
The Association between Obesity and Depression among Children and the Role of Family: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
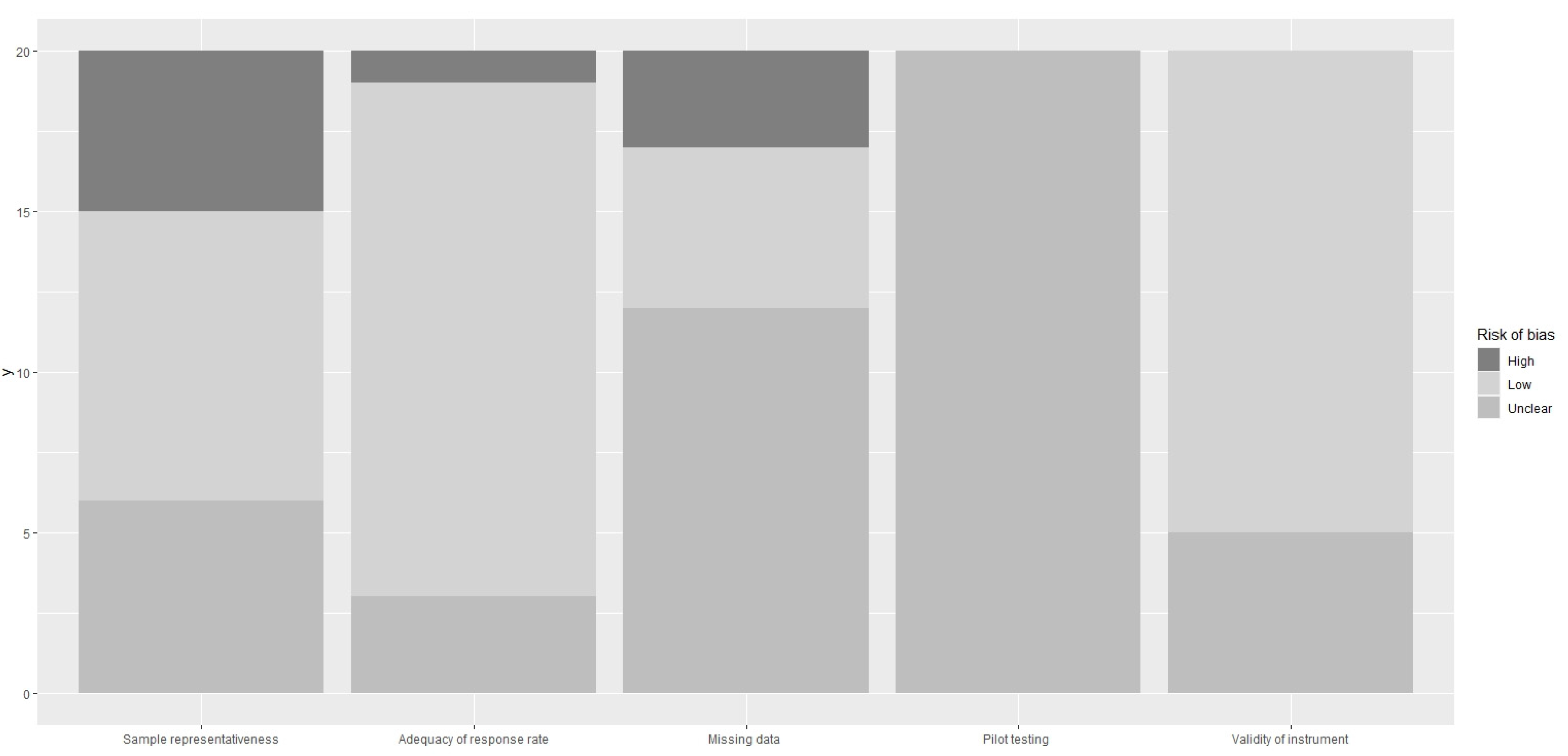
2.5. Risk of Bias Assessment
3. Results
3.1. Does Depression Lead to Obesity?
3.1.1. Case-Control Studies
3.1.2. Cross-Sectional Studies
3.1.3. Longitudinal Studies
3.1.4. Systematic Reviews and Meta-Analyses
3.2. Does Obesity Lead to Depression?
3.2.1. Case-Control Studies
3.2.2. Cross-Sectional Studies
3.2.3. Longitudinal Studies
3.2.4. Systematic Reviews and Meta-Analyses
3.3. Does the Family Environment Affect the Association between Obesity and Depression?
3.4. Risk of Bias Assessment Results
4. Discussion
4.1. Does Depression Lead to Obesity?
4.2. Does Obesity Lead to Depression?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blasco, B.V.; García-Jiménez, J.; Bodoano, I.; Gutiérrez-Rojas, L. Obesity and Depression: Its Prevalence and Influence as a Prognostic Factor: A Systematic Review. Psychiatry Investig. 2020, 17, 715–724. [Google Scholar] [CrossRef]
- Nemiary, D.; Shim, R.; Mattox, G.; Holden, K. The relationship between obesity and depression among adolescents. Psychiatr. Ann. 2012, 42, 305–308. [Google Scholar] [CrossRef]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- American Psychiatric Association. What Is Depression? Available online: https://www.psychiatry.org/patients-families/depression/what-is-depression (accessed on 19 March 2022).
- Sagar, R.; Gupta, T. Psychological aspects of obesity in children and adolescents. Indian J. Pediatr. 2018, 85, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.; Matthews, L.; Cobley, S.; Han, A.; Sanders, R.; Wiltshire, H.D.; Baker, J.S. Psychological consequences of childhood obesity: Psychiatric comorbidity and prevention. Adolesc. Health Med. Ther. 2016, 7, 125. [Google Scholar] [CrossRef] [PubMed]
- Mühlig, Y.; Antel, J.; Föcker, M.; Hebebrand, J. Are bidirectional associations of obesity and depression already apparent in childhood and adolescence as based on high-quality studies? A systematic review. Obes. Rev. 2016, 17, 235–249. [Google Scholar] [CrossRef]
- Small, L.; Aplasca, A. Child obesity and mental health: A complex interaction. Child Adolesc. Psychiatr. Clin. N. Am. 2016, 25, 269–282. [Google Scholar] [CrossRef]
- Anderson, S.E.; Cohen, P.; Naumova, E.N.; Must, A. Association of depression and anxiety disorders with weight change in a prospective community-based study of children followed up into adulthood. Arch. Pediatr. Adolesc. Med. 2006, 160, 285–291. [Google Scholar] [CrossRef]
- Phillips, B.A.; Gaudette, S.; McCracken, A.; Razzaq, S.; Sutton, K.; Speed, L.; Thompson, J.; Ward, W. Psychosocial functioning in children and adolescents with extreme obesity. J. Clin. Psychol. Med. Settings 2012, 19, 277–284. [Google Scholar] [CrossRef]
- Davison, K.K.; Jurkowski, J.M.; Lawson, H.A. Reframing family-centred obesity prevention using the Family Ecological Model. Public Health Nutr. 2013, 16, 1861–1869. [Google Scholar] [CrossRef]
- Lovejoy, M.C.; Graczyk, P.A.; O’Hare, E.; Neuman, G. Maternal depression and parenting behavior: A meta-analytic review. Clin. Psychol. Rev. 2000, 20, 561–592. [Google Scholar] [CrossRef]
- Markowitz, S.; Friedman, M.A.; Arent, S.M. Understanding the relation between obesity and depression: Causal mechanisms and implications for treatment. Clin. Psychol. Sci. Pract. 2008, 15, 1. [Google Scholar] [CrossRef]
- Korczak, D.J.; Lipman, E.; Morrison, K.; Szatmari, P. Are children and adolescents with psychiatric illness at risk for increased future body weight? A systematic review. Dev. Med. Child Neurol. 2013, 55, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Latzer, Y.; Stein, D. A review of the psychological and familial perspectives of childhood obesity. J. Eat. Disord 2013, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Esposito, M.; Gallai, B.; Roccella, M.; Marotta, R.; Lavano, F.; Lavano, S.M.; Mazzotta, G.; Bove, D.; Sorrentino, M.; Precenzano, F.; et al. Anxiety and depression levels in prepubertal obese children: A case-control study. Neuropsychiatr. Dis. Treat. 2014, 10, 1897–1902. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Erriu, M.; Jezek, S.; Almenara, C.A.; Tambelli, R. Trajectories of aggressive and depressive symptoms in male and female overweight children: Do they share a common path or do they follow different routes? PLoS ONE 2018, 13, e0190731. [Google Scholar] [CrossRef]
- Chung, K.H.; Chiou, H.Y.; Chen, Y.H. Psychological and physiological correlates of childhood obesity in Taiwan. Sci. Rep. 2015, 5, 17439. [Google Scholar] [CrossRef]
- Byrne, M.E.; Tanofsky-Kraff, M.; Lavender, J.M.; Parker, M.N.; Shank, L.M.; Swanson, T.N.; Ramirez, Ε.; LeMay-Russell, S.; Yang, S.B.; Brady, S.M.; et al. Bridging executive function and disinhibited eating among youth: A network analysis. Int. J. Eat. Disord. 2021, 54, 721–732. [Google Scholar] [CrossRef]
- Lynch, T.; Azuero, A.; Lochman, J.E.; Park, N.J.; Turner-Henson, A.; Rice, M. The Influence of Psychological Stress, Depressive Symptoms, and Cortisol on Body Mass and Central Adiposity in 10-to-12-Year-Old Children. J. Pediatr. Nurs. 2019, 44, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Wickrama, K.K.; O’Neal, C.W.; Oshri, A. Are stressful developmental processes of youths leading to health problems amplified by genetic polymorphisms? The case of body mass index. J. Youth Adolesc. 2014, 43, 1096–1109. [Google Scholar] [CrossRef]
- Schwartz, B.S.; Glass, T.A.; Pollak, J.; Hirsch, A.G.; Bailey-Davis, L.; Moran, T.H.; Bandeen-Roche, K. Depression, its comorbidities and treatment, and childhood body mass index trajectories. Obesity 2016, 24, 2585–2592. [Google Scholar] [CrossRef] [PubMed]
- Olive, L.S.; Telford, R.M.; Byrne, D.G.; Abhayaratna, W.P.; Telford, R.D. Symptoms of stress and depression effect percentage of body fat and insulin resistance in healthy youth: LOOK longitudinal study. Health Psychol. 2017, 36, 749. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.M.; Garber, A.K.; Tabler, J.L.; Murray, S.B.; Bibbins-Domingo, K. Differential Risk Factors for Unhealthy Weight Control Behaviors by Sex and Weight Status Among U.S. Adolescents. J. Adolesc. Health 2018, 63, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Pine, A.; Barch, D.M.; Luby, J.; Whalen, D.J. Emotion Identification in Preschool and Early Adolescent Body Mass Index: Exploring the Roles of Depressive Symptoms and Peer Relations. Child Psychiatry Hum. Dev. 2020, 51, 321–329. [Google Scholar] [CrossRef]
- Moradi, M.; Mozaffari, H.; Askari, M.; Azadbakht, L. Association between overweight/obesity with depression, anxiety, low self-esteem, and body dissatisfaction in children and adolescents: A systematic review and meta-analysis of observational studies. Crit. Rev. Food Sci Nutr. 2020, 62, 555–570. [Google Scholar] [CrossRef]
- Topçu, S.; Orhon, F.Ş.; Tayfun, M.; Uçaktürk, S.A.; Demirel, F. Anxiety, depression and self-esteem levels in obese children: A case-control study. J. Pediatr. Endocrinol. Metab. 2016, 29, 357–361. [Google Scholar] [CrossRef]
- Sepulveda, A.R.; Blanco, M.; Nova, E.; Marcos, A.; Martínez, S.G.; Carrobles, J.A.; Graell, M. Identifying the relationship between biological, psychosocial and family markers associated with childhood obesity: Case-control “ANOBAS” study. Psychoneuroendocrinology 2019, 110, 104428. [Google Scholar] [CrossRef]
- Lindberg, L.; Hagman, E.; Danielsson, P.; Marcus, C.; Persson, M. Anxiety and depression in children and adolescents with obesity: A nationwide study in Sweden. BMC Med. 2020, 18, 30. [Google Scholar] [CrossRef]
- Sepúlveda, A.R.; Solano, S.; Blanco, M.; Lacruz, T.; Graell, M. Prevalence of childhood mental disorders in overweight and obese Spanish children: Identifying loss of control eating. Psychiatry Res. 2018, 267, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.J.; Kim, H.S.; Yoon, K.H. Analyzing the distinguishing factors that affect childhood obesity in South Korea. Front. Med. 2018, 12, 707–716. [Google Scholar] [CrossRef]
- Blanco, M.; Solano, S.; Alcántara, A.I.; Parks, M.; Román, F.J.; Sepúlveda, A.R. Psychological well-being and weight-related teasing in childhood obesity: A case–control study. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2019, 25, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, A.R.; Lacruz, T.; Solano, S.; Blanco, M.; Moreno, A.; Rojo, M.; Beltrán, L.; Graell, M. Identifying Loss of Control Eating within Childhood Obesity: The Importance of Family Environment and Child Psychological Distress. Children 2020, 7, 225. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.W.; Lin, C.Y.; Strong, C.; Liu, C.H.; Hsieh, Y.P.; Lin, Y.C.; Tsai, M.C. Psychological correlates of eating behavior in overweight/obese adolescents in Taiwan: Psychometric and correlation analysis of the Three-Factor Eating Questionnaire (TFEQ)-R21. Pediatr. Neonatol. 2021, 62, 41–48. [Google Scholar] [CrossRef]
- Lim, H.J.; Chung, S.S.; Joung, K.H. Factors of depressive symptoms among elementary, middle, and high school students. Arch. Psychiatr. Nurs. 2016, 30, 302–308. [Google Scholar] [CrossRef]
- Gibson, L.Y.; Allen, K.L.; Davis, E.; Blair, E.; Zubrick, S.R.; Byrne, S.M. The psychosocial burden of childhood overweight and obesity: Evidence for persisting difficulties in boys and girls. Eur. J. Pediatr. 2017, 176, 925–933. [Google Scholar] [CrossRef]
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A systematic review of Australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef]
- Quek, Y.H.; Tam, W.W.; Zhang, M.W.; Ho, R.C. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef]
- Köhler, C.A.; Evangelou, E.; Stubbs, B.; Solmi, M.; Veronese, N.; Belbasis, L.; Bortolato, B.; Meloa, M.C.A.; Coelho, C.A.; Fernandes, B.S.; et al. Mapping risk factors for depression across the lifespan: An umbrella review of evidence from meta-analyses and Mendelian randomization studies. J. Psychiatr. Res. 2018, 103, 189–207. [Google Scholar] [CrossRef]
- Sutaria, S.; Devakumar, D.; Yasuda, S.S.; Das, S.; Saxena, S. Is obesity associated with depression in children? Systematic review and meta-analysis. Arch. Dis Child. 2019, 104, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, E.; Canals, J.; Arija, V.; De Henauw, S.; Michels, N. The role of emotion regulation in childhood obesity: Implications for prevention and treatment. Nutr. Res. Rev. 2016, 29, 17–29. [Google Scholar] [CrossRef]
- Fabricatore, A.N.; Wadden, T.A. Psychological aspects of obesity. Clin. Dermatol. 2004, 22, 332–337. [Google Scholar] [CrossRef]
- Wardle, J.; Cooke, L. The impact of obesity on psychological well-being. Best Pr. Res. Clin. Endocrinol. Metab. 2005, 19, 421–440. [Google Scholar] [CrossRef] [PubMed]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Kovacs, M. The Children’s Depression Inventory: A Self-Rated Depression Scale for School-Aged Youngsters; University of Pittsburgh, School of Medicine, Department of Psychiatry, Western Psychiatric Institute and Clinic: Pittsburgh, PA, USA, 1983. [Google Scholar]
- Nibras, S.; Kentor, R.; Masood, Y.; Price, K.; Schneider, N.M.; Tenenbaum, R.B.; Calarge, C. Psychological and Psychiatric Comorbidities in Youth with Serious Physical Illness. Children 2022, 9, 1051. [Google Scholar] [CrossRef]
- Rojo, M.; Solano, S.; Lacruz, T.; Baile, J.I.; Blanco, M.; Graell, M.; Sepúlveda, A.R. Linking psychosocial stress events, psychological disorders and childhood obesity. Children 2021, 8, 211. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Keyword Combinations | No of Records |
|---|---|
| (childhood obesity) AND (childhood depression) AND (family role) | 27 |
| (childhood obesity) AND (childhood depression) AND (family structure) | 12 |
| (childhood obesity) AND (childhood depression) | 362 |
| (childhood obesity) AND (childhood mental health) AND (family role) | 38 |
| (childhood obesity) AND (childhood mental health) AND (family structure) | 15 |
| (childhood obesity) AND (childhood mental health) | 467 |
| Total | 921 |
| Author (Year) | Sample and Country | Study Type | Main Findings |
|---|---|---|---|
| Esposito et al. (2014) [18] | 148 children (8 to 12 years of age) | Case-control study | Significantly higher level of depressive and anxious symptomatology among the group with obesity in comparison to the control group |
| Cerniglia et al. (2018) [19] | 180 children (2 to 8 years of age) | Case-control study | Normal-weight children had lower depressive symptoms compared with overweight youths. Overweight females showed lower depressive scores than overweight males at 2 years of age. |
| Chung et al. (2015) [20] | 302 children from Taipei, Taiwan | Cross-sectional study | No significant difference in depression between the healthy-weight and overweight children or with obesity. |
| Byrne et al. (2021) [21] | 248 children (8 to 17 years-old) | Cross-sectional study | No association between depressive symptoms and obesity |
| Lynch et al. (2019) [22] | 147 children (10 to 12 years-old) | Cross-sectional study | Depressive symptoms explained a significant amount of the variance in the body mass index (BMI) and central adiposity when gender, race/ethnicity, puberty, and socioeconomic status were controlled |
| Wickrama et al. (2014) [23] | 12,424 adolescents (12 to 19 years of age) | Longitudinal study | Adolescents with more depressive symptoms and adolescents with more genetic risk alleles had a higher BMI compared with adolescents with fewer depressive symptoms and risk alleles. |
| Schwartz et al. (2016) [24] | 105,163 children (8 to 18 years of age) | Longitudinal study | Children who had experienced at least one depressive event had a higher average BMI than children without such an experience; the older the children, the stronger the association. |
| Olive et al. (2017) [25] | 791 healthy Australian children (7 to 8 years of age) | Longitudinal study | Both boys and girls with higher depressive symptoms had a higher percentage of body fat. |
| Nagata et al. (2018) [26] | 14,322 U.S. adolescents | Longitudinal study | Depressive symptoms were associated with increased odds of unhealthy weight control behaviors in females; no association was found in boys. |
| Pine et al. (2019) [27] | 231 preschoolers in St. Louis, MI, USA | Longitudinal study | There was a significant positive association between preschool depressive symptoms and adolescent BMI. |
| Moradi et al. (2020) [28] | NA | Meta-analysis | No association was observed between overweight and the risk of depression (pooled risk estimate: 1.00, 95% CI: 0.92–1.08, p = 0.97). Moreover, there was not any relationship between obesity and the risk of depression (pooled risk estimate: 1.08, 95% CI: 0.97–1.21, p = 0.17). |
| Author (Year) | Sample and Country | Study Type | Main Findings |
|---|---|---|---|
| Topçu et al. (2016) [29] | 167 children with obesity and 200 normal-weight children aged 9–16 years | Case-control study | Obesity in children was associated with a significantly higher rate of depression and anxiety, and lower self-esteem scores. There were significant differences among them with obesity and control groups in terms of the total score of CDI [12 (4–39)] versus [8 (3–19)]; p < 0.001 |
| Sepulveda et al. (2019) [30] | 100 preadolescents (aged 8 to 12 years) from Madrid, Spain | Case-control study | Obese preadolescents reported higher levels of depression |
| Lindberg et al. (2020) [31] | 12,507 Swedish children aged 6–17 in the Swedish childhood obesity treatment register (BORIS, 2005–2015) compared with a matched group of 60,063 children from the general population | Case-control study | Obesity was a significant risk factor for anxiety and depression. Girls with obesity had a 43% higher risk of anxiety and depression compared with girls in the general population. A similar result held for boys (adjusted HR, 1.33). |
| Sepulveda et al. (2018) [32] | 170 children aged 8 to 12 years from different health centers in Madrid, Spain | Cross-sectional study | Five percent of the sample was diagnosed with major depression |
| Yang et al. (2018) [33] | 197 elementary school students and 461 middle school students | Cross-sectional study | Childhood obesity can cause depression and reduce children’s quality of life because of their distorted body perception |
| Blanco et al. (2019) [34] | 50 Spanish preadolescents with obesity | Cross-sectional study | Obese children reported higher depression. |
| Sepulveda et al. (2020) [35] | Nine Spanish families of children aged 8 to 12 years | Cross-sectional study | Positive association between weight status and depression (measured through CDI). |
| Lin et al. (2021) [36] | 445 Taiwanese children aged 13 to 15 years | Cross-sectional study | No difference in depression between normal-weight and overweight/obese children (4.85 ± 3.53 vs. 4.81 ± 3.96) |
| Lim et al. (2016) [37] | 759 high-grade elementary school students, 609 middle school students, and 496 high school students | Longitudinal study | Obesity was among the meaningful variables of depressive symptoms from childhood to adolescence. |
| Gibson et al. (2017) [38] | 212 children aged 8 to 13 years | Longitudinal study | Overweight girls and girls with obesity reported greater impairment in depression as well as in other areas of psychological difficulties than normal-weight girls. No such association was found for boys. |
| Sanders et al. (2015) [39] | NA | Systematic review | A high depression prevalence in overweight children and children with obesity was identified in Australian children and adolescents |
| Quek et al. (2017) [40] | 51,272 participants | Meta-analysis | There was a positive association between childhood and adolescent obesity and depression and more severe depressive symptoms in the groups with obesity. |
| Köhler et al. (2018) [41] | NA | Systematic review (umbrella review) | Obesity and metabolic abnormalities constituted risk factors for depression. |
| Sutaria et al. (2019) [42] | 143,603 children | Meta-analysis | Obese female children had significantly increased odds of concurrent and future depression compared with non-obese female children. |
| Smith et al. (2020) [43] | NA | Literature review | Psychological conditions, such as low self-esteem, depression, and eating disorders can result from excess weight in childhood. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanellopoulou, A.; Antonogeorgos, G.; Douros, K.; Panagiotakos, D.B. The Association between Obesity and Depression among Children and the Role of Family: A Systematic Review. Children 2022, 9, 1244. https://doi.org/10.3390/children9081244
Kanellopoulou A, Antonogeorgos G, Douros K, Panagiotakos DB. The Association between Obesity and Depression among Children and the Role of Family: A Systematic Review. Children. 2022; 9(8):1244. https://doi.org/10.3390/children9081244
Chicago/Turabian StyleKanellopoulou, Aikaterini, George Antonogeorgos, Konstantinos Douros, and Demosthenes B. Panagiotakos. 2022. "The Association between Obesity and Depression among Children and the Role of Family: A Systematic Review" Children 9, no. 8: 1244. https://doi.org/10.3390/children9081244
APA StyleKanellopoulou, A., Antonogeorgos, G., Douros, K., & Panagiotakos, D. B. (2022). The Association between Obesity and Depression among Children and the Role of Family: A Systematic Review. Children, 9(8), 1244. https://doi.org/10.3390/children9081244