
Physical Activity Design for Balance Rehabilitation in Children with Autism Spectrum Disorder

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Evaluation
2.3. Statistical Analysis
2.4. Training Program—Physical Activity (P.A.)
- Positive influence on the body scheme representation;
- Recovery of laterality disturbances;
- Recovery of orientation, organizing, and spatial structure problems;
- Recovery of orientation and temporal structuring disorders;
- Recovery of balance and coordination disorders.
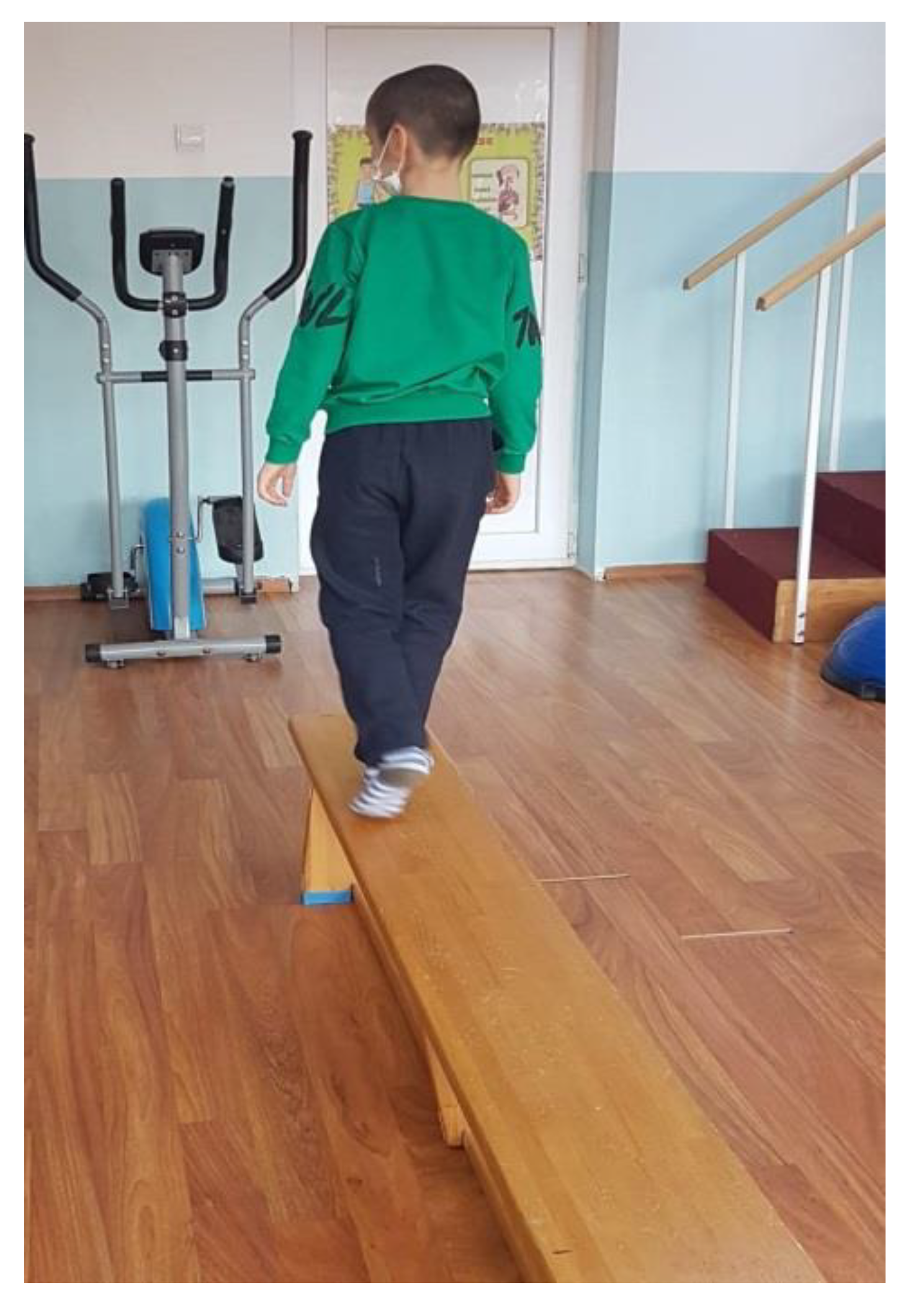
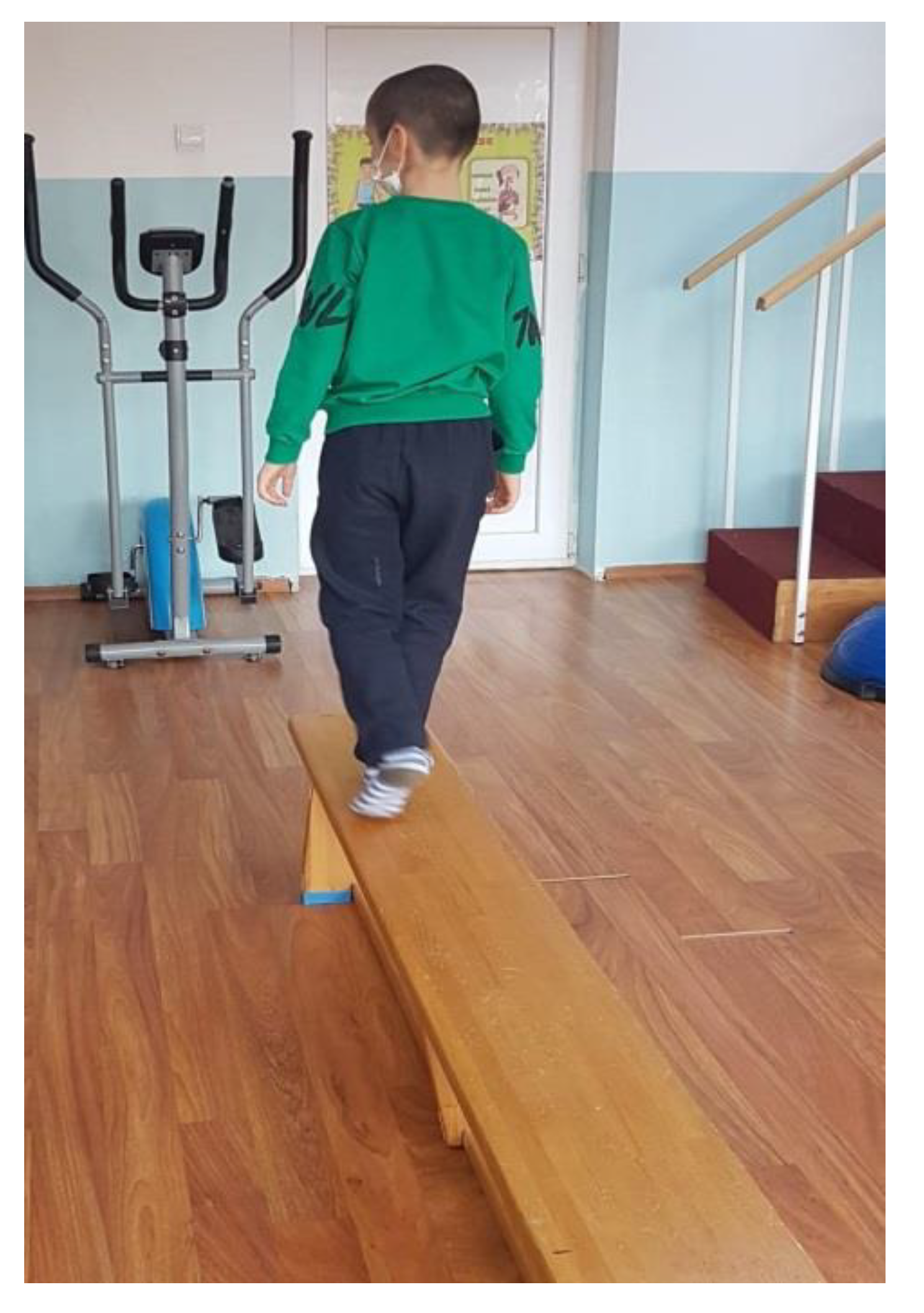
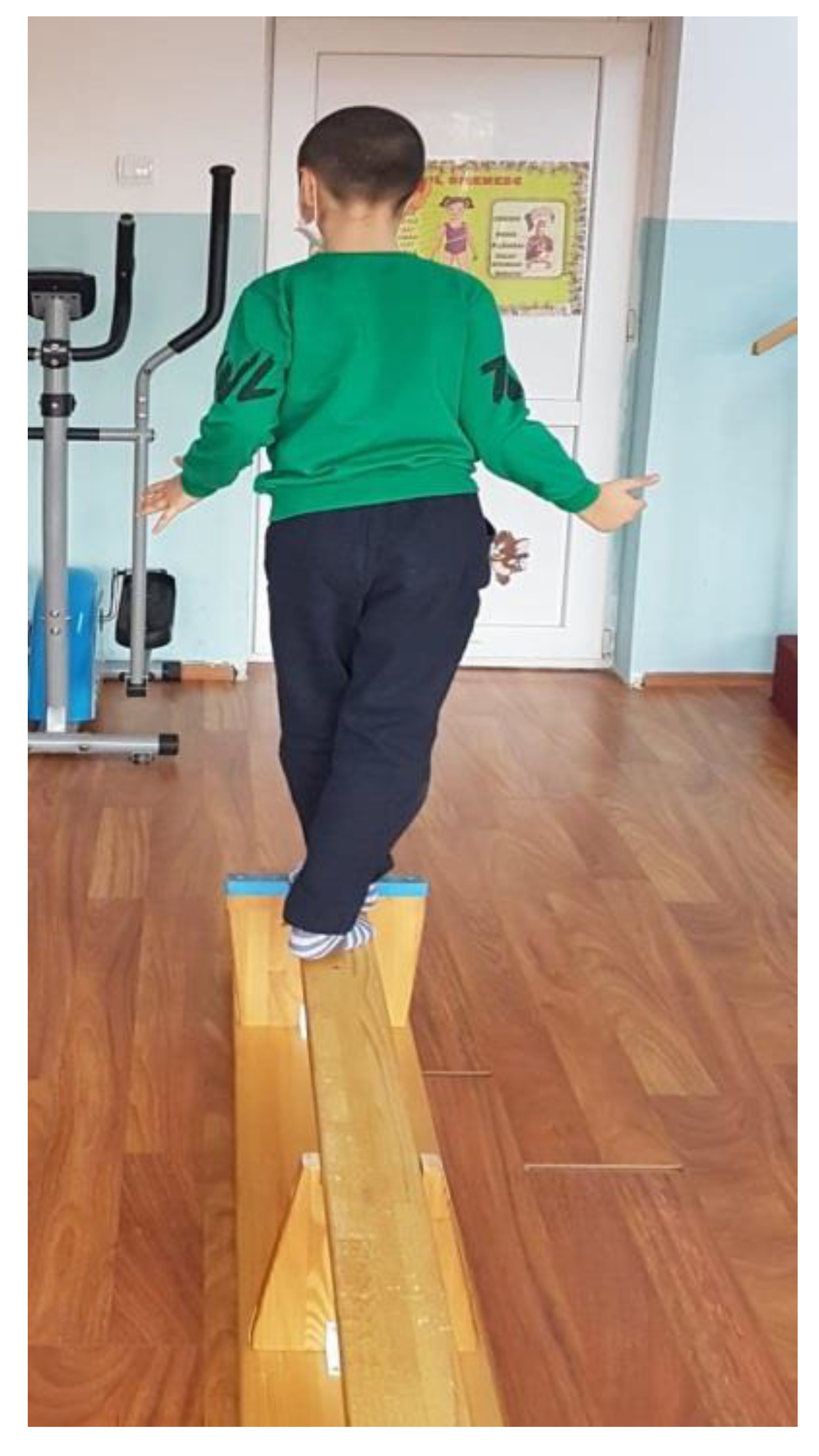
- Walking on a gymnastic bench, on the narrow side, as seen in Figure 3. (This exercise is useful for increasing the balance and coordination of the lower limbs; using the upper limbs to maintain balance means that we train those too.) We recommend that patients perform 4 repetitions of this exercise, 3 times per week.
- Standing on one leg, like a stork, for 10 s per leg (this exercise improves balance and coordination). We recommend that patients perform 6 repetitions of this exercise, 3 times per week.
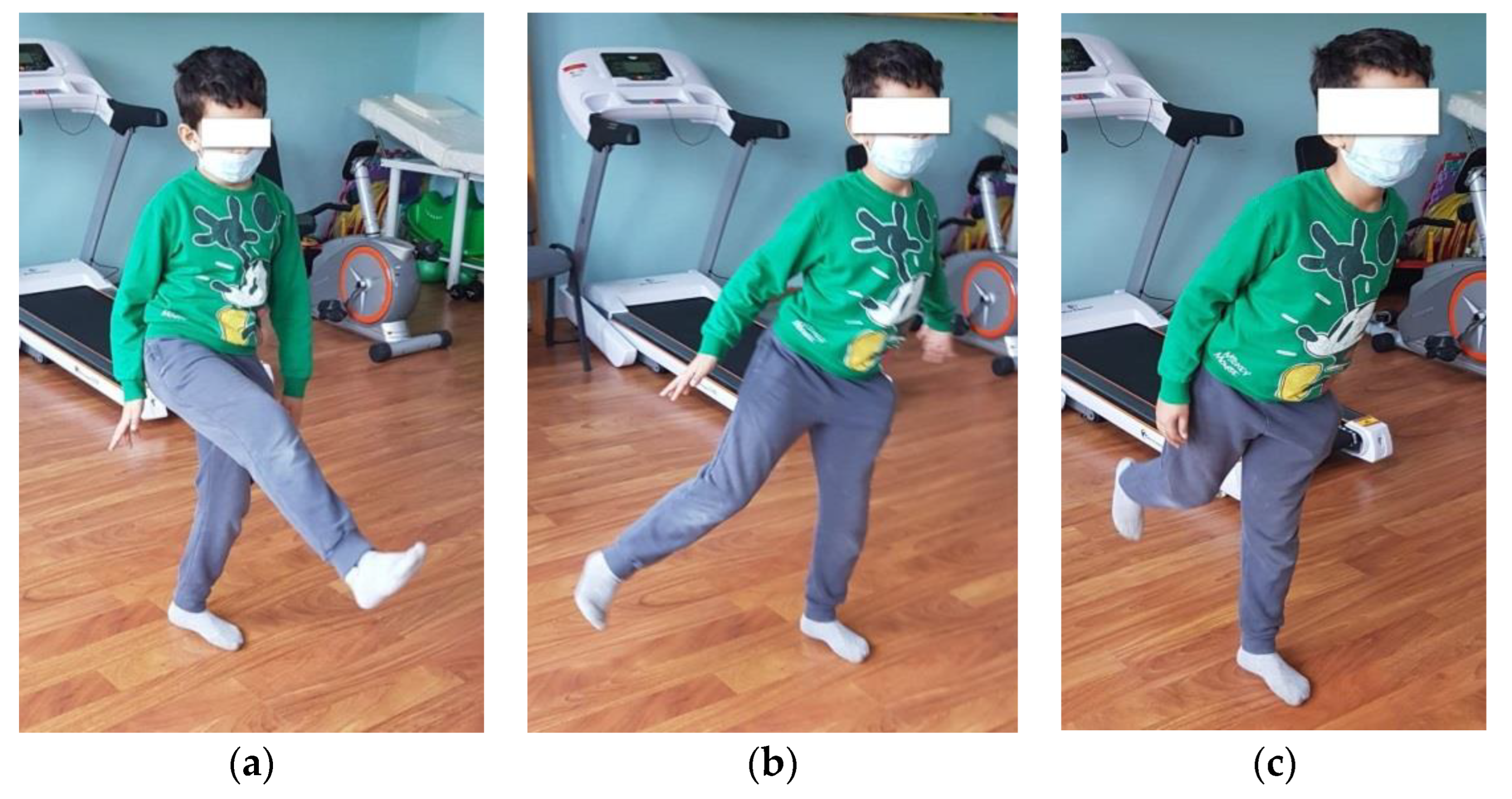
- Standing on one leg, with the other leg in front, lateral, and behind without touching the ground (Figure 4). (This exercise is good for increasing dynamic balance.) We recommend that patients perform 6 repetitions of this exercise, 3 times per week.
- Jumping from one leg to another while using circles on the ground to mark the place where the child must jump. (This exercise improves dynamic balance and coordination.) We recommend that patients perform 4 repetitions of this exercise, 3 times per week.
- Balance board exercises. First, we need to help the child and keep him or her balanced by placing the board near a parallel bar, where they can maintain their own balance. When the child is confident enough, he or she can release the support and stay on the board by themselves (as shown in Figure 5). This should be performed 3 times per week. (This exercise is useful for increasing balance.)
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hazlett, H.C.; Poe, M.D.; Gerig, G.; Styner, M.; Chappell, C.; Smith, R.G.; Vachet, C.; Piven, J. Early brain overgrowth in autism associated with an increase in cortical surface area before age 2 years. Arch. Gen. Psychiatry 2011, 68, 467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, C.A.; Morrow, E.M.; Rubenstein, J.L. Autism and brain development. Cell 2008, 135, 396–400. [Google Scholar] [CrossRef] [Green Version]
- Noura, A.; Koushik, M. Classification of Autism Spectrum Disorder From EEG-Based Functional Brain Connectivity Analysis. Neural Comput. 2021, 33, 1914–1941. [Google Scholar] [CrossRef]
- Courchesne, E.; Campbell, K.; Solso, S. Brain growth across the life span in autism: Age-specific changes in anatomical pathology. Brain Res. 2011, 1380, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirvikoski, T.; Mittendorfer-Rutz, E.; Boman, M.; Larsson, H.; Lichtenstein, P.; Bölte, S. Premature mortality in autism spectrum disorder. Br. J. Psychiatry J. Ment. Sci. 2016, 208, 232–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohane, I.S.; McMurry, A.; Weber, G.; MacFadden, D.; Rappaport, L.; Kunkel, L.; Bickel, J.; Wattanasin, N.; Spence, S.; Murphy, S.; et al. The co-morbidity burden of children and young adults with autism spectrum disorders. PLoS ONE 2012, 7, e33224. [Google Scholar] [CrossRef]
- Tye, B.W.; Commins, N.; Ryazanova, L.V.; Wühr, M.; Springer, M.; Pincus, D.; Churchman, L.S. Proteotoxicity from aberrant ribosome biogenesis compromises cell fitness. eLife 2019, 8, e43002. [Google Scholar] [CrossRef]
- Vorstman, J.; Parr, J.R.; Moreno-De-Luca, D.; Anney, R.; Nurnberger, J.I., Jr.; Hallmayer, J.F. Autism genetics: Opportunities and challenges for clinical translation. Nat. Rev. Genet. 2017, 18, 362–376. [Google Scholar] [CrossRef]
- Becker, E.B.; Stoodley, C.J. Autism spectrum disorder and the cerebellum. Int. Rev. Neurobiol. 2013, 113, 1–34. [Google Scholar] [CrossRef]
- Bruchhage, M.; Bucci, M.P.; Becker, E. Cerebellar involvement in autism and ADHD. Handb. Clin. Neurol. 2018, 155, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, M.W.; Sweeney, J.A. Sensorimotor dysfunctions as primary features of autism spectrum disorders. Sci. China Life Sci. 2015, 58, 1016–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacrey, L.A.; Zwaigenbaum, L.; Bryson, S.; Brian, J.; Smith, I.M.; Roberts, W.; Szatmari, P.; Roncadin, C.; Garon, N.; Novak, C.; et al. Can parents’ concerns predict autism spectrum disorder? A prospective study of high-risk siblings from 6 to 36 months of age. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.K.; Marini, M.; Lehr, S.A.; Cerruti, C.; Shin, J.E.; Joy-Gaba, J.A.; Ho, A.K.; Teachman, B.A.; Wojcik, S.P.; Koleva, S.P.; et al. Reducing implicit racial preferences: I. A comparative investigation of 17 interventions. J. Exp. Psychol. Gen. 2014, 143, 1765–1785. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.P.; Doyen, C.; Contenjean, Y.; Kaye, K. The effect of performing a dual task on postural control in children with autism. ISRN Neurosci. 2013, 2013, 796174. [Google Scholar] [CrossRef]
- Chen, M.H.; Lan, W.H.; Hsu, J.W.; Huang, K.L.; Su, T.P.; Li, C.T.; Lin, W.C.; Tsai, C.F.; Tsai, S.J.; Lee, Y.C.; et al. Risk of Developing Type 2 Diabetes in Adolescents and Young Adults with Autism Spectrum Disorder: A Nationwide Longitudinal Study. Diabetes Care 2016, 39, 788–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fournier, K.A.; Hass, C.J.; Naik, S.K.; Lodha, N.; Cauraugh, J.H. Motor coordination in autism spectrum disorders: A synthesis and meta-analysis. J. Autism Dev. Disord. 2010, 40, 1227–1240. [Google Scholar] [CrossRef] [PubMed]
- Memari, A.H.; Ghaheri, B.; Ziaee, V.; Kordi, R.; Hafizi, S.; Moshayedi, P. Physical activity in children and adolescents with autism assessed by triaxial accelerometry. Pediatric Obes. 2013, 8, 150–158. [Google Scholar] [CrossRef]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radonovich, K.J.; Fournier, K.A.; Hass, C.J. Relationship between postural control and restricted, repetitive behaviors in autism spectrum disorders. Front. Integr. Nneurosci. 2013, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Lacquaniti, F. Automatic control of limb movement and posture. Curr. Opin. Neurobiol. 1992, 2, 807–814. [Google Scholar] [CrossRef]
- Massion, J. Postural control systems in developmental perspective. Neurosci. Biobehav. Rev. 1998, 22, 465–472. [Google Scholar] [CrossRef]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Tureck, K.; Schneiderman, R.L. Autism and exergaming: Effects on repetitive behaviors and cognition. Psychol. Res. Behav. Manag. 2011, 4, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Chen, S. The Effects of Structured Physical Activity Program on Social Interaction and Communication for Children with Autism. BioMed Res. Int. 2018, 1825046. [Google Scholar] [CrossRef]
- Arzoglou, D.; Tsimaras, V.; Kotsikas, G.; Fotiadou, E.; Sidiropoulou, M.; Proios, M.; Bassa, E. The effect of a traditional dance training program on neuromuscular coordination of individuals with autism. J. Phys. Educ. Sport 2013, 13, 563–569. [Google Scholar] [CrossRef]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic review with meta-analysis: The worldwide prevalence of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Lochbaum, M.; Crews, D. Viability of Cardiorespiratory and Muscular Strength Programs for the Adolescent with Autism. J. Evid. Based Integr. Med. 2003, 8, 225–233. [Google Scholar] [CrossRef]
- Pan, Y.; Chen, W.; Xu, Y.; Yi, X.; Han, Y.; Yang, Q.; Li, X.; Huang, L.; Johnston, S.C.; Zhao, X.; et al. Genetic Polymorphisms and Clopidogrel Efficacy for Acute Ischemic Stroke or Transient Ischemic Attack: A Systematic Review and Meta-Analysis. Circulation 2017, 135, 21–33. [Google Scholar] [CrossRef]
- Gouleme, N.; Scheid, I.; Peyre, H.; Seassau, M.; Maruani, A.; Clarke, J.; Delorme, R.; Bucci, M.P. Postural Control and Emotion in Children with Autism Spectrum Disorders. Transl. Neurosci. 2017, 8, 158–166. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Leventhal, B.L.; Koh, Y.J.; Fombonne, E.; Laska, E.; Lim, E.C.; Cheon, K.-A.; Kim, S.-J.; Kim, Y.-K.; Lee, H.; et al. Prevalence of autism spectrum disorders in a total population sample. Am. J. Psychiatry 2011, 168, 904–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheldavi, H.; Shakerian, S.; Nahid, S.; Boshehri, S.; Zarghami, M. The effects of balance training intervention on postural control of children with autism spectrum disorder: Role of sensory information. Res. Autism Spectr. Disord. 2014, 8, 8–14. [Google Scholar] [CrossRef]
- Travers, B.G.; Mason, A.H.; Mrotek, L.; Ellertson, A.; Dean, D.C.; Engel, C.; Gomez, A.; Dadalko, O.I.; McLaughlin, K. Biofeedback-based, videogame balance training in autism. J. Autism Dev. Disord. 2017, 48, 163–175. [Google Scholar] [CrossRef]
- Jabouille, F.; Billot, M.; Hermand, E.; Lemonnier, E.; Perrochon, A. Balance rehabilitation for postural control in children with Autism Spectrum Disorder: A two-case report study. Physiother. Theory Pract. 2021. [Google Scholar] [CrossRef] [PubMed]
- Caldani, S.; Atzori, P.; Peyre, H.; Delorme, R.; Bucci, M.P. Short rehabilitation training program may improve postural control in children with autism spectrum disorders: Preliminary evidences. Sci. Rep. 2020, 10, 7917. [Google Scholar] [CrossRef] [PubMed]
- Abdel Ghafar, M.A.; Abdelraouf, O.R.; Abdelgalil, A.A.; Seyam, M.K.; Radwan, R.E.; El-Bagalaty, A.E. Quantitative Assessment of Sensory Integration and Balance in Children with Autism Spectrum Disorders: Cross-Sectional Study. Children 2022, 9, 353. [Google Scholar] [CrossRef]
- Gong, X.; Li, X.; Wang, Q.; Hoi, S.P.; Yin, T.; Zhao, L.; Meng, F.; Luo, X.; Liu, J. Comparing visual preferences between autism spectrum disorder (ASD) and normal children to explore the characteristics of visual preference of Children with ASD by improved visual preference paradigm: A case-control study. Transl. Pediatr. 2021, 10, 2006–2015. [Google Scholar] [CrossRef]
- Moseley, R.L.; Pulvermüller, F. What can autism teach us about the role of sensorimotor systems in higher cognition? New clues from studies on language, action semantics, and abstract emotional concept processing. Cortex 2018, 100, 149–190. [Google Scholar] [CrossRef]
- Brehmer, Y.; Li, S.C.; Müller, V.; von Oertzen, T.; Lindenberger, U. Memory plasticity across the life span: Uncovering children’s latent potential. Dev. Psychol. 2007, 43, 465–478. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.; Partridge, K.; Girdler, S.; Morris, S.L. Standing postural control in individuals with autism spectrum disorder: Systematic review and meta-analysis. J. Autism Dev. Disord. 2017, 47, 2238–2253. [Google Scholar] [CrossRef]
- Smoot Reinert, S.; Jackson, K.; Bigelow, K. Using posturography to examine the immediate effects of vestibular therapy for children with autism spectrum disorders: A feasibility study. Phys. Occup. Ther. Pediatr. 2015, 35, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Doumas, M.; McKenna, R.; Murphy, B. Postural control deficits in autism spectrum disorder: The role of sensory integration. J. Autism Dev. Disord. 2016, 46, 853–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.L.; Foster, C.J.; Parsons, R.; Falkmer, M.; Falkmer, T.; Rosalie, S.M. Differences in the use of vision and proprioception for postural control in autism spectrum disorder. Neuroscience 2015, 307 (Suppl. C), 273–280. Available online: http://www.sciencedirect.com/science/article/pii/S0306452215007721 (accessed on 23 June 2022). [CrossRef] [PubMed]
- Memari, A.H.; Ghanouni, P.; Gharibzadeh, S.; Eghlidi, J.; Ziaee, V.; Moshayedi, P. Postural sway patterns in children with autism spectrum disorder compared with typically developing children. Res. Autism Spectr. Disord. 2013, 7, 325–332. Available online: http://www.sciencedirect.com/science/article/pii/S1750946712001183. (accessed on 23 June 2022). [CrossRef]
- Li, Y.; Mache, M.A.; Todd, T.A. Complexity of center of pressure in postural control for children with autism spectrum disorders was partially compromised. J. Appl. Biomech. 2019, 35, 190–195. Available online: https://journals.humankinetics.com/view/journals/jab/35/3/article-p190.xml. (accessed on 23 June 2022). [CrossRef] [PubMed]
- Laurenco, C.; Esteves, D.; Corredeira, R.; Seabra, A. The effect of a trampoline-based training program on the muscle strength of the inferior limbs and motor proficiency in children with autism spectrum disorders. J. Phys. Educ. Sport. 2015, 15, 592. [Google Scholar] [CrossRef]
- Najafabadi, M.G.; Sheikh, M.; Hemayattalab, R.; Memari, A.H.; Aderyani, M.R.; Hafizi, S. The Effect of SPARK on Social and Motor Skills of Children with Autism. Pediatr. Neonatol. 2018, 59, 481–487. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject No | Weight (kg) | Height (cm) | Gender | Level of Disability According to the Social Assistance Criteria |
|---|---|---|---|---|
| S1 | 37 | 134 | F | Mild |
| S2 | 27 | 124 | M | Mild |
| S3 | 36 | 134 | M | Mild |
| S4 | 18 | 126 | F | Mild |
| S5 | 22 | 125 | M | Mild |
| S6 | 44 | 147 | F | Mild |
| S7 | 44 | 138 | M | Mild |
| S8 | 38 | 145 | F | Mild |
| S9 | 25 | 128 | M | Mild |
| S10 | 35 | 136 | M | Mild |
| S11 | 20 | 137 | M | Mild |
| S12 | 23 | 128 | M | Mild |
| S13 | 45 | 150 | F | Mild |
| S14 | 42 | 136 | M | Mild |
| S15 | 40 | 140 | F | Mild |
| S16 | 26 | 129 | M | Mild |
| S17 | 37 | 136 | M | Mild |
| S18 | 21 | 128 | M | Mild |
| S19 | 24 | 124 | M | Mild |
| S20 | 47 | 149 | M | Mild |
| S21 | 41 | 151 | M | Mild |
| S22 | 30 | 147 | F | Mild |
| S23 | 26 | 132 | M | Mild |
| S24 | 34 | 150 | M | Mild |
| S25 | 17 | 135 | M | Mild |
| S26 | 20 | 152 | M | Mild |
| S27 | 43 | 142 | F | Mild |
| S28 | 39 | 129 | M | Mild |
| Subjects | Weight (Kg) | The Surface of the Confidence Ellipse A (mm2) | The Length of the Curve (Lc) Described by COP (mm) | Coefficient Lc/A |
|---|---|---|---|---|
| S1 | 37 | 326 | 787 | 2.41 |
| S2 | 27 | 357 | 525 | 1.47 |
| S3 | 36 | 1489 | 407 | 0.27 |
| S4 | 18 | 1437 | 900 | 0.63 |
| S5 | 22 | 2935 | 1144 | 0.12 |
| S6 | 44 | 30 | 480 | 16.16 |
| S7 | 44 | 30 | 297 | 10.05 |
| S8 | 38 | 328 | 788 | 2.40 |
| S9 | 25 | 356 | 527 | 1.48 |
| S10 | 35 | 1490 | 410 | 0.28 |
| S11 | 20 | 1440 | 910 | 0.63 |
| S12 | 23 | 2740 | 1150 | 0.12 |
| S13 | 45 | 30 | 481 | 16.03 |
| S14 | 42 | 29 | 300 | 10.34 |
| S15 | 40 | 322 | 780 | 2.42 |
| S16 | 26 | 353 | 520 | 1.47 |
| S17 | 37 | 1480 | 417 | 0.28 |
| S18 | 21 | 1430 | 912 | 0.64 |
| S19 | 24 | 2816 | 1104 | 0.11 |
| S20 | 47 | 30 | 470 | 15.77 |
| S21 | 41 | 27 | 279 | 10.51 |
| S22 | 30 | 336 | 786 | 2.34 |
| S23 | 26 | 367 | 523 | 1.43 |
| S24 | 34 | 1469 | 415 | 0.28 |
| S25 | 17 | 1487 | 900 | 0.61 |
| S26 | 20 | 2773 | 1094 | 0.11 |
| S27 | 43 | 32 | 460 | 14.51 |
| S28 | 39 | 28 | 279 | 10.13 |
| Weight (Kg) | The Surface of the Confidence Ellipse A (mm2) | The Length of the Curve (Lc) Described by COP (mm) | Coefficient Lc/A | |
|---|---|---|---|---|
| Minimum | 17 | 26.55 | 279 | 0.11 |
| Maximum | 47 | 2935 | 1150 | 16.16 |
| Mean | 32.18 | 927.32 | 644.44 | 4.39 |
| Standard deviation | 9.50 | 977.42 | 283.43 | 5.75 |
| Subjects | Weight (Kg) | The Surface of the Confidence Ellipse A (mm2) | The Length of the Curve (Lc) Described by COP (mm) | Coefficient Lc/A |
|---|---|---|---|---|
| S1 | 38 | 18 | 398 | 22.16 |
| S2 | 28 | 3 | 268 | 89.77 |
| S3 | 38 | 125 | 385 | 3.06 |
| S4 | 21 | 37 | 274 | 7.33 |
| S5 | 24 | 246 | 620 | 2.52 |
| S6 | 43 | 18 | 351 | 19.25 |
| S7 | 46 | 21 | 344 | 16.18 |
| S8 | 33 | 20 | 391 | 19.58 |
| S9 | 30 | 5 | 277 | 56.65 |
| S10 | 40 | 127 | 384 | 3.01 |
| S11 | 23 | 38 | 269 | 7.15 |
| S12 | 28 | 240 | 617 | 2.57 |
| S13 | 46 | 19 | 341 | 17.67 |
| S14 | 42 | 19 | 334 | 17.34 |
| S15 | 32 | 18 | 388 | 21.60 |
| S16 | 25 | 4 | 277 | 75.22 |
| S17 | 35 | 135 | 389 | 2.87 |
| S18 | 26 | 35 | 249 | 7.04 |
| S19 | 27 | 236 | 618 | 2.62 |
| S20 | 43 | 18 | 349 | 19.25 |
| S21 | 45 | 27 | 350 | 12.83 |
| S22 | 39 | 17 | 388 | 22.87 |
| S23 | 29 | 3 | 269 | 99.67 |
| S24 | 34 | 129 | 371 | 2.88 |
| S25 | 18 | 36 | 280 | 7.70 |
| S26 | 22 | 264 | 613 | 2.32 |
| S27 | 36 | 19 | 353 | 18.38 |
| S28 | 37 | 22 | 349 | 16.04 |
| Weight (Kg) | The Surface of the Confidence Ellipse A (mm2) | The Length of the Curve (L) Described by COP (mm) | Coefficient Lc/A | |
|---|---|---|---|---|
| Minimum | 18 | 2.70 | 249 | 2.32 |
| Maximum | 46 | 264 | 619.50 | 99.67 |
| Mean | 33.14 | 67.91 | 374.67 | 21.27 |
| Standard deviation | 8.22 | 84.23 | 110.66 | 26.32 |
| The Surface of the Confidence Ellipse | The Length of the Curve Described by the COP | Coefficient Lc/A | |
|---|---|---|---|
| p values (results of Student’s t test) | 0.004 | 0.000 | 0.0016 |
| Cohen’s D test | 0.8 | 1.25 | −0.9 |
| Variables | EV2 Weight | EV2 The Surface of the Confidence Ellipse | EV2 The Length of the Curve Described by the COP | EV2 Coefficient Lc/A |
|---|---|---|---|---|
| EV1 Weight | 0.918 | −0.374 | −0.128 | −0.079 |
| EV1 The surface of the confidence ellipse | −0.620 | 0.911 | 0.693 | −0.456 |
| EV1 The length of the curve described by the COP | −0.721 | 0.548 | 0.549 | −0.258 |
| Variables | EV2 Weight | EV2 The Surface of the Confidence Ellipse | EV2 The Length of the Curve Described by the COP | EV2 Coefficient Lc/A |
|---|---|---|---|---|
| EV1 Weight | 0.903 | −0.374 | 0.094 | 0.352 |
| EV1 The surface of the confidence ellipse | −0.673 | 0.637 | 0.321 | −0.616 |
| EV1 The length of the curve described by the COP | −0.746 | 0.246 | 0.199 | −0.215 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roșca, A.M.; Rusu, L.; Marin, M.I.; Ene Voiculescu, V.; Ene Voiculescu, C. Physical Activity Design for Balance Rehabilitation in Children with Autism Spectrum Disorder. Children 2022, 9, 1152. https://doi.org/10.3390/children9081152
Roșca AM, Rusu L, Marin MI, Ene Voiculescu V, Ene Voiculescu C. Physical Activity Design for Balance Rehabilitation in Children with Autism Spectrum Disorder. Children. 2022; 9(8):1152. https://doi.org/10.3390/children9081152
Chicago/Turabian StyleRoșca, Andreea Maria, Ligia Rusu, Mihnea Ion Marin, Virgil Ene Voiculescu, and Carmen Ene Voiculescu. 2022. "Physical Activity Design for Balance Rehabilitation in Children with Autism Spectrum Disorder" Children 9, no. 8: 1152. https://doi.org/10.3390/children9081152
APA StyleRoșca, A. M., Rusu, L., Marin, M. I., Ene Voiculescu, V., & Ene Voiculescu, C. (2022). Physical Activity Design for Balance Rehabilitation in Children with Autism Spectrum Disorder. Children, 9(8), 1152. https://doi.org/10.3390/children9081152