C.; de Oliveira, L.T.; Olenscki, N.G.; Bonfante, E.A.; Adabo, G.L. Mechanical behavior of ceramic monolithic systems with different thicknesses. Oper. Dent. 2019, 44, E244–E253. [Google Scholar] [CrossRef]
- de Paula, V.G.; Bonfante, G.; Lorenzoni, F.C.; Coelho, P.G.; Bonjardim, L.R.; Fardin, V.P.; Bonfante, E.A. Lifetime prediction of veneered versus monolithic lithium disilicate crowns loaded on marginal ridges. Dent. Mater. 2019, 35, 511–522. [Google Scholar] [CrossRef]
- Gehrt, M.A.; Wolfart, S.; Rafai, N.; Reich, S.M.; Edelhoff, D. Clinical results of lithium-disilicate crowns after up to 9 years of service. Clin. Oral Investig. 2013, 17, 275–284. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Group | P | |||||
|---|---|---|---|---|---|---|
| Monolithic N = 22 | Layered N = 22 | |||||
| N | % | N | % | |||
| Ceramic fracture | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Marginal adaptation | A | 21 | 95.5% | 22 | 100.0% | 1.000 |
| B | 1 | 4.5% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Color | A | 11 | 50.0% | 22 | 100.0% | <0.001 |
| B | 11 | 50.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Caries | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Marginal discoloration | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Occlusal contact | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Approximal contact | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Retention | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Postoperative sensitivity | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Ceramic fracture | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Marginal adaptation | A | 21 | 95.5% | 22 | 100.0% | 1.000 |
| B | 1 | 4.5% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Color | A | 11 | 50.0% | 22 | 100.0% | <0.001 |
| B | 11 | 50.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Caries | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Marginal discoloration | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Occlusal contact | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Approximal contact | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Retention | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Postoperative sensitivity | A | 22 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Group | P | |||||
|---|---|---|---|---|---|---|
| Monolithic N = 22 * | Layered N = 22 | |||||
| N | % | N | % | |||
| Ceramic fracture | A | 21 | 95.5% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 1 | 4.5% | 0 | 0.0% | ||
| Marginal adaptation | A | 18 | 81.8% | 22 | 100.0% | 0.108 |
| B | 3 | 13.6% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 1 | 4.5% | 0 | 0.0% | ||
| Color | A | 11 | 52.4% | 22 | 100.0% | <0.001 |
| B | 10 | 47.6% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Caries | A | 21 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Marginal discoloration | A | 16 | 76.2% | 22 | 100.0% | 0.021 |
| B | 5 | 23.8% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Occlusal contact | A | 21 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Approximal contact | A | 21 | 100.0% | 20 | 90.9% | 0.488 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 2 | 9.1% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Retention | A | 21 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Postoperative sensitivity | A | 21 | 100.0% | 22 | 100.0% | 1.000 |
| B | 0 | 0.0% | 0 | 0.0% | ||
| C | 0 | 0.0% | 0 | 0.0% | ||
| D | 0 | 0.0% | 0 | 0.0% | ||
| Group | N | Minimum | Maximum | Percentiles | P | |||
|---|---|---|---|---|---|---|---|---|
| 25th | 50th (Median) | 75th | ||||||
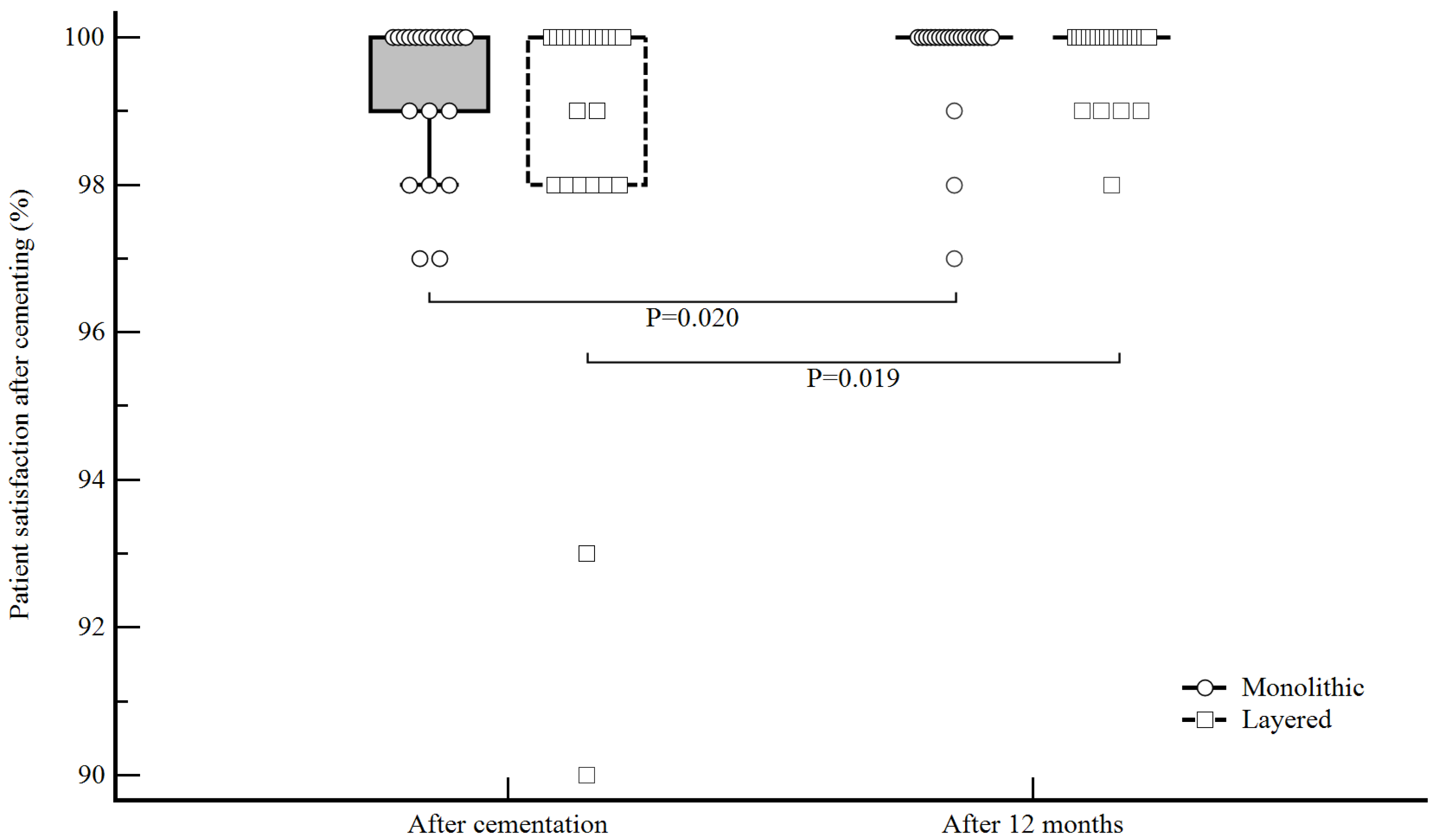
| Patient satisfaction after cementing | Monolithic | 22 | 97.00 | 100.00 | 98.75 | 100.00 | 100.00 | 0.458 |
| Layered | 22 | 90.00 | 100.00 | 98.00 | 100.00 | 100.00 | ||
| Patient satisfaction after 12 months | Monolithic | 22 | 97.00 | 100.00 | 100.00 | 100.00 | 100.00 | 0.578 |
| Layered | 22 | 98.00 | 100.00 | 99.75 | 100.00 | 100.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Špehar, D.; Jakovac, M. Clinical Evaluation of Reduced-Thickness Monolithic Lithium-Disilicate Crowns: One-Year Follow-Up Results. Processes 2021, 9, 2119. https://doi.org/10.3390/pr9122119
Špehar D, Jakovac M. Clinical Evaluation of Reduced-Thickness Monolithic Lithium-Disilicate Crowns: One-Year Follow-Up Results. Processes. 2021; 9(12):2119. https://doi.org/10.3390/pr9122119
Chicago/Turabian StyleŠpehar, Davor, and Marko Jakovac. 2021. "Clinical Evaluation of Reduced-Thickness Monolithic Lithium-Disilicate Crowns: One-Year Follow-Up Results" Processes 9, no. 12: 2119. https://doi.org/10.3390/pr9122119
APA StyleŠpehar, D., & Jakovac, M. (2021). Clinical Evaluation of Reduced-Thickness Monolithic Lithium-Disilicate Crowns: One-Year Follow-Up Results. Processes, 9(12), 2119. https://doi.org/10.3390/pr9122119