
Effect of Small Volume Blood Sampling on the Outcomes of Very Low Birth Weight Preterm Infants


Abstract

1. Introduction
2. Materials and Methods
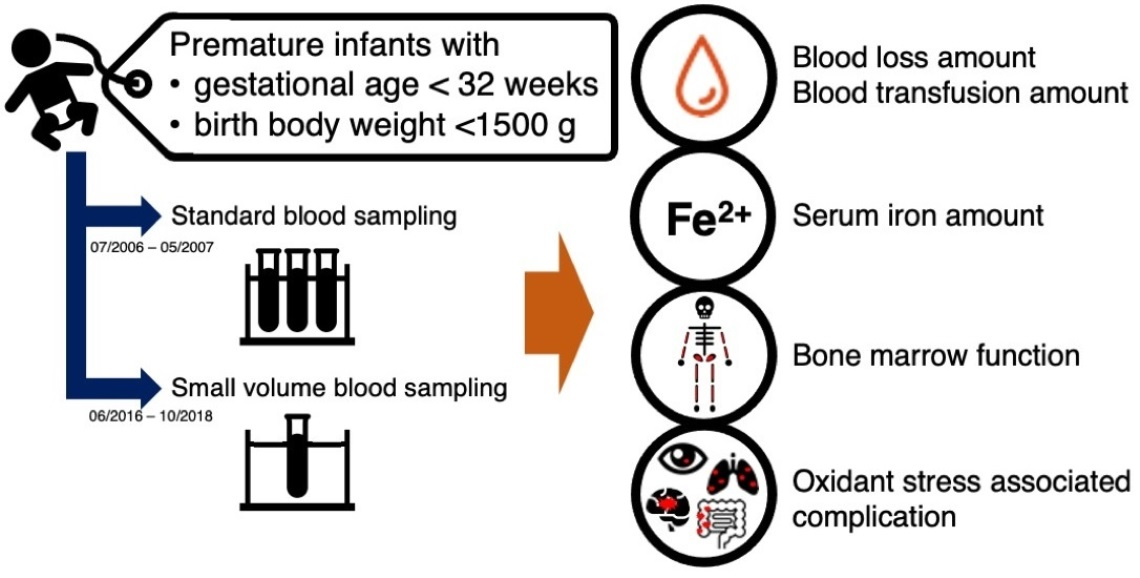
2.1. Study Design and Data Collection
2.2. Ethics Statement
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Packed Red Blood Cell Transfusion, Blood Loss, and Iron Status at Day 30
3.3. Clinical Outcomes
3.4. Factors for Complications Related to Oxidative Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saito-Benz, M.; Flanagan, P.; Berry, M.J. Management of anaemia in pre-term infants. Br. J. Haematol. 2020, 188, 354–366. [Google Scholar] [CrossRef]
- Strauss, R.G. Anaemia of prematurity: Pathophysiology and treatment. Blood Rev. 2010, 24, 221–225. [Google Scholar] [CrossRef]
- Cooke, R.W.; Drury, J.A.; Yoxall, C.W.; James, C. Blood transfusion and chronic lung disease in preterm infants. Eur. J. Pediatr. 1997, 156, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Saugstad, O.D. Bronchopulmonary dysplasia-oxidative stress and antioxidants. Semin. Neonatol. 2003, 8, 39–49. [Google Scholar] [CrossRef]
- Englert, J.A.; Saunders, R.A.; Purohit, D.; Hulsey, T.C.; Ebeling, M. The effect of anemia on retinopathy of prematurity in extremely low birth weight infants. J. Perinatol. 2001, 21, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.L.; Tseng, H.I.; Lu, C.C.; Yang, S.N.; Fan, H.C.; Yang, R.C. Effect of blood transfusions on the outcome of very low body weight preterm infants under two different transfusion criteria. Pediatr. Neonatol. 2009, 50, 110–116. [Google Scholar] [CrossRef]
- Lin, J.C.; Strauss, R.G.; Kulhavy, J.C.; Johnson, K.J.; Zimmerman, M.B.; Cress, G.A.; Connolly, N.W.; Widness, J.A. Phlebotomy overdraw in the neonatal intensive care nursery. Pediatrics 2000, 106, e19. [Google Scholar] [CrossRef]
- Strauss, R.G. Practical issues in neonatal transfusion practice. Am. J. Clin. Pathol. 1997, 107, S57–S63. [Google Scholar]
- Kirpalani, H.; Bell, E.F.; Hintz, S.R.; Tan, S.; Schmidt, B.; Chaudhary, A.S.; Johnson, K.J.; Crawford, M.M.; Newman, J.E.; Vohr, B.R.; et al. Higher or Lower Hemoglobin Transfusion Thresholds for Preterm Infants. N. Engl. J. Med. 2020, 383, 2639–2651. [Google Scholar] [CrossRef]
- Ozdemir, Z.; Torer, B.; Hanta, D.; Cetinkaya, B.; Gulcan, H.; Tarcan, A. Determination of tissue hypoxia by physicochemical approach in premature anemia. Pediatr. Neonatol. 2017, 58, 425–429. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hwang, J.S.; Rehan, V.K. Recent Advances in Bronchopulmonary Dysplasia: Pathophysiology, Prevention, and Treatment. Lung 2018, 196, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Di Pietro, G.M.; Esposito, S. Bronchopulmonary dysplasia: Clinical aspects and preventive and therapeutic strategies. J. Transl. Med. 2018, 16, 36. [Google Scholar] [CrossRef] [PubMed]
- Shohat, M.; Reisner, S.H.; Krikler, R.; Nissenkorn, I.; Yassur, Y.; Ben-Sira, I. Retinopathy of prematurity: Incidence and risk factors. Pediatrics 1983, 72, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Cooke, R.W.; Clark, D.; Hickey-Dwyer, M.; Weindling, A.M. The apparent role of blood transfusions in the development of retinopathy of prematurity. Eur. J. Pediatr. 1993, 152, 833–836. [Google Scholar] [CrossRef]
- Hesse, L.; Eberl, W.; Schlaud, M.; Poets, C.F. Blood Transfusion, Iron Load, and Retinopathy of Prematurity. Eur. J. Pediatr. 1997, 156, 465–470. [Google Scholar] [CrossRef]
- Zhu, Z.; Hua, X.; Yu, Y.; Zhu, P.; Hong, K.; Ke, Y. Effect of red blood cell transfusion on the development of retinopathy of prematurity: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0234266. [Google Scholar] [CrossRef]
- Hay, S.; Zupancic, J.A.; Flannery, D.D.; Kirpalani, H.; Dukhovny, D. Should we believe in transfusion-associated enterocolitis? Applying a GRADE to the literature. Semin Perinatol. 2017, 41, 80–91. [Google Scholar] [CrossRef]
- Teišerskas, J.; Bartašienė, R.; Tamelienė, R. Associations between red blood cell transfusions and necrotizing enterocolitis in very low birth weight infants: Ten-year data of a tertiary neonatal unit. Medicina 2019, 55, 16. [Google Scholar] [CrossRef]
- Mohamed, A.; Shah, P.S. Transfusion associated necrotizing enterocolitis: A meta-analysis of observational data. Pediatrics 2012, 129, 529–540. [Google Scholar] [CrossRef]
- Stokes, V.; Rajai, A.; Mukherjee, D.; Mukherjee, A. Transfusion-associated necrotizing enterocolitis (NEC) in extremely preterm infants: Experience of a tertiary neonatal center in UK. J. Matern. Fetal Neonatal Med. 2021, 20, 1–6. [Google Scholar] [CrossRef]
- Sayari, A.J.; Tashiro, J.; Sola, J.E.; Perez, E.A. Blood transfusions, increased rates of surgical NEC, and lower survival: A propensity score-matched analysis. J. Pediatr. Surg. 2016, 51, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.T.; Saroha, V.; Patel, R.M. Transfusion-related Gut Injury and Necrotizing Enterocolitis. Clin. Perinatol. 2020, 47, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Bell, E.F. When to transfuse preterm babies. Arch. Dis. Child. Fetal Neonatal Ed. 2008, 93, F469–F473. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; O’Brien, K.O. Pregnancy and iron homeostasis: An update. Nutr. Rev. 2013, 71, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Hirano, K.; Morinobu, T.; Kim, H.; Hiroi, M.; Ban, R.; Ogawa, S.; Ogihara, H.; Tamai, H.; Ogihara, T. Blood transfusion in-creases radical promoting non-transferrin bound iron in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 84, F188–F193. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Small Volume Blood Sampling | Standard Blood Sampling | p-Value |
|---|---|---|---|
| (n = 84) | (n = 20) | ||
| Mean ± SD | Mean ± SD | ||
| Infant at birth | |||
| Gestational age (week) | 29 ± 2 | 29 ± 3 | 0.659 |
| Birth weight (g) | 1191 ± 245 | 1118 ± 302 | 0.463 |
| Small for gestational age, n (%) | 20 (23.8) | 3 (15) | 0.394 |
| Male, n (%) | 37 (44.1) | 13 (65) | 0.092 |
| Multiple births, n (%) | 32 (38.1) | 6 (30) | 0.499 |
| Apgar score at 1 min | 5.4 ± 1.7 | 5.3 ± 1.8 | 0.735 |
| Apgar score at 5 min | 7.0 ± 1.8 | 7.0 ± 1.1 | 0.635 |
| Data at birth | |||
| Hemoglobin (g/dL) | 16.2 ± 1.9 | 18.3 ± 7.0 | 0.867 |
| Hematocrit (%) | 48.4 ± 5.6 | 45.0 ± 12.5 | 0.575 |
| Small Volume Blood Sampling | Standard Blood Sampling | p-Value | |
|---|---|---|---|
| (n = 84) | (n = 20) | ||
| Mean ± SD | Mean ± SD | ||
| Age at 1st PRBC˙ transfusion (day-old) | 16.0 ± 10.4 | 10.8 ± 7.9 | 0.061 |
| Blood loss volume via phlebotomy (mL) by day 30 | 22.1 ± 8.4 | 52.5 ± 18.4 | <0.0001 |
| PRBC˙ transfusion volume (mL) by day 30 | 12.8 ± 16.0 | 26.0 ± 16.0 | 0.001 |
| Lab data at 30-day-old | |||
| Hematocrit (%) | 29.8 ± 4.0 | 21.4 ± 13.2 | 0.014 |
| Reticulocyte (%) | 5.2 ± 4.4 | 3.3 ± 3.6 | 0.008 |
| Iron (ug/dL) | 71.7 ± 20.6 | 48.3 ± 33.2 | 0.003 |
| Ferritin (ug/L) | 123.3 ± 107.5 | 160.9 ± 174.5 | 0.670 |
| Lactate level (mmol/L) | 2.0 ± 1.1 | 1.2 ± 0.9 | 0.004 |
| Small Volume Blood Sampling | Standard Blood Sampling | p-Value | |
|---|---|---|---|
| (n = 84) | (n = 20) | ||
| Mean ± SD | Mean ± SD | ||
| Feeding amount (mL) by day 30 | |||
| Total feeding volume | 4269.4 ± 2199.7 | 1451.6 ± 1477.7 | <0.0001 |
| Human milk/Donor human milk | 2683.6 ± 1795.3 | 1160.2 ± 1189.4 | 0.001 |
| Preterm formula | 1581.8 ± 1661.2 | 291.5 ± 623.9 | <0.0001 |
| Duration of parental nutrition used (Day) | |||
| 20.6 ± 20.4 | 48.8 ± 32.5 | 0.0002 | |
| Regression Coefficient | 95% CI * | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Feeding volume by day 30 | 0.002 | 0.002 | 0.010 | 0.002 |
| PRBC transfusion volume by day 30 | 0.223 | −0.107 | 0.777 | 0.115 |
| Birth body weight | 0.014 | −0.045 | 0.479 | 0.254 |
| Gestational age | 1.593 | −3.027 | 3.299 | 0.932 |
| Blood loss volume via phlebotomy by day 30 | 0.234 | −0.449 | 0.479 | 0.950 |
| Outcomes | Small Blood Sampling | Standard Blood Sampling | p-Value |
|---|---|---|---|
| (n = 84) | (n = 20) | ||
| N (%) | N (%) | ||
| Proportion of associated condition (%) | |||
| Respiratory distress syndrome with the need for surfactant therapy | 22 (26.2) | 9 (45) | 0.098 |
| Intraventricular hemorrhage | 24 (28.6) | 6 (30.0) | 0.899 |
| Severe intraventricular hemorrhage | 2 (2.38) | 2 (10.0) | 0.111 |
| Patent ductus arteriosus | 44 (52.4) | 10 (50.0) | 0.848 |
| Apnea of prematurity | 73 (86.9) | 12 (60.0) | 0.093 |
| Retinopathy of prematurity | 25 (29.8) | 5 (25.0) | 0.749 |
| Bronchopulmonary dysplasia | 35 (41.7) | 4 (20.0) | 0.072 |
| NEC 1, all stage | 5 (5.95) | 1 (5.0) | 0.869 |
| Confirmed NEC 1 (≥2a Bell’s stage) | 1 (1.2) | 1 (5.0) | 0.265 |
| Culture proved sepsis | 10 (11.9) | 9 (45.0) | 0.001 |
| Duration of associated condition (days) (Mean ± SD) | |||
| Time to regain birth body weight | 12.7 ± 5.0 | 18.1 ± 7.0 | 0.003 |
| Time on a ventilator or nasal CPAP 2 | 43.5 ± 23.6 | 32.3 ± 25.2 | 0.073 |
| Time on supplemental oxygen | 1.3 ± 3.7 | 1.1 ± 2.8 | 0.966 |
| Hospital stays | 67.2 ± 23.7 | 84.2 ± 44.2 | 0.181 |
| PRBC Transfusion Volume by Day 30 | Birth Body Weight | Blood Loss Volume via Phlebotomy by Day 30 | Gestational Age | |||
|---|---|---|---|---|---|---|
| IVH 1 | Regression coefficient | 0.021 | 0.001 | 0.018 | 0.164 | |
| 95% CI * | Upper | 0.080 | 0.005 | 0.024 | 0.241 | |
| Lower | −0.003 | −0.0003 | −0.046 | −0.402 | ||
| p-value | 0.067 | 0.096 | 0.537 | 0.624 | ||
| NEC 2 | Regression coefficient | 0.042 | 0.002 | 0.031 | 0.312 | |
| 95% CI * | Upper | 0.180 | 0.007 | 0.042 | 0.800 | |
| Lower | 0.017 | −0.002 | −0.080 | −0.424 | ||
| p-value | 0.018 | 0.296 | 0.536 | 0.548 | ||
| BPD 3 | Regression coefficient | 0.020 | 0.001 | 0.018 | 0.146 | |
| 95% CI * | Upper | 0.079 | 0.001 | 0.010 | 0.348 | |
| Lower | −0.002 | −0.003 | −0.061 | −0.227 | ||
| p-value | 0.064 | 0.137 | 0.165 | 0.680 | ||
| ROP 4 | Regression coefficient | 0.022 | 0.001 | 0.020 | 0.187 | |
| 95% CI * | Upper | 0.066 | 0.002 | 0.022 | 0.051 | |
| Lower | −0.021 | −0.003 | −0.055 | −0.690 | ||
| p-value | 0.315 | 0.600 | 0.429 | 0.117 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, P.-C.; Chung, H.-W.; Yang, S.-T.; Chen, H.-L. Effect of Small Volume Blood Sampling on the Outcomes of Very Low Birth Weight Preterm Infants. Children 2022, 9, 1190. https://doi.org/10.3390/children9081190
Su P-C, Chung H-W, Yang S-T, Chen H-L. Effect of Small Volume Blood Sampling on the Outcomes of Very Low Birth Weight Preterm Infants. Children. 2022; 9(8):1190. https://doi.org/10.3390/children9081190
Chicago/Turabian StyleSu, Pin-Chun, Hao-Wei Chung, Shu-Ting Yang, and Hsiu-Lin Chen. 2022. "Effect of Small Volume Blood Sampling on the Outcomes of Very Low Birth Weight Preterm Infants" Children 9, no. 8: 1190. https://doi.org/10.3390/children9081190
APA StyleSu, P.-C., Chung, H.-W., Yang, S.-T., & Chen, H.-L. (2022). Effect of Small Volume Blood Sampling on the Outcomes of Very Low Birth Weight Preterm Infants. Children, 9(8), 1190. https://doi.org/10.3390/children9081190