
Number of Convolution Layers and Convolution Kernel Determination and Validation for Multilayer Convolutional Neural Network: Case Study in Breast Lesion Screening of Mammographic Images


 ,
, 

Abstract
1. Introduction
2. Methodology
2.1. Collection of Mammography Images
2.2. MCNN-Based Classifier Design
- ROI feature map extraction: a 100 pixels (width) × 100 pixels (height) bounding box was used to extract feature map in the ROI; a 100 (width) × 100 (height) pixel bounding box was used to extract the feature map in the suspicious lesion area on the left or right breast. After ROI extraction, the feature maps were fed into multiconvolutional pooling layers for the feature extraction process.
- Multiconvolutional pooling processing: The multiconvolutional pooling layers were used to detect the shape, borders, or corners of the input feature map via 2D spatial convolutional processes and process sharpening and noise removal [21,22,23], followed by maximum pooling (MP) to reduce the feature map dimensions. For each convolutional pooling process, one convolutional process and one pooling process were used to perform feature extraction. Hence, for each feature extraction, 16 different weighted kernel windows were used to produce 16 feature maps, and 16 MP processes were performed to reduce the dimensions of the feature maps.
- Determination of the size of kernel convolution windows: In literature [35,36], a 3 × 3 kernel convolution window was used to replace high-dimensional kernel convolution windows, such as those with window sizes 5 × 5, 7 × 7, 9 × 9, 11 × 11; the high-dimensional convolution kernel had a wide feature search range; however, its process resulted in specific feature omission and increased computation and complexity. Through experimental results, the convolutional process with a 3 × 3 kernel window can retain the same performance for feature extraction using a 5 × 5 kernel window. Although the computational volume of a 3 × 3 window was higher than those of a 5 × 5 window, the 3 × 3 kernel window required fewer window parameters than the 5 × 5 window. Continuous multi 3 × 3 convolution kernel processes showed the rapid enhancement and extraction of the desired object from low-level features (extraction of an object’s edge) to high-level information (extraction of an object’s shape) in the detection of nonlinear features, and such a result can increase the nonlinearity feature representation [27,36]. Hence, this study used a complete 3 × 3 kernel window for feature extraction and determined the number of kernel windows in each convolutional layer.
- Classification layer design: we established a fully connected backpropagation neural network (BPNN), including an input layer, two hidden layers, and an output layer that used the loss functions, such as cross-entropy or binary cross-entropy (BCE) function, to evaluate the classifier’s performance [35,36,37,38]. The BPNN’s parameters were adjusted using an optimization algorithm, such as the adaptive moment estimation method (ADAM) algorithm [39,40], and employed the loss function to minimize the residual value between the desired and predicted values because the error rate was as low as possible. The BCE loss function was selected for this study and depicted as follows [35,36,39,40]:
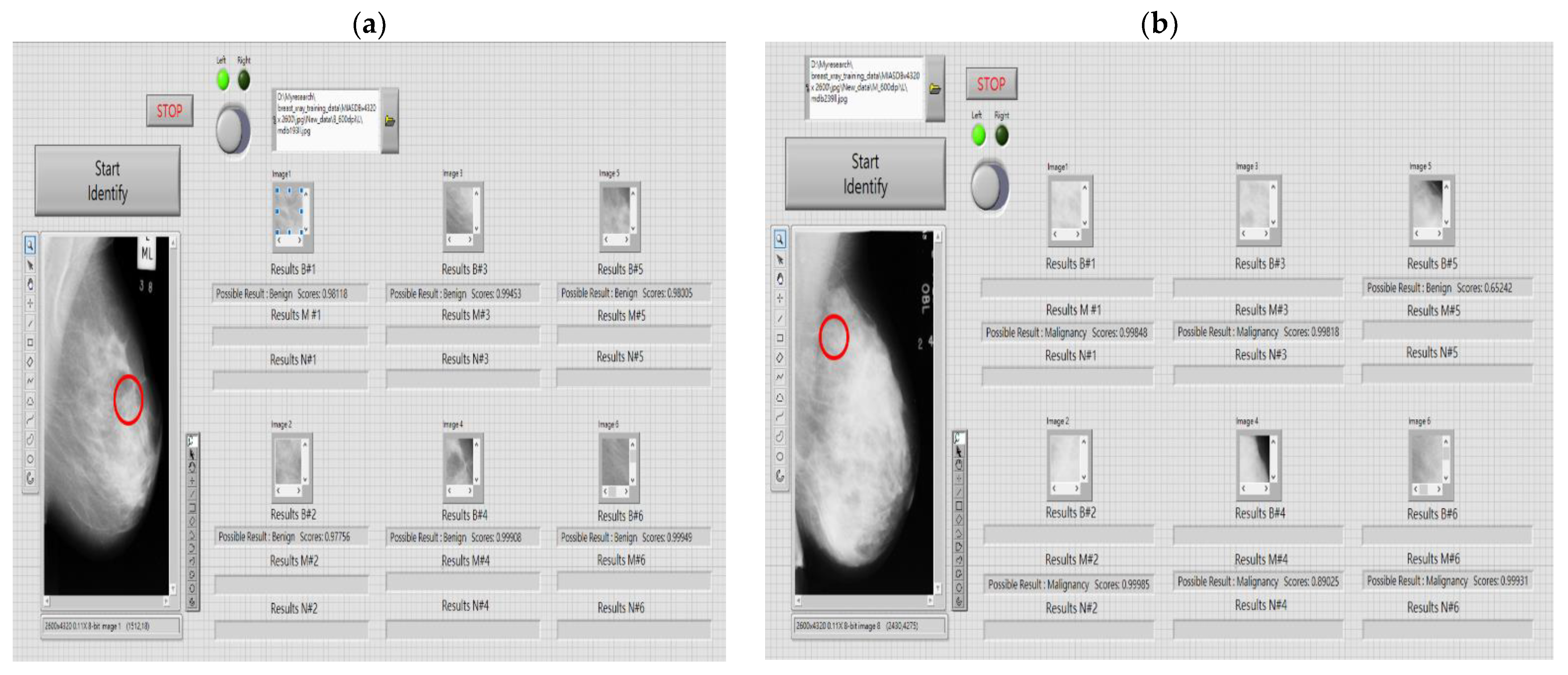
2.3. Human–Machine Interface Design for Breast Lesion Screening
- (1)
- ROI extraction function (manual or automatic modes): The path of mammography images can be set and images can be easily imported into the human–machine interface. In automatic screening mode, the most frequent region of breast tumors (based on the high distribution probability on right and left breasts) and the specific bounding box with 100 × 100 pixel dimension were used to automatically extract the feature maps (at least six maps) and save them in a designated file based on the screenshot sequence in automatic mode, or the clinician and radiologist can manually extract the feature maps. After the selection of the feature maps, they were saved in the designated file according to the sequence in manual mode.
- (2)
- Feature enhancement, noise removal, and feature extraction: three convolutional pooling layers (default structure) were used for digital image preprocessing and feature extraction.
- (3)
- Determination of kernel convolution window size and number: The size of kernel windows was set to 3 × 3 (default), the number of kernel windows to 16, and the size of MP window to 2 × 2. After the convolution processes in each convolutional layer, the same number of MP processes were performed. The size and number of kernel convolution windows can be set by the users (clinicians and radiologists).
- (4)
- Pattern recognition function: the open-source TensorFlow platform [41] was used to carry out an MCNN-based classification with a suitable number of convolution layers and kernel windows.
3. Experimental Results
- The suitable classifier structure consisted of three convolutional pooling layers and a fully connected BPNN was suggested to establish the multilayer classifier model;
- The size of the kernel convolution window could be set to 3 × 3 for convolutional operations;
- The better capacity of feature extraction could be achieved by using 16 kernel convolution windows and 16 MP winds for each convolutional pooling layer, which could increase the classifier’s recognition capability.
4. Discussion
- these processes were continuously to perform the end-to-end noise filtering and feature extraction tasks, which could extract the high-level spatial information, such as the possible lesion’s contour and shape, to detect nonlinear features representation and increase the classification accuracy;
- reducing the number of convolution layers and convolution kernel and pooling processes could reduce the dimension of feature parameters and also reduce the computational complexity and computational time;
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MCNN | Multilayer Convolutional Neural Network |
| CNN | Convolutional Neural Network |
| MPN | Multilayer Perceptron Network |
| 2D | Two-Dimension |
| 1D | One-Dimension |
| ML | Machine Learning |
| DL | Deep Learning |
| MIAS | Mammographic Image Analysis Society |
| BI-RADS | Breast Imaging-Reporting and Data System |
| ROI | Region of Interest |
| Nor | Normal |
| B | Benign |
| M | Malignant |
| CAD | Computer-Aided Diagnosis |
| TP | True Positive |
| FP | False Positive |
| TN | True Negative |
| FN | False Negative |
| AI | Artificial Intelligence |
| MP | Maximum Pooling |
| BPNN | Backpropagation Neural Network |
| BCE | Binary Cross-Entropy |
| ADAM | Adaptive Moment Estimation Method |
| GPU | Graphics Processing Unit |
| PPV | Positive Predictive Value |
| DDSM | Digital Database of Screening Mammography |
| CBIS-DDSM | Curated Breast Imaging Subset of Digital Database for Screening Mammography-DDSM |
| DNN | Deep Neural Network |
| Grad-CAM | Gradient-Weighted Class Activation Mapping |
| ASR | Automatic Speech Recognition |
| ADR | Automatic Depression Recognition |
| MIT-BIH | Massachusetts Institute of Technology-Beth Israel Hospital Arrhythmia Laboratory |
| DNN-HMM | Deep Neural Network Hidden Markov Model |
| RMSE | Root Mean Square Error |
| MAE | Mean Absolute Error |
References
- World Cancer Day 2021: Spotlight on IARC Research Related to Breast Cancer. 2021. Available online: https://www.iarc.who.int/featured-news/world-cancer-day-2021/ (accessed on 12 July 2022).
- Ministry Health and Welfare, Taiwan, 2020 Cause of Death Statistics. 2021. Available online: https://dep.mohw.gov.tw/dos/lp-1800-113.html (accessed on 12 July 2022).
- IARC Working Group on the Evaluation of Cancer-Preventive Interventions, Breast Cancer Screening. In IARC Handbooks of Cancer Prevention; International Agency for Research on Cancer: Lyon, France, 2016; Volume 15.
- Tsai, K.-J.; Chou, M.-C.; Li, H.-M.; Liu, S.-T.; Hsu, J.-H.; Yeh, W.-C.; Hung, C.-M.; Yeh, C.-Y.; Hwang, S.-H. A high-performance deep neural network model for BI-RADS classification of screening mammography. Sensors 2022, 22, 1160. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.A.; Comstock, C.E.; Lee, C.H. ACR BIRADS® magnetic resonance imaging. In ACR BI-RADS® Atlas, BREAST Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Sickles, E.; d’Orsi, C.; Bassett, L.; Appleton, C.; Berg, W.; Burnside, E.; Feig, S.; Gavenonis, S.; Newell, M.; Trinh, M. Acr bi-rads® mammogramphy. ACR BI-RADS® Atlas Breast Imaging Report. Data Syst. 2013, 5, 2013. [Google Scholar]
- Breast Imaging-Reporting and Data System (BI-RADS). Available online: https://radiopaedia.org/articles/breast-imagingreporting-and-data-sytem-bi-rads (accessed on 20 July 2021).
- Halkiotis, S.; Botsis, T.; Rangoussi, M. Automatic detection of clustered microcalcifications in digital mammograms using mathematical morphology and neural networks. Signal Process. 2007, 87, 1559–1568. [Google Scholar] [CrossRef]
- Mahersia, H.; Boulehmi, H.; Hamrouni, K. Development of intelligent systems based on Bayesian regularization network and neuro-fuzzy models for mass detection in mammograms: A comparative analysis. Comput. Methods Programs Biomed. 2016, 126, 46–62. [Google Scholar] [CrossRef]
- Vijayarajeswari, R.; Parthasarathy, P.; Vivekanandan, S.; Basha, A.A. Classification of mammogram for early detection of breast cancer using SVM classifier and Hough transform. Measurement 2019, 146, 800–805. [Google Scholar] [CrossRef]
- He, L.; Niu, M.; Tiwari, P.; Marttinen, P.; Su, R.; Jiang, J.; Guo, C.; Wang, H.; Ding, S.; Wang, Z.; et al. Deep learning for depression recognition with audiovisual cues: A review. Inf. Fusion 2022, 80, 56–86. [Google Scholar] [CrossRef]
- Sathyan, A.; Martis, D.; Cohen, K. Mass and calcification detection from digital mammogramsusing UNets. In Proceedings of the 2020 7th IEEE International Conference on Soft Computing & Machine Intelligence (ISCMI), Stockholm, Sweden, 14–15 November 2020; pp. 229–232. [Google Scholar]
- Agarwal, R.; Díaz, O.; Yap, M.H.; Lladó, X.; Martí, R. Deep learning for mass detection in full field digital mammograms. Comput. Biol. Med. 2020, 121, 103774. [Google Scholar] [CrossRef]
- Xu, S.; Adeli, E.; Cheng, J.Z.; Xiang, L.; Li, Y.; Lee, S.W.; Shen, D. Mammographic mass segmentation using multichannel and multiscale fully convolutional networks. Int. J. Imaging Syst. Technol. 2020, 30, 1095–1107. [Google Scholar] [CrossRef]
- Shelhamer, E.; Long, J.; Darrell, T. Fully convolutional networks for semantic segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 640–651. [Google Scholar] [CrossRef]
- Lee, J.; Nishikawa, R.M. Automated mammographic breast density estimation using a fully convolutional network. Med. Phys. 2018, 45, 1178–1190. [Google Scholar] [CrossRef]
- Ben-Ari, R.; Akselrod-Ballin, A.; Karlinsky, L.; Hashoul, S. Domain specific convolutional neural nets for detection of architectural distortion in mammograms. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging, Melbourne, Australia, 18–21 April 2017; pp. 552–556. [Google Scholar]
- Bruno, A.; Ardizzone, E.; Vitabile, S.; Midiri, M. A novel solution based on scale invariant feature transform descriptors and deep learning for the detection of suspicious regions in mammogram images. J. Med. Signals Sens. 2020, 10, 158–173. [Google Scholar] [PubMed]
- Heath, M.; Bowyer, K.; Kopans, D.; Kegelmeyer, P.; Moore, R.; Chang, K.; Munishkumaran, S. Current status of the digital database for screening mammography. In Digital Mammography; Springer: Dordrecht, The Netherlands, 1998; pp. 457–460. [Google Scholar]
- Lee, R.S.; Gimenez, F.; Hoogi, A.; Miyake, K.K.; Gorovoy, M.; Rubin, D.L. A curated mammography data set for use in computer-aided detection and diagnosis research. Sci. Data 2017, 4, 170177. [Google Scholar] [CrossRef] [PubMed]
- Samala, R.K.; Chan, H.; Hadjiiski, L.; Helvie, M.A.; Richter, C.D.; Cha, K.H. Breast cancer diagnosis in digital breast tomosynthesis: Effects of training sample size on multi-stage transfer learning using deep neuralnets. IEEE Trans. Med. Imaging 2019, 38, 686–696. [Google Scholar] [CrossRef]
- Valkonen, M.; Isola, J.; Ylinen, O.; Muhonen, V.; Saxlin, A.; Tolonen, T.; Nykter, M.; Ruusuvuori, P. Cytokeratin-supervised deep learning for automatic recognition of epithelial cells in breast cancers stained for ER, PR, and Ki-67. IEEE Trans. Med. Imaging 2020, 39, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, H.; Higuchi, H.; Ishikawa, M. Classification of metastatic breast cancer cell using deep learning approach. In Proceedings of the 2021 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Jeju Island, Korea, 20–23 April 2021; pp. 425–428. [Google Scholar]
- Thanh, D.N.H.; Kalavathi, P.; Thanh, l.; Prasath, V.B.S. Chest X-ray image denoising using Nesterov optimization method with total variation regularization. Procedia Comput. Sci. 2020, 171, 1961–1969. [Google Scholar] [CrossRef]
- Gu, J.; Wang, Z.; Kuen, J.; Ma, L.; Shahroudy, A.; Shuai, B.; Liu, T.; Wang, X.; Wang, G.; Cai, J.; et al. Recent advances in convolutional neural network. Pattern Recognit. 2018, 77, 354–377. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Avci, O.; Abdeljaber, O.; Ince, T.; Gabbouj, M.; Inman, D.J. 1D convolutional neural networks and applications: A survey. Mech. Syst. Signal Processing 2021, 151, 107398. [Google Scholar] [CrossRef]
- Chansong, D.; Supratid, S. Impacts of Kernel size on different resized images in object recognition based on convolutional neural network. In Proceedings of the 2021 9th International Electrical Engineering Congress (iEECON), Pattaya, Thailand, 10–12 March 2021. [Google Scholar]
- Wu, J.; Chen, P.; Li, C.; Kuo, Y.; Pai, N.; Lin, C. Multilayer fractional-order machine vision classifier for rapid typical lung diseases screening on digital chest X-Ray images. IEEE Access 2020, 8, 105886–105902. [Google Scholar] [CrossRef]
- Lin, C.; Wu, J.; Li, C.; Chen, P.; Pai, N.; Kuo, Y. Enhancement of chest X-ray images to improve screening accuracy rate using iterated function system and multilayer fractional-order machine learning classifier. IEEE Photonics J. 2020, 12, 1–19. [Google Scholar] [CrossRef]
- Pilot European Image Processing Archive, The Mini-MIAS Database of Mammograms. 2012. Available online: http://peipa.essex.ac.uk/pix/mias/ (accessed on 12 July 2022).
- Mammographic Image Analysis Society (MIAS) Database v1.21. 2019. Available online: https://www.repository.cam.ac.uk/handle/1810/250394 (accessed on 12 July 2022).
- Oza, P.; Sharma, P.; Patel, S.; Bruno, A. A bottom-up review of image analysis methods for suspicious region detection in mammograms. J. Imaging 2021, 7, 190. [Google Scholar] [CrossRef]
- Chicco, D.; Jurman, G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genom. 2020, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Haffner, P. Gradient-based learning applied to document recognition. Proc. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef]
- Zhang, X. A Convolutional Neural Network Assisted Fast Tumor Screening System Based on Fractional-Order Image Enhancement: The Case of Breast X-ray Medical Imaging. Master’s Thesis, Department of Electrical Engineering, National Chin-Yi University of Technology, Taichung, Taiwan, 2021. [Google Scholar]
- Chen, P.; Zhang, X.; Wu, J.; Pai, C.C.; Hsu, J.; Lin, C.; Pai, N. Automatic breast tumor screening of mammographic images with optimal convolutional neural network. Appl. Sci. 2022, 12, 4079. [Google Scholar] [CrossRef]
- Chougrad, H.; Zouaki, H.; Alheyane, O. Deep convolutional neural networks for breast cancer screening. Comput. Methods Programs Biomed. 2018, 157, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.; Wookey, S. The real-world-weight cross-entropy loss function: Modeling the costs of mislabeling. IEEE Access 2019, 8, 4806–4813. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. In Proceedings of the 3rd International Conference for Learning Representations, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Ma, J.; Yarats, D. Quasi-hyperbolic momentum and Adam for deep learning. Proc. ICLR 2019, 2019, 1–38. [Google Scholar]
- Li, Y.; Shen, T.; Chen, C.; Chang, W.; Lee, P.; Huang, C.-C. Automatic detection of atherosclerotic plaque and calcification from intravascular ultrasound Images by using deep convolutional neural networks. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2021, 68, 1762–1772. [Google Scholar] [CrossRef]
- Lin, C.; Lai, H.; Chen, P.; Wu, J.; Pai, C.; Su, C.; Ho, H.-W. Breast lesions screening of mammographic images with 2D spatial and 1D convolutional neural network-based classifier. Appl. Sci. 2022, 12, 7516. [Google Scholar] [CrossRef]
- AlGhamdi; Abdel-Mottaleb, M.; Collado-Mesa, F. Du-net: Convolutional network for the detection of arterial calcifications in mammograms. IEEE Trans. Med. Imaging 2020, 39, 3240–3249. [Google Scholar] [CrossRef]
- Suh, Y.J.; Jung, J.; Cho, B. Automated breast cancer detection in digital mammograms of various densities via deep learning. J. Pers. Med. 2020, 10, 211. [Google Scholar] [CrossRef]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Kachuee, M.; Fazeli, S.; Sarrafzadeh, M. ECG heartbeat classification: A deep transferable representation. In Proceedings of the 2018 IEEE International Conference on Healthcare Informatics (ICHI), New York, NY, USA, 4–7 June 2018. [Google Scholar]
- Mamatov, N.; Niyozmatova, N.; Samijonov, A. Software for preprocessing voice signals. Int. J. Appl. Sci. Eng. 2020, 18, 1–8. [Google Scholar]
- Ragab, M.G.; Abdulkadir, S.J.; Aziz, N.; Alhussian, H.; Bala, A.; Alqushaibi, A. An ensemble one dimensional convolutional neural network with Bayesian optimization for environmental sound classification. Appl. Sci. 2021, 11, 4660. [Google Scholar] [CrossRef]
- Mukhamadiyev, A.; Khujayarov, I.; Djuraev, O.; Cho, J. Automatic speech recognition method based on deep learning approaches for Uzbek language. Sensors 2022, 22, 3683. [Google Scholar] [CrossRef]
- Li, S.; Dong, M.; Du, G.; Mu, X. Attention dense-u-net for automatic breast mass segmentation in digital mammogram. IEEE Access 2019, 7, 59037–59047. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual explanations from deep networks via gradient-based localization. In Proceedings of the 2017 IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar]
- Ehsan, S.; Clark, A.F.; Rehman, N.; McDonald-Maier, K.D. Integral images: Efficient algorithms for their Computation and storage in resource-constrained embedded vision systems. Sensors 2015, 15, 16804–16830. [Google Scholar] [CrossRef]
- George Moody and Roger Mark, MIT-BIH Arrhythmia Database. 2005. Version: 1.0.0. Available online: https://physionet.org/content/mitdb/1.0.0/ (accessed on 12 July 2022).
- Makeev, A.; Glick, S.J. Low-Dose contrast-enhanced breast CT using spectral shaping filters: An experimental study. IEEE Trans. Med. Image 2017, 36, 2417–2423. [Google Scholar] [CrossRef]
- Wu, J.; Chen, P.; Lin, C.; Chen, S.; Shung, K.K. Breast benign and malignant tumors rapidly screening by ARFI-VTI elastography and random decision forests based classifier. IEEE Access 2020, 8, 54019–54034. [Google Scholar] [CrossRef]
- Gubern-M’erida, A.; Kallenberg, M.; Mann, R.M.; Martí, R.; Karssemeijer, N. Breast segmentation and density estimation in breast MRI: A fully automatic framework. IEEE J. Biomed. Health Inform. 2015, 19, 349–357. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CNN Model | 1st Layer | 2nd Layer | 3rd Layer | 4th Layer | 5th Layer | Stride | Padding |
|---|---|---|---|---|---|---|---|
| 1 | 3 × 3, 16 2 × 2, 16 | - | - | - | - | 1 2 | 1 |
| 2 | 3 × 3, 16 2 × 2, 16 | 5 × 5, 16 2 × 2, 16 | - | - | - | 1 2 | 1 |
| 3 | 3 × 3, 16 2 × 2, 16 | 5 × 5, 16 2 × 2, 16 | 7 × 7, 16 2 × 2, 16 | - | - | 1 2 | 1 |
| 4 | 3 × 3, 16 2 × 2, 16 | 5 × 5, 16 2 × 2, 16 | 7 × 7, 16 2 × 2, 16 | 9 × 9, 16 2 × 2, 16 | - | 1 2 | 1 |
| 5 | 3 × 3, 16 2 × 2, 16 | 5 × 5, 16 2 × 2, 16 | 7 × 7, 16 2 × 2, 16 | 9 × 9, 16 2 × 2, 16 | 11 × 11, 16 2 × 2, 16 | 1 2 | 1 |
| Model | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Training CPU Time (min) | <30 | <240 | <7 | <10 | <180 |
| Average Accuracy (%) | 90.99% | 90.34% | 95.92% | 95.28% | 95.71% |
| Model | 1st Convolutional Window and Window Size | 2nd Convolutional Window and Window Size | 3rd Convolutional Window and Window Size | Stride/Padding | Maximum Pooling Window | Stride |
|---|---|---|---|---|---|---|
| 1 | Fractional Order, 3 × 3, 2 | Kernel, 3 × 3, 16 | Kernel, 3 × 3, 16 | 1/1 | 2 × 2, 16 | 2 |
| 2 | Kernel, 3 × 3, 16 | Kernel, 3 × 3, 16 | Kernel, 3 × 3, 16 | 1/1 | 2 × 2, 16 | 2 |
| Test Fold | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Average Accuracy (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model | ||||||||||||
| 1 | 96.14 | 97.43 | 98.07 | 97.96 | 98.93 | 98.07 | 96.35 | 95.60 | 96.89 | 98.28 | 97.37 | |
| 2 | 97.00 | 96.60 | 95.40 | 96.20 | 97.60 | 94.40 | 95.00 | 98.10 | 96.00 | 95.00 | 95.93 | |
| Model | 1st Convolutional Window and Window Size | 2nd Convolutional Window and Window Size | 3rd Convolutional Window and Window Size | Stride/Padding | Maximum Pooling Window | Stride |
|---|---|---|---|---|---|---|
| 2-1 | Kernel, 3 × 3, 4 | Kernel, 3 × 3, 4 | Kernel, 3 × 3, 4 | 1/1 | 2 × 2, 4, 8, 16, 32 | 2 |
| 2-2 | Kernel, 3 × 3, 8 | Kernel, 3 × 3, 8 | Kernel, 3 × 3, 8 | 1/1 | 2 | |
| 2-3 | Kernel, 3 × 3, 16 | Kernel, 3 × 3, 16 | Kernel, 3 × 3, 16 | 1/1 | 2 | |
| 2-4 | Kernel, 3 × 3, 32 | Kernel, 3 × 3, 32 | Kernel, 3 × 3, 32 | 1/1 | 2 |
| Model | Average Precision (%) | Average Recall (%) | Average Accuracy (%) | Average F1 Score | Average CPU Time (s) for Training |
|---|---|---|---|---|---|
| 2-1 | 92.03 | 88.94 | 91.57 | 0.9076 | 148.02 |
| 2-2 | 94.77 | 92.81 | 95.03 | 0.9389 | 237.39 |
| 2-3 | 95.19 | 95.19 | 95.04 | 0.9516 | 308.38 |
| 2-4 | 94.06 | 93.60 | 95.30 | 0.9395 | 332.05 |
| Model | First Convolutional Pooling Layer | Second Convolutional Pooling Layer | Third Convolutional Pooling Layer | Classification Layer | Average Training Time (s) | Average Accuracy (%) |
|---|---|---|---|---|---|---|
| 3-1 | 2D Kernel Convolutional Process, 3 × 3, 8 (Stride = 1) Maximum Pooling, 2 × 2, 8 (Stride = 2) | Flattening Process 1D Kernel Convolutional Process, 1 × 100, 8 | 1D Kernel Convolutional Process, 1 × 100, 8 1D Pooling Processes (Stride = 10) | BPNN: Input Layer (250 nodes), 1st Hidden Layer (64 nodes), 2nd Hidden Layer (64 nodes), and Output Layer (2 nodes) | 322.74 (Loss = 0.1211) | 93.40 |
| 3-2 | Flattening Process 1D Kernel Convolutional Process, 1 × 100, 8 1D Pooling Processes (Stride = 10) | - | 305.39 (Loss = 0.1650) | 94.00 | ||
| 3-3 | 2D Kernel Convolutional Process, 3 × 3, 4 (Stride = 1) Maximum Pooling, 2 × 2, 4 (Stride = 2) | Flattening Process 1D Kernel Convolutional Process, 1 × 100, 4 | 1D Kernel Convolutional Process, 1 × 100, 4 1D Pooling Processes (Stride = 10) | 347.67 (Loss = 0.2293) | 91.20 | |
| 3-4 | Flattening Process 1D Kernel Convolutional Process, 1 × 100, 4 1D Pooling Processes (Stride = 10) | - | 324.27 (Loss = 0.1538) | 94.80 |
| Literature | Database | Method | Purpose |
|---|---|---|---|
| [42] | MIAS Image Database [30,31] | 2D spatial and 1D CNN | Breast Lesions Screening Precision: 96.70%; Recall: 96.13%; Accuracy: 96.40%; F1 Score: 0.9641 |
| [43] | CBIS-DDSM Database [20] | Dense-Unet Model | Calcification Detection Sensitivity: 91.22%; Specificity: 92.01%; Accuracy: 91.47%; F1 Score: 0.9219 |
| [44] | Collected by Department of Breast and Endocrine Surgery at Hallym University Sacred Heart Hospital [44] | DenseNet-169, EfficientNet-B5 | Automated Breast Cancer Detection (1) DenseNet-169: AUC = 0.952 ± 0.005; Mean Sensitivity: 87.0%; Mean Specificity: 88.4%; Mean Accuracy: 88.1% (2) EfficientNet-B5: AUC = 0.954 ± 0.020; Mean Sensitivity: 88.3%; Mean Specificity: 87.9%; Mean Accuracy: 87.9% |
| [4] | E-Da Hospital Image Database [4] | DNN (Deep Neural Network) | BI-RADS Classification Sensitivity: 95.31%; Specificity: 99.15%; Accuracy: 94.22% [49] |
| [11] | DDSM Database [19] | Attention Dense-Unet Model | Mass Segmentation Sensitivity: 77.89%; Specificity: 84.69%; Accuracy: 78.38% |
| [45] | MIT-BIH Arrhythmia Dataset [53] | 11-layer 1D CNN (DNN) | Arrhythmia Detection Precision: 75.91%; Recall: 92.88%; Accuracy: 95.85%; F1 Score: 0.8115 |
| [46] | MIT-BIH Arrhythmia Dataset [53] | 11-layer 2D CNN (DNN) | Arrhythmia Detection Precision: 89.31%; Recall: 91.69%; Accuracy: 89.31%; F1 Score: 0.8957 |
| [48] | 8732 Urban Sounds (Ten Classes) [48] | 1D CNN (DNN) 3, 5, and 10-Convolution Cross-Validation | Environmental Sound Classification Average Accuracy: 94.46% |
| [49] | Uzbek Dataset Consists of 207 h of Transcribed Audio Spoken by 1281 Speakers [49] | Deep Neural Network Hidden Markov Model (DNN-HMM) | Automatic Speech Recognition for Uzbek Language Training Accuracy: 96% Testing Accuracy: 93% |
| [50] | Audio and Video: AVEC2013 and AVEC2014 Database [50] | 1D CNN and 2D CNN | Depression Recognition RMSE 7–10 MAE: 5–9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, F.-Z.; Lin, C.-H.; Chen, P.-Y.; Pai, N.-S.; Su, C.-M.; Pai, C.-C.; Ho, H.-W. Number of Convolution Layers and Convolution Kernel Determination and Validation for Multilayer Convolutional Neural Network: Case Study in Breast Lesion Screening of Mammographic Images. Processes 2022, 10, 1867. https://doi.org/10.3390/pr10091867
Zhang F-Z, Lin C-H, Chen P-Y, Pai N-S, Su C-M, Pai C-C, Ho H-W. Number of Convolution Layers and Convolution Kernel Determination and Validation for Multilayer Convolutional Neural Network: Case Study in Breast Lesion Screening of Mammographic Images. Processes. 2022; 10(9):1867. https://doi.org/10.3390/pr10091867
Chicago/Turabian StyleZhang, Feng-Zhou, Chia-Hung Lin, Pi-Yun Chen, Neng-Sheng Pai, Chun-Min Su, Ching-Chou Pai, and Hui-Wen Ho. 2022. "Number of Convolution Layers and Convolution Kernel Determination and Validation for Multilayer Convolutional Neural Network: Case Study in Breast Lesion Screening of Mammographic Images" Processes 10, no. 9: 1867. https://doi.org/10.3390/pr10091867
APA StyleZhang, F.-Z., Lin, C.-H., Chen, P.-Y., Pai, N.-S., Su, C.-M., Pai, C.-C., & Ho, H.-W. (2022). Number of Convolution Layers and Convolution Kernel Determination and Validation for Multilayer Convolutional Neural Network: Case Study in Breast Lesion Screening of Mammographic Images. Processes, 10(9), 1867. https://doi.org/10.3390/pr10091867