
Comparative Analysis of Clinical and Epidemiological Characteristics in Patients with SARI Confirmed as Influenza or COVID-19 Admitted in a Tertiary Care Hospital in Bucharest, Romania

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Ethics Approval
3. Results
3.1. Characteristics of Patients with Laboratory-Confirmed Influenza in the 2018–2019 Season
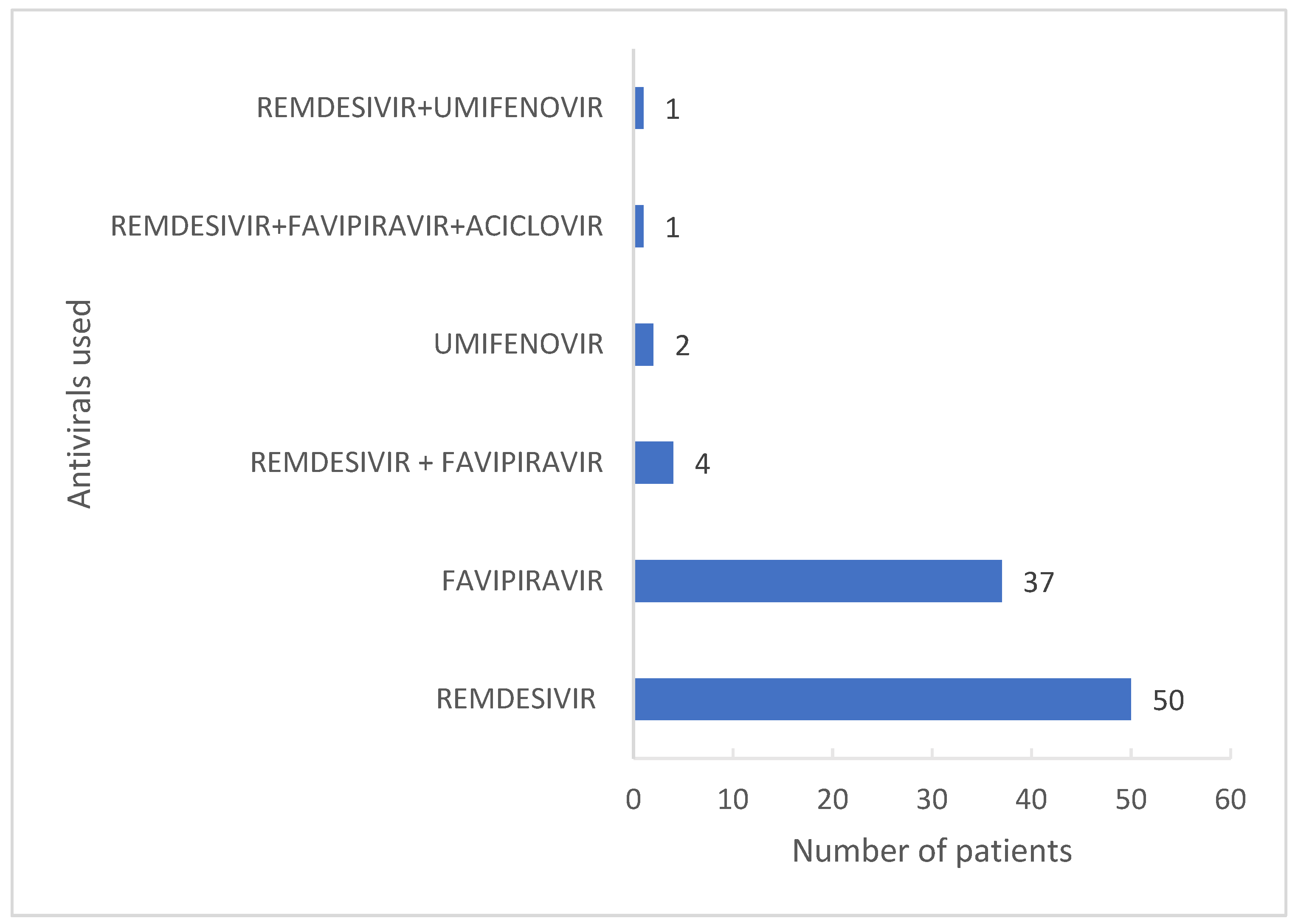
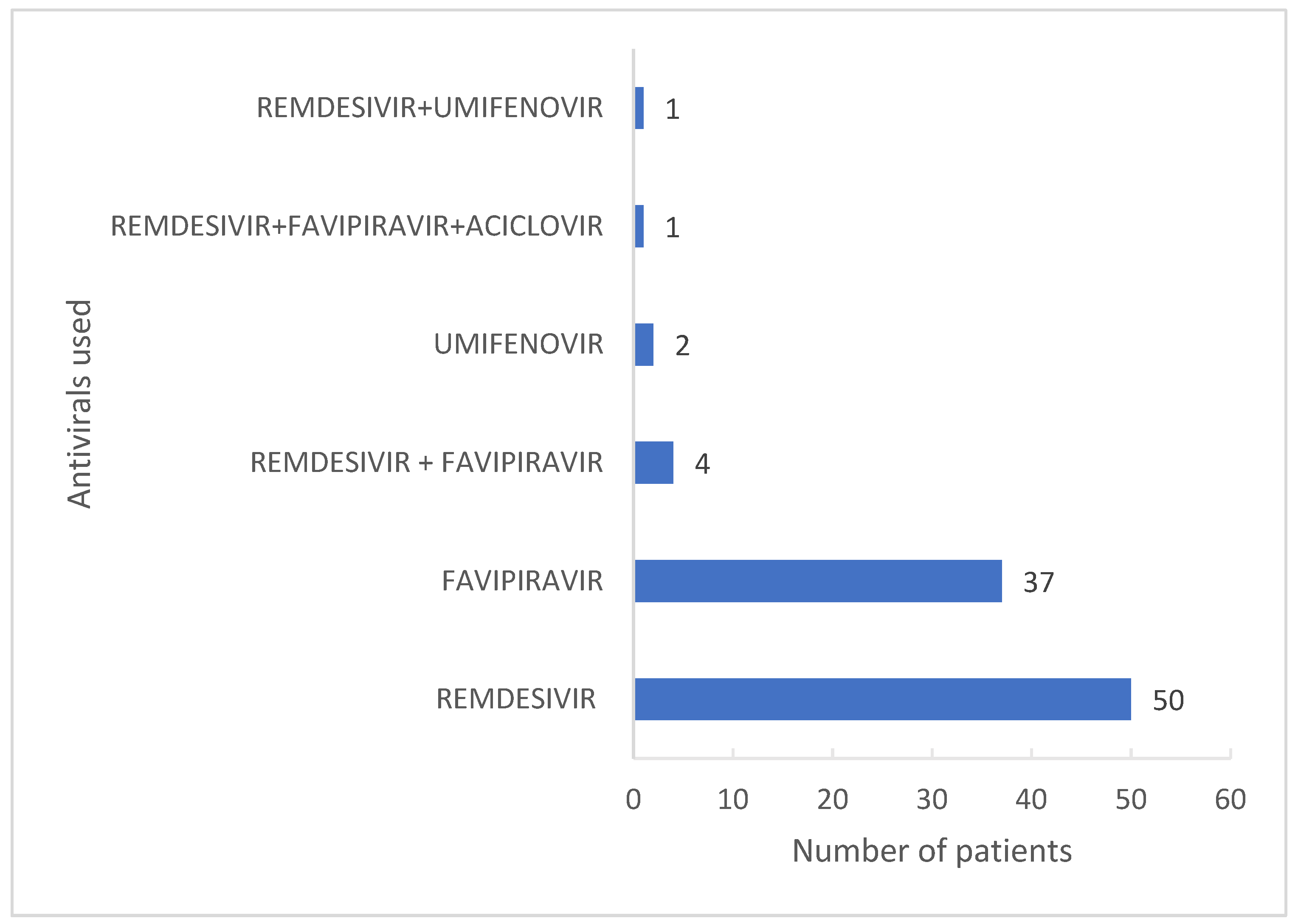
3.2. Characteristics of Patients with Laboratory-Confirmed COVID-19 in the 2020–2021 Season
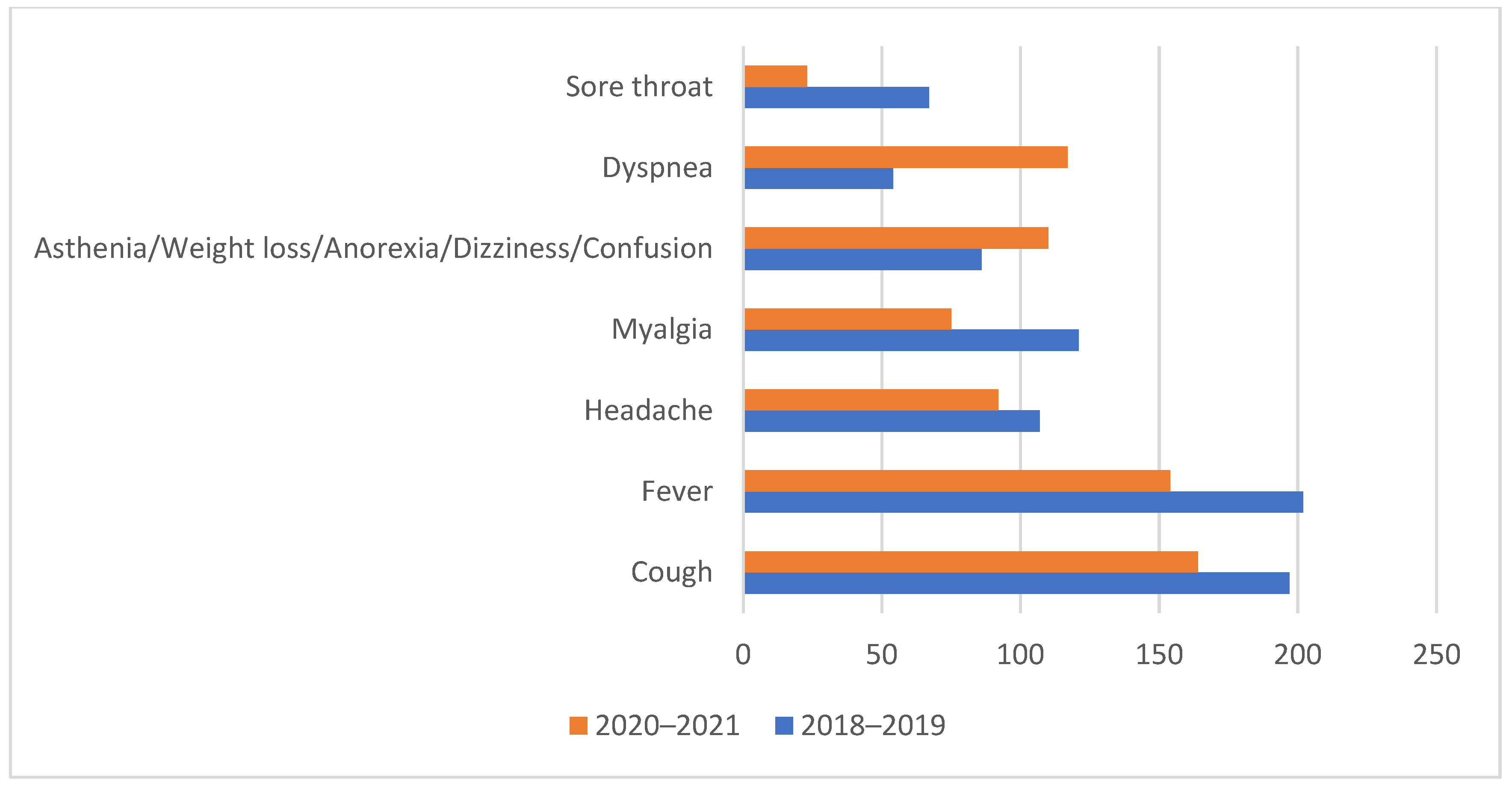
3.3. Comparison of Cases of Laboratory-Confirmed Influenza and COVID-19 in the Two Pre-Pandemic and COVID-19 Pandemic Seasons
4. Discussion
- The data were collected from a single hospital and cannot be generalized to the country.
- We cannot exclude an involuntary selection bias driven by hospital admission of severe COVID-19 cases.
- The data for the 2018–2019 season are only relevant for the circulating subtypes in that respective season, preponderantly A/H1, and to a smaller extent A/H3, while no B influenza viruses circulated that season. Given the differences in terms of clinical presentation and clinical outcomes between different influenza types or subtypes, a further analysis of multiple influenza seasons is warranted, to account for potential biases.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dascălu, S. The Successes and Failures of the Initial COVID-19 Pandemic Response in Romania. Front. Public Health 2020, 8, 344. [Google Scholar] [CrossRef] [PubMed]
- Drăgănescu, A.; Săndulescu, O.; Florea, D.; Vlaicu, O.; Streinu-Cercel, A.; Oțelea, D.; Luminos, M.L.; Aramă, V.; Abrudan, S.; Streinu-Cercel, A.; et al. The 2017–2018 influenza season in Bucharest, Romania: Epidemiology and characteristics of hospital admissions for influenza-like illness. BMC Infect. Dis. 2019, 19, 967. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, H.; Boneva, D.; Elkbuli, A. The intersection of viral illnesses: A seasonal influenza epidemic amidst the COVID-19 pandemic. Ann. Med. Sur. 2020, 60, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Harrington, W.N.; Kackos, C.M.; Webby, R.J. The evolution and future of influenza pandemic preparedness. Exp. Mol. Med. 2021, 53, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Laurie, K.L.; Rockman, S. Which influenza viruses will emerge following the SARS-CoV-2 pandemic? Influenza Other Respir. Viruses 2021, 15, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Pițigoi, D.; Nițescu, M.; Streinu-Cercel, A.; Bacruban, R.; Ivanciuc, A.E.; Lazăr, M.; Cherciu, C.M.; Crăciun, M.D.; Aramă, V.; Streinu-Cercel, A.; et al. Characteristics of influenza in elderly patients with and without diabetes, hospitalized for severe acute respiratory infection in a tertiary care hospital from Bucharest Romania—A three-year prospective epidemiological surveillance study. Germs 2019, 9, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control, Estimated Flu-Related Illnesses, Medical visits, Hospitalizations, and Deaths in the United States—2018–2019 Flu Season. Available online: https://www.cdc.gov/flu/about/burden/2018-2019.html (accessed on 24 November 2021).
- World Health Organization, Review of the 2018–2019 Influenza Season in the Northern Hemisphere. Available online: https://www.who.int/publications-detail-redirect/who-wer-9432-345-363 (accessed on 24 November 2021).
- Adlhoch, C.; Mook, P.; Lamb, F.; Ferland, L.; Melidou, A.; Amato-Gauci, A.; Pebody, R. The European Influenza Surveillance Network, Very little influenza in the WHO European Region during the 2020/21 season, weeks 40 2020 to 8 2021. Eurosurveillance 2021, 26, 2–9. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Seasonal influenza. In Annual Epidemiological Report 2020; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- European Centre for Disease Prevention and Control. Seasonal influenza 2018–2019. In Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2019. [Google Scholar]
- Centrul Național de Supraveghere şi Control Boli Transmisibile, Evolutia Infectiilor Respiratorii Acute, a Gripei si a Infectiilor Respiratorii Acute Severe (SARI) in Sezonul 2020–2021. Available online: http://cnscbt.ro/index.php/informari-saptamanale/gripa/2475-informare-infectii-respiratorii-17-05-2021-23-05-2021-s-20/file (accessed on 17 June 2021).
- Emborg, H.D.; Carnahan, A.; Bragstad, K.; Trebbien, R.; Brytting, M.; Hungnes, O.; Byström, E.; Vestergaard, L. Abrupt termination of the 2019/20 influenza season following preventive measures against COVID-19 in Denmark, Norway and Sweden. Eurosurveillance 2021, 26, 10–15. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control, Data on Country Response Measures to COVID-19. 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/download-data-response-measures-covid-19 (accessed on 18 June 2021).
- Groves, H.E.; Piché-Renaud, P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; Sevenhuysen, C.; Campigotto, A.; Gubbay, J.B.; Morris, S.K. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada. Lancet Reg. Health-Am. 2021, 1, 100015. [Google Scholar] [PubMed]
- Noh, J.Y.; Seong, H.; Yoon, J.G.; Song, J.Y.; Cheong, H.J.; Kim, W.J. Social distancing against covid-19: Implication for the control of influenza. J. Korean Med. Sci. 2020, 35, e182. [Google Scholar] [CrossRef]
- Flerlage, T.; Boyd, D.F.; Meliopoulos, V.; Thomas, P.G.; Schultz-Cherry, S. Influenza virus and SARS-CoV-2: Pathogenesis and host responses in the respiratory tract. Nat. Rev. Microbiol. 2021, 19, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Ministerul Sănătății, Ordinul nr. 555 din 3 Aprilie 2020 Privind Aprobarea Planului de Măsuri Pentru Pregătirea Spitalelor în Contextul Epidemiei de Coronavirus COVID-19, a Listei Spitalelor Care Asigură Asistenţa Medicală Pacienţilor Testaţi Pozitiv cu Virusul SARS-CoV-2 în Faza I şi în Faza a II-a şi a Listei cu Spitalele de Suport Pentru Pacienţii Testaţi Pozitiv sau Suspecţi cu Virusul SARS-CoV-2. Available online: https://legislatie.just.ro/Public/DetaliiDocument/224705 (accessed on 17 November 2021).
- Drăgănescu, A.; Săndulescu, O.; Florea, D.; Vlaicu, O.; Streinu-Cercel, A.; Oţelea, D.; Aramă, V.; Luminos, M.L.; Streinu-Cercel, A.; Niţescu, M.; et al. The influenza season 2016/17 in Bucharest, Romania—Surveillance data and clinical characteristics of patients with influenza-like illness admitted to a tertiary infectious diseases hospital. Braz. J. Infect. Dis. 2018, 22, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Puig-Barberà, J.; Tormos, A.; Trushakova, S.; Sominina, A.; Pisareva, M.; Ciblak, M.A.; Badur, S.; Yu, H.; Cowling, B.J.; Burtseva, E. The Global Influenza Hospital Surveillance Network (GIHSN): A new platform to describe the epidemiology of severe influenza. Influenza Other Respir. Viruses 2015, 9, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Miron, V.D.; Bănică, L.; Săndulescu, O.; Paraschiv, S.; Surleac, M.; Florea, D.; Vlaicu, O.; Milu, P.; Streinu-Cercel, A.; Bilașco, A.; et al. Clinical and molecular epidemiology of influenza viruses from Romanian patients hospitalized during the 2019/20 season. PLoS ONE 2021, 16, e0258798. [Google Scholar] [CrossRef] [PubMed]
- Centrul Național pentru Supraveghere și Control Boli Transmisbile, Evoluția Infecțiilor Respiratorii Acute, a Gripei și a Infecțiilor Respiratorii Acute Severe (SARI) în Sezonul 2018–2019. Available online: https://www.cnscbt.ro/index.php/analiza-date-supraveghere/gripa-si-infectii-respiratorii-acute/1208-analiza-sezon-gripal-2018-2019/file (accessed on 24 November 2021).
- Centrul Național Pentru Supraveghere și Control Boli Transmisbile, Analiză Sezon Gripal 2018–2019. Available online: http://www.cnscbt.ro/index.php/prezentari/ateliere-de-lucru-infectii-respiratorii-acute-gripa-sari-1-2-noiembrie-2019/2116-analiza-sezonul-gripal-2018-2019-1/file (accessed on 24 November 2021).
- European Centre for Disease Prevention and Control, COVID-19 Situation Update for the EU/EEA, as of 24 November 2021. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 24 November 2021).
- Olaru, O.G.; Badiu, D.C.; Stănescu, A.D.; Pena, C.M.; Papacocea, R.I.; Balcangiu Stroescu, A. Study of available antiviral treatments for COVID-19 during pregnancy. Farmacia 2020, 68, 957–965. [Google Scholar] [CrossRef]
- Jones, W.A.; de Cassia Castro, R.; Masters, H.L.; Carrico, R. Influenza Management during the COVID-19 Pandemic: A Review of Recent Innovations in Antiviral Therapy and Relevance to Primary Care Practice. Mayo Clin. Proc. Innov. Qual. Outcome 2021, 5, 974–991. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Influenza n (%) | COVID-19 n (%) | Statistical Analysis (z-, p-Values) | |
|---|---|---|---|---|
| Sex | Male | 84 (40.4 %) | 128 (67.0%) | −5.3252, p < 0.00001 |
| Age | 18 years–65 years | 138 (66.3%) | 126 (66.0%) | 0.0796, p = 0.93624 |
| >65 years | 70 (33.7%) | 65 (34.0%) | −0.0796, p = 0.93624 | |
| Symptoms at hospital admission | Cough | 197 (94.7%) | 164 (85.9%) | 3.0076, p = 0.00262 |
| Fever | 202 (97.1%) | 154 (80.6%) | 5.3054, p < 0.00001 | |
| Malaise | 121 (58.2%) | 131 (68.6%) | −2.1541, p = 0.03156 | |
| Headache | 107 (51.4%) | 92 (48.2%) | 0.6535, p = 0.5157 | |
| Myalgia | 121 (58.2%) | 75 (39.3%) | 3.7736, p = 0.00016 | |
| Asthenia/weight loss/anorexia/ dizziness/ confusion | 86 (41.3%) | 110 (57.6%) | −3.2426, p = 0.0012 | |
| Dyspnea | 54 (26.0%) | 117 (61.3%) | −7.1168, p < 0.00001 | |
| Sore throat | 67 (32.2% ) | 23 (12.0%) | 4.8154, p < 0.00001 | |
| Body mass index | <18.5 | 9 (4.3%) | 0 (0.0%) | 2.9078, p = 0.00362 |
| 18.5–24.9 | 99 (47.6%) | 42 (22.0%) | 5.3452, p < 0.00001 | |
| 25–29.9 | 57 (27.4%) | 71 (37.2%) | −2.0883, p = 0.03662 | |
| ≥30 | 43 (20.7%) | 78 (40.8%) | −4.3773, p < 0.00001 | |
| Comorbidities | Cardiovascular diseases | 72 (44.7%) | 66 (45.5%) | −0.1399, p = 0.88866 |
| Obesity | 43 (26.7%) | 78 (53.8%) | −4.8385, p < 0.00001 | |
| Diabetes | 39 (24.2%) | 34 (23.4%) | 0.1589, p = 0.87288 | |
| Pulmonary diseases | 43 (26.7%) | 11 (7.6%) | 4.3812, p < 0.00001 | |
| Liver diseases | 25 (15.5%) | 12 (8.3%) | 1.9429, p = 0.05238 | |
| Immunodeficiency, including HIV | 26 (16.1%) | 10 (6.9%) | 2.5083, p = 0.01208 | |
| Chronic renal Impairment | 17 (10.6%) | 12 (8.3%) | 0.6809, p = 0.4965 | |
| Cancer | 20 (12.4%) | 9 (6.2%) | 1.8535, p = 0.06432 | |
| Rheumatological/ autoimmune diseases | 15 (9.3%) | 7 (4.6%) | 1.5179, p = 0.12852 | |
| Neurological diseases | 8 (5.0%) | 5 (3.4%) | 0.6585, p = 0.50926 | |
| Other comorbidities | 76 (47.2%) | 39 (26.9%) | 3.6624, p = 0.00026 | |
| Evolution and clinical outcome | Requirement of supplementary oxygen | 21 (10.1%) | 72 (37.7%) | −6.514, p = < 0.00001 |
| Admission to intensive care | 5 (2.4%) | 15 (7.9%) | −2.4921, p = < 0.01278 | |
| Mechanical ventilation | 4 (1.9%) | 15 (7.9%) | −2.7787, p = 0.00544 | |
| Death | 5 (2.4%) | 15 (7.9%) | −2.4921, p = < 0.01278 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enciu, B.G.; Drăgănescu, A.C.; Pițigoi, D.; Săndulescu, O.; Crăciun, M.D.; Bilașco, A.; Streinu-Cercel, A.; Streinu-Cercel, A.; Florea, D.; Miron, V.D.; et al. Comparative Analysis of Clinical and Epidemiological Characteristics in Patients with SARI Confirmed as Influenza or COVID-19 Admitted in a Tertiary Care Hospital in Bucharest, Romania. Processes 2022, 10, 327. https://doi.org/10.3390/pr10020327
Enciu BG, Drăgănescu AC, Pițigoi D, Săndulescu O, Crăciun MD, Bilașco A, Streinu-Cercel A, Streinu-Cercel A, Florea D, Miron VD, et al. Comparative Analysis of Clinical and Epidemiological Characteristics in Patients with SARI Confirmed as Influenza or COVID-19 Admitted in a Tertiary Care Hospital in Bucharest, Romania. Processes. 2022; 10(2):327. https://doi.org/10.3390/pr10020327
Chicago/Turabian StyleEnciu (Milcu), Bianca Georgiana, Anca Cristina Drăgănescu, Daniela Pițigoi, Oana Săndulescu, Maria Dorina Crăciun, Anuța Bilașco, Anca Streinu-Cercel, Adrian Streinu-Cercel, Dragoș Florea, Victor Daniel Miron, and et al. 2022. "Comparative Analysis of Clinical and Epidemiological Characteristics in Patients with SARI Confirmed as Influenza or COVID-19 Admitted in a Tertiary Care Hospital in Bucharest, Romania" Processes 10, no. 2: 327. https://doi.org/10.3390/pr10020327
APA StyleEnciu, B. G., Drăgănescu, A. C., Pițigoi, D., Săndulescu, O., Crăciun, M. D., Bilașco, A., Streinu-Cercel, A., Streinu-Cercel, A., Florea, D., Miron, V. D., & Aramă, V. (2022). Comparative Analysis of Clinical and Epidemiological Characteristics in Patients with SARI Confirmed as Influenza or COVID-19 Admitted in a Tertiary Care Hospital in Bucharest, Romania. Processes, 10(2), 327. https://doi.org/10.3390/pr10020327