
Craniofacial Morphologic Predictors for Passive Myofunctional Therapy of Pediatric Obstructive Sleep Apnea Using an Oral Appliance with a Tongue Bead


 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
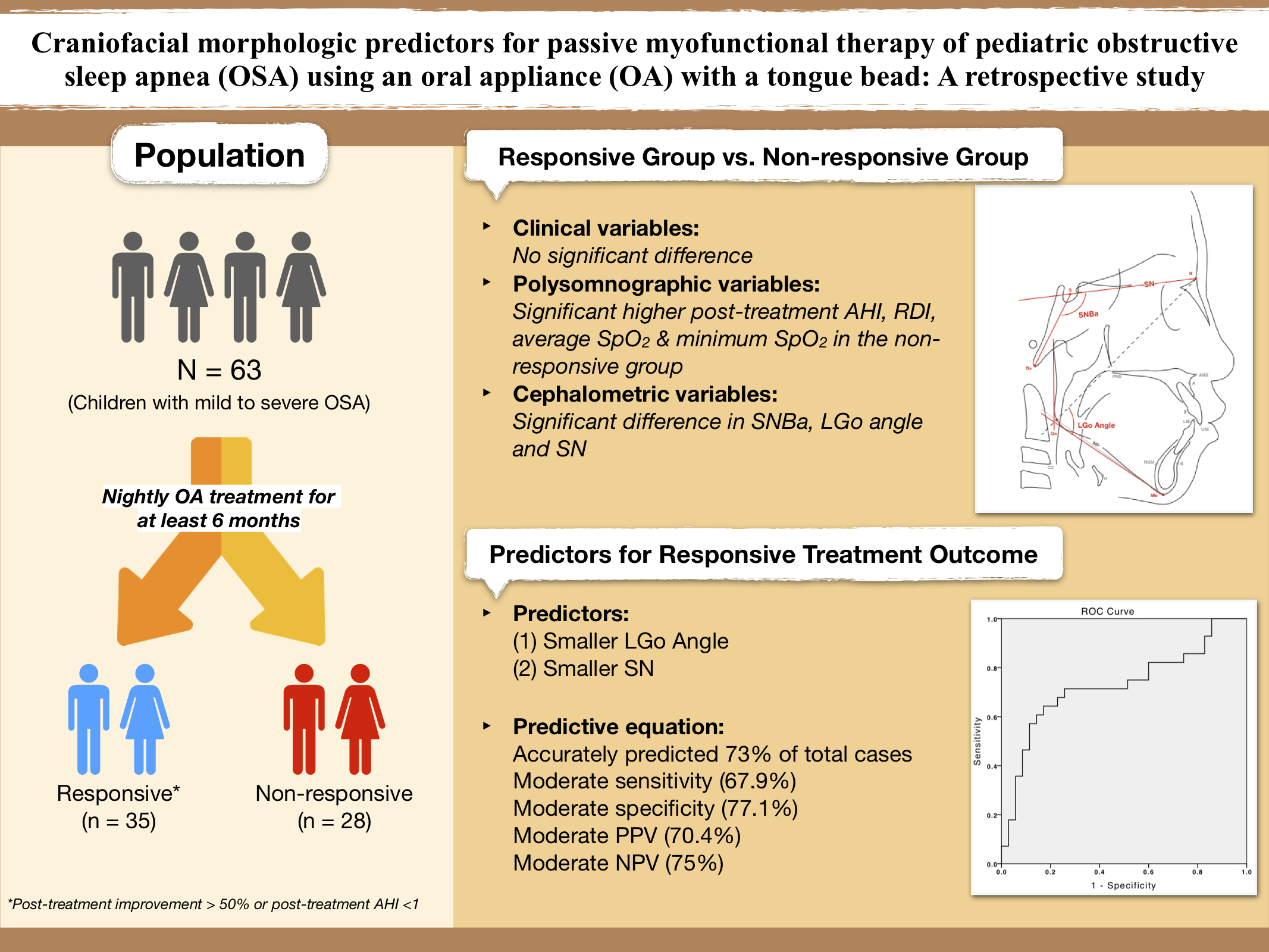
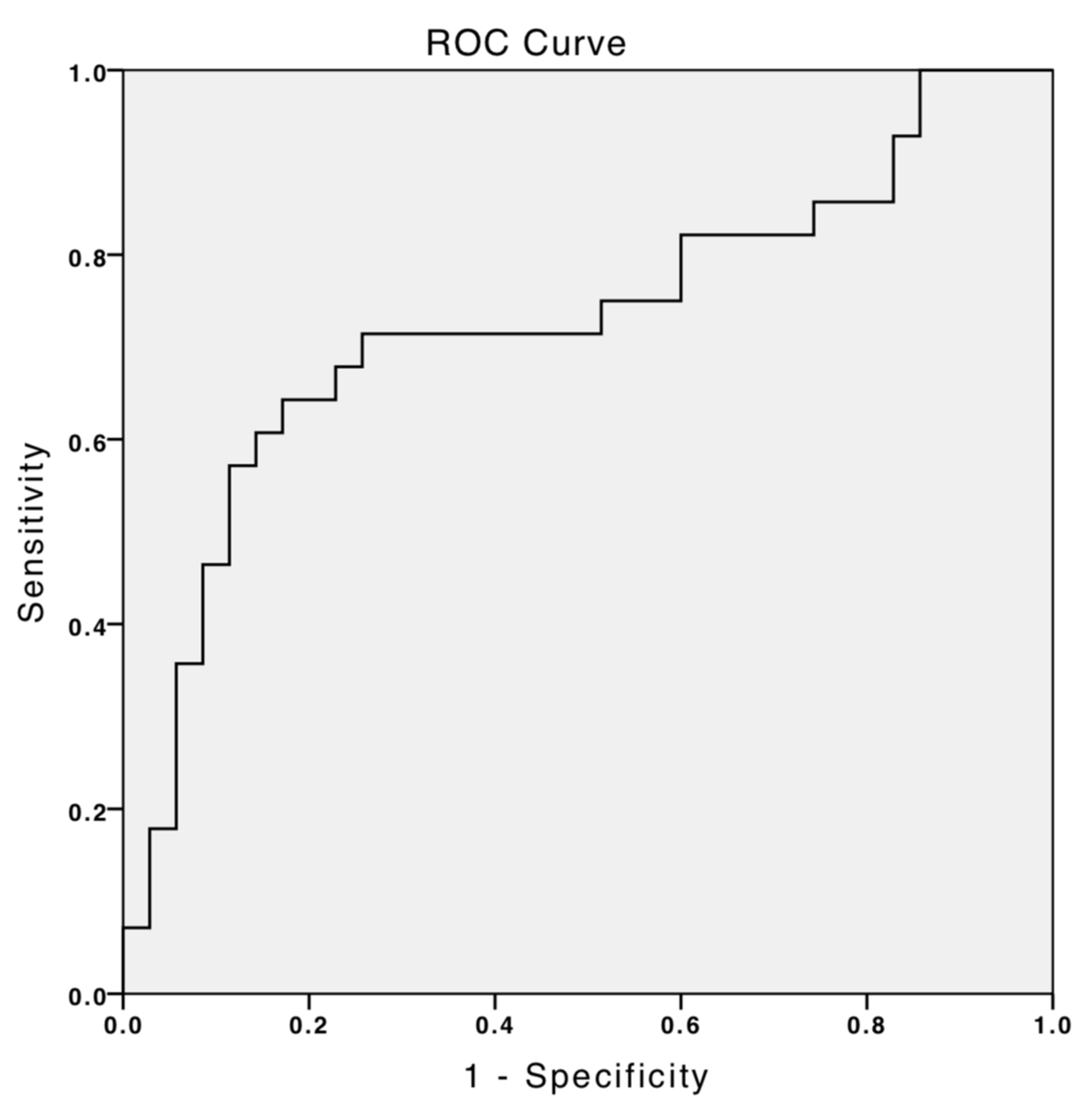
2.1. Participants
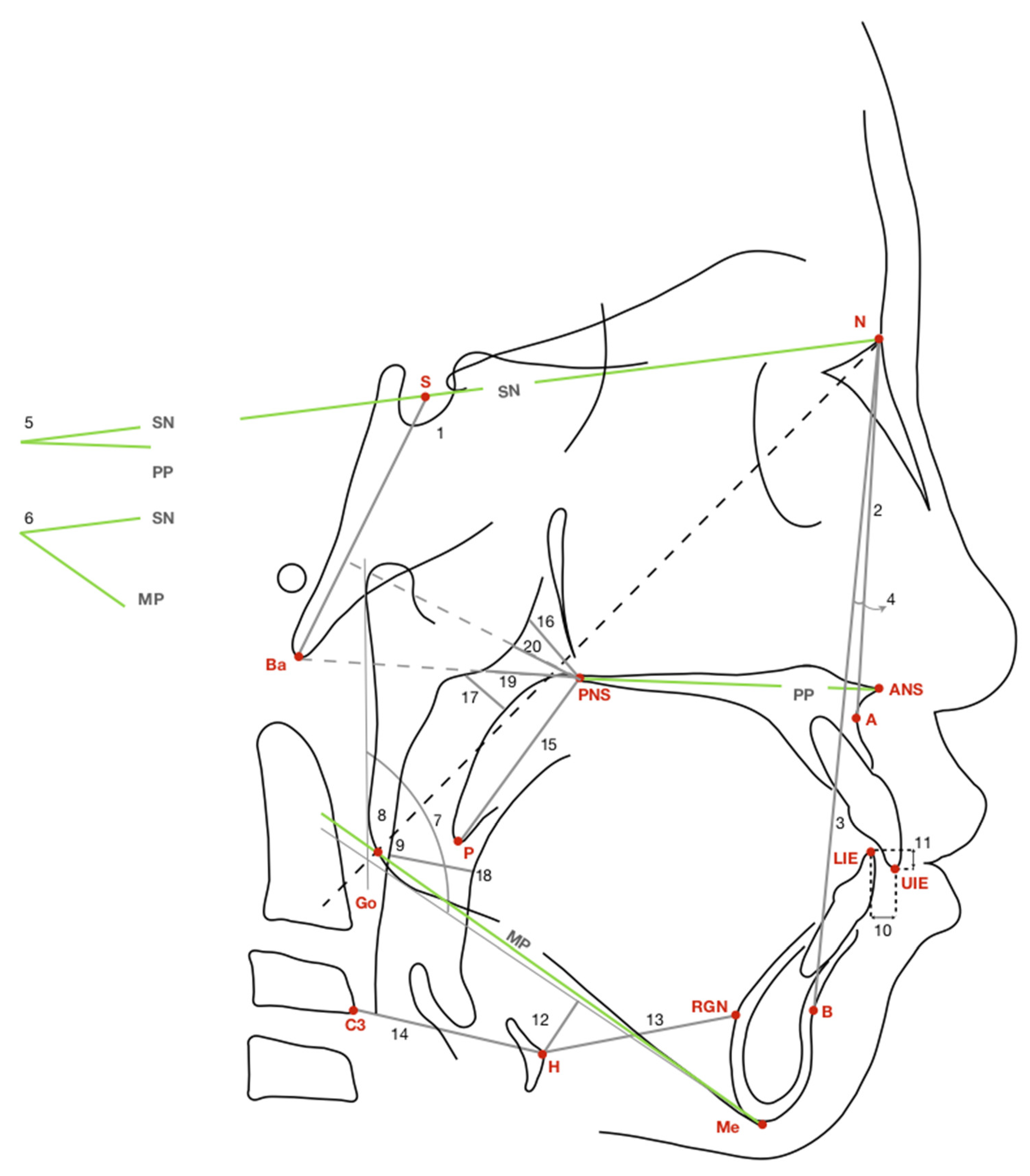
2.2. Lateral Cephalometric Radiography
2.3. Oral Appliance with a Built-In Tongue Bead
3. Statistical Analyses
4. Results
4.1. Descriptive Statistics
4.2. Cephalometric Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guilleminault, C.; Stoohs, R. Chronic snoring and obstructive sleep apnea syndrome in children. Lung 1990, 168, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Section on Pediatric Pulmonology; Subcommittee on Obstructive Sleep Apnea Syndrome; American Academy of Pediatrics. Clinical practice guideline: Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002, 109, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Sheldon, S.H.; Spruyt, K.; Ward, S.D.; et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, 576–584. [Google Scholar] [CrossRef]
- Katz, E.S.; D’Ambrosio, C.M. Pathophysiology of pediatric obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 253–262. [Google Scholar] [CrossRef]
- Capua, M.; Ahmadi, N.; Shapiro, C. Overview of obstructive sleep apnea in children: Exploring the role of dentists in diagnosis and treatment. J. Can. Dent. Assoc. 2009, 75, 285–289. [Google Scholar]
- Bahammam, A. Obstructive sleep apnea: From simple upper airway obstruction to systemic inflammation. Ann. Saudi Med. 2011, 31, 1–2. [Google Scholar] [CrossRef][Green Version]
- Lal, C.; Strange, C.; Bachman, D. Neurocognitive impairment in obstructive sleep apnea. Chest 2012, 141, 1601–1610. [Google Scholar] [CrossRef]
- Brunetti, L.; Rana, S.; Lospalluti, M.L.; Pietrafesa, A.; Francavilla, R.; Fanelli, M.; Armenio, L. Prevalence of obstructive sleep apnea syndrome in a cohort of 1207 children of southern Italy. Chest 2001, 120, 1930–1935. [Google Scholar] [CrossRef]
- Rosen, C.L.; Larkin, E.K.; Kirchner, H.L.; Emancipator, J.L.; Bivins, S.F.; Surovec, S.A.; Martin, R.J.; Redline, S. Prevalence and risk factors for sleep-disordered breathing in 8- to 11-year-old children: Association with race and prematurity. J. Pediatr. 2003, 142, 383–389. [Google Scholar] [CrossRef]
- Rosen, C.L.; Storfer-Isser, A.; Taylor, H.G.; Kirchner, H.L.; Emancipator, J.L.; Redline, S. Increased behavioral morbidity in school-aged children with sleep-disordered breathing. Pediatrics 2004, 114, 1640–1648. [Google Scholar] [CrossRef]
- Sogut, A.; Altin, R.; Uzun, L.; Ugur, M.B.; Tomac, N.; Acun, C.; Kart, L.; Can, G. Prevalence of obstructive sleep apnea syndrome and associated symptoms in 3–11-year-old Turkish children. Pediatr. Pulmonol. 2005, 39, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, J.C.; Chervin, R.D. Epidemiology of pediatric obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Liao, D.; Calhoun, S.; Vela-Bueno, A.; Fedok, F.; Vlasic, V.; Graff, G. Sleep disordered breathing in children in a general population sample: Prevalence and risk factors. Sleep 2009, 32, 731–736. [Google Scholar] [CrossRef]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; de Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int. J. Environ. Res. Public Health 2019, 16, 3235. [Google Scholar] [CrossRef] [PubMed]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef]
- Dehlink, E.; Tan, H.L. Update on paediatric obstructive sleep apnoea. J. Thorac. Dis. 2016, 8, 224–235. [Google Scholar] [CrossRef]
- Brockbank, J.C. Update on pathophysiology and treatment of childhood obstructive sleep apnea syndrome. Paediatr. Respir. Rev. 2017, 24, 21–23. [Google Scholar] [CrossRef]
- Schmidt-Nowara, W.; Lowe, A.; Wiegand, L.; Cartwright, R.; Perez-Guerra, F.; Menn, S. Oral appliances for the treatment of snoring and obstructive sleep apnea: A review. Sleep 1995, 18, 501–510. [Google Scholar] [CrossRef]
- Villa, M.P.; Bernkopf, E.; Pagani, J.; Broia, V.; Montesano, M.; Ronchetti, R. Randomized controlled study of an oral jaw-positioning appliance for the treatment of obstructive sleep apnea in children with malocclusion. Am. J. Respir. Crit. Care Med. 2002, 165, 123–127. [Google Scholar] [CrossRef]
- Ferguson, K.A.; Cartwright, R.; Rogers, R.; Schmidt-Nowara, W. Oral appliances for snoring and obstructive sleep apnea: A review. Sleep 2006, 29, 244–262. [Google Scholar] [CrossRef]
- Doff, M.H.; Hoekema, A.; Wijkstra, P.J.; van der Hoeven, J.H.; Huddleston Slater, J.J.; de Bont, L.G.; Stegenga, B. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: A 2-year follow-up. Sleep 2013, 36, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Cistulli, P.A.; Gotsopoulos, H.; Marklund, M.; Lowe, A.A. Treatment of snoring and obstructive sleep apnea with mandibular repositioning appliances. Sleep Med. Rev. 2004, 8, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Holley, A.B.; Lettieri, C.J.; Shah, A.A. Efficacy of an adjustable oral appliance and comparison with continuous positive airway pressure for the treatment of obstructive sleep apnea syndrome. Chest 2011, 140, 1511–1516. [Google Scholar] [CrossRef]
- Ferguson, K.A.; Ono, T.; Lowe, A.A.; al-Majed, S.; Love, L.L.; Fleetham, J.A. A short-term controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnoea. Thorax 1997, 52, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Pancer, J.; Al-Faifi, S.; Al-Faifi, M.; Hoffstein, V. Evaluation of variable mandibular advancement appliance for treatment of snoring and sleep apnea. Chest 1999, 116, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Qian, J.; Petocz, P.; Darendeliler, M.A.; Cistulli, P.A. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2001, 163, 1457–1461. [Google Scholar] [CrossRef] [PubMed]
- Machado-Junior, A.J.; Signorelli, L.G.; Zancanella, E.; Crespo, A.N. Randomized controlled study of a mandibular advancement appliance for the treatment of obstructive sleep apnea in children: A pilot study. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e403–e407. [Google Scholar] [CrossRef]
- Idris, G.; Galland, B.; Robertson, C.J.; Gray, A.; Farella, M. Mandibular advancement appliances for sleep-disordered breathing in children: A randomized crossover clinical trial. J. Dent. 2018, 71, 9–17. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Korayem, M.; Heo, G.; Witmans, M.; Major, M.P.; Major, P.W. Craniofacial morphological characteristics in children with obstructive sleep apnea syndrome: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2013, 144, 269–277. [Google Scholar] [CrossRef]
- Eveloff, S.E.; Rosenberg, C.L.; Carlisle, C.C.; Millman, R.P. Efficacy of a Herbst mandibular advancement device in obstructive sleep apnea. Am. J. Respir. Crit Care Med. 1994, 149, 905–909. [Google Scholar] [CrossRef]
- Mayer, G.; Meier-Ewert, K. Cephalometric predictors for orthopaedic mandibular advancement in obstructive sleep apnoea. Eur. J. Orthod. 1995, 17, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Lowe, A.A.; Fleetham, J.A.; Park, Y.C. Cephalometric and physiologic predictors of the efficacy of an adjustable oral appliance for treating obstructive sleep apnea. Am. J. Orthod. Dentofacial Orthop. 2001, 120, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Mataki, S.; Kurosaki, N. Cephalometric evaluation of craniofacial and upper airway structures in Japanese patients with obstructive sleep apnea. J. Med. Dent. Sci 2003, 50, 109–120. [Google Scholar] [PubMed]
- Marklund, M.; Stenlund, H.; Franklin, K.A. Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: Tolerability and predictors of treatment success. Chest 2004, 125, 1270–1278. [Google Scholar] [CrossRef]
- Otsuka, R.; Almeida, F.R.; Lowe, A.A.; Ryan, F. A comparison of responders and nonresponders to oral appliance therapy for the treatment of obstructive sleep apnea. Am. J. Orthod Dentofac. Orthop. 2006, 129, 222–229. [Google Scholar] [CrossRef]
- Hoekema, A.; Doff, M.H.; de Bont, L.G.; van der Hoeven, J.H.; Wijkstra, P.J.; Pasma, H.R.; Stegenga, B. Predictors of obstructive sleep apnea-hypopnea treatment outcome. J. Dent. Res. 2007, 86, 1181–1186. [Google Scholar] [CrossRef]
- Shen, H.L.; Wen, Y.W.; Chen, N.H.; Liao, Y.F. Craniofacial morphologic predictors of oral appliance outcomes in patients with obstructive sleep apnea. J. Am. Dent. Assoc. 2012, 143, 1209–1217. [Google Scholar] [CrossRef]
- Chuang, L.C.; Lian, Y.C.; Hervy-Auboiron, M.; Guilleminault, C.; Huang, Y.S. Passive myofunctional therapy applied on children with obstructive sleep apnea: A 6-month follow-up. J. Formos. Med. Assoc. 2017, 116, 536–541. [Google Scholar] [CrossRef]
- Huang, Y.S.; Chuang, L.C.; Hervy-Auboiron, M.; Paiva, T.; Lin, C.H.; Guilleminault, C. Neutral supporting mandibular advancement device with tongue bead for passive myofunctional therapy: A long term follow-up study. Sleep Med. 2019, 60, 69–74. [Google Scholar] [CrossRef]
- Chin, A.; Perry, S.; Liao, C.; Yang, Y. The relationship between the cranial base and jaw base in a Chinese population. Head Face Med. 2014, 10, 1–8. [Google Scholar] [CrossRef]
- Battagel, J.M.; Johal, A.; L’Estrange, P.R.; Croft, C.B.; Kotecha, B. Changes in airway and hyoid position in response to mandibular protrusion in subjects with obstructive sleep apnoea (OSA). Eur. J. Orthod. 1999, 21, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Influence of sleep posture on response to oral appliance therapy for sleep apnea syndrome. Sleep 2001, 24, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Casale, M.; Pappacena, M.; Rinaldi, V.; Bressi, F.; Baptista, P.; Salvinelli, F. Obstructive sleep apnea syndrome: From phenotype to genetic basis. Curr. Genom. 2009, 10, 119–126. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Responsive Group (N = 28) | Non-Responsive Group (N = 35) | Total (N = 63) | p | |
|---|---|---|---|---|
| Sex, no. (%) | ||||
| Male | 21 (33.3%) | 29 (46.1%) | 50 (79.4%) | 0.444 a |
| Female | 7 (11.1%) | 6 (9.5%) | 13 (20.6%) | |
| Age (years) | 8.14 ± 3.45 | 9.23 ± 3.03 | 8.75 ± 3.24 | 0.140 b |
| Birth weight (gm) | 2692.32 ± 804.59 | 2931.4 ± 781.70 | 2825.14 ± 794.58 | 0.368 b |
| Gestational age (week) | 36.39 ± 3.77 | 37.77 ± 3.00 | 37.16 ± 3.40 | 0.119 b |
| Birth, no. (%) | ||||
| Full-term | 16 (25.4%) | 25 (39.7%) | 41 (65.1%) | 0.237 a |
| Preterm | 12 (19%) | 10 (15.9%) | 22 (34.9%) | |
| BMI | 17.90 ± 4.42 | 19.39 ± 5.18 | 18.72 ± 4.88 | 0.240 b |
| Body height (cm) | 125.68 ± 22.42 | 129.28 ± 29.28 | 127.68 ± 26.31 | 0.265 b |
| Pre-treatment OSA severity, no. (%) | ||||
| Mild (1 ≤ AHI < 5) | 17 (27.0%) | 25 (39.7%) | 42 (66.7%) | 0.546 a |
| Moderate (5 ≤ AHI < 10) | 9 (14.3%) | 7 (11.1%) | 16 (25.4%) | |
| Severe (AHI ≥ 10) | 2 (3.2%) | 3 (4.8%) | 5 (7.9%) | |
| Pretreatment PSG data | ||||
| AHI (No./h) | 4.79 ± 3.39 | 4.41 ± 4.03 | 4.58 ± 3.73 | 0.575 b |
| RDI (No./h) | 7.46 ± 5.89 | 6.59 ± 5.01 | 6.98 ± 5.39 | 0.534 b |
| Mean SpO2 (%) | 97.27 ± 0.87 | 97.57 ± 0.65 | 97.44 ± 0.76 | 0.088 b |
| Average SpO2 (%) | 96.46 ± 2.62 | 97.11 ± 0.83 | 96.83 ± 1.87 | 0.601 b |
| Minimum SpO2 (%) | 89.61 ± 4.25 | 89.94 ± 3.80 | 89.79 ± 3.97 | 0.994 b |
| Post-treatment PSG data | ||||
| AHI (No./h) | 1.42 ± 1.25 | 5.66 ± 4.99 | 3.78 ± 4.34 | 0.000 *,b |
| RDI (No./h) | 4.47 ± 4.77 | 6.59 ± 5.34 | 5.65 ± 5.16 | 0.007 *,b |
| Mean SpO2 (%) | 97.75 ± 0.52 | 97.51 ± 0.70 | 97.62 ± 0.63 | 0.156 b |
| Average SpO2 (%) | 97.46 ± 0.58 | 96.94 ± 7.65 | 97.17 ± 0.73 | 0.005 *,b |
| Minimum SpO2 (%) | 92.18 ± 4.06 | 89.89 ± 4.25 | 90.90 ± 4.29 | 0.009 *,b |
| Skeletal Measurement, Degree | |
| SNBa | Cranial base angulation in midsagittal plane |
| SNA | Angle from S to N to A point |
| SNB | Angle from S to N to B point |
| ANB | Anteroposterior discrepancy degree of maxilla and mandible |
| SNPP | Angulation of the palatal plane with the SN line |
| SNMP | Angulation of the mandibular plane with the SN line. |
| Gonial Angle (Go Angle) | The angle formed by the tangent to the posterior border and the tangent to the lower border of the mandible |
| Upper gonial angle (UGo Angle) | The superior angle of gonial angle divided by N-Go line |
| Lower gonial angle (LGo Angle) | The inferior angle of gonial angle divided by N-Go line |
| Skeletal measurement, mm | |
| SN | Anterior cranial base length, from sella to nasion |
| SBa | Length of sella to basion |
| SGo | Posterior facial height, from sella to gonion |
| NMe | Anterior facial height, from nasion to menton |
| Dental measurement, mm | |
| Overjet | Horizontal relation of maxillary and mandibular incisors |
| Overbite | Vertical relation of maxillary and mandibular incisors |
| Hyoid bone measurement, mm | |
| MP-H | Linear distance between hyoid bone (H) to mandibular plane. |
| H-RGN | Linear distance between H and RGN. |
| Hy-C3 | Linear distance between C3 and H. |
| Airway measurement, mm | |
| LSP | Soft palate length |
| PNSNPhp | Width between PNS and posterior wall of nasopharynx |
| MinRPA | Minimal width of airway behind soft palate perpendicular to posterior pharyngeal wall |
| MinRGA | Minimal width of airway behind tongue perpendicular to posterior pharyngeal wall |
| PNSAD1 | Width from PNS to the nearest adenoid tissue measured along PNS-Ba line |
| PNSAD2 | Width from PNS to the nearest adenoid tissue measured along the line perpendicular to S-Ba line |
| Pre-Treatment | Post-Treatment | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Minimum | Maximum | Mean | SD | Minimum | Maximum | ||
| AHI (No./h) | 4.79 | 3.39 | 1.50 | 14.20 | 1.42 | 1.25 | 0.00 | 5.70 | 0.000 * |
| RDI (No./h) | 7.46 | 5.89 | 2.10 | 28.90 | 4.47 | 4.77 | 0.80 | 21.70 | 0.002 * |
| Mean SpO2 (%) | 97.27 | 0.87 | 94.00 | 98.00 | 97.75 | 0.52 | 96.00 | 98.00 | 0.007 * |
| Average SpO2 (%) | 96.46 | 2.62 | 84.80 | 98.00 | 97.46 | 0.58 | 96.00 | 98.00 | 0.018 * |
| Lowest SpO2 (%) | 89.61 | 4.25 | 79.00 | 95.00 | 92.18 | 4.06 | 78.00 | 97.00 | 0.000 * |
| Pre-Treatment | Post-Treatment | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Minimum | Maximum | Mean | SD | Minimum | Maximum | ||
| AHI (No./h) | 4.41 | 4.03 | 1.10 | 20.90 | 5.66 | 4.99 | 1.40 | 22.90 | 0.035 * |
| RDI (No./h) | 6.59 | 5.01 | 1.70 | 23.50 | 6.59 | 5.34 | 1.80 | 23.20 | 0.993 |
| Mean SpO2 (%) | 97.57 | 0.65 | 95.00 | 98.00 | 97.51 | 0.70 | 96.00 | 98.00 | 0.686 |
| Average SpO2 (%) | 97.11 | 0.83 | 95.00 | 98.00 | 96.94 | 7.65 | 95.00 | 98.00 | 0.275 |
| Lowest SpO2 (%) | 89.94 | 3.80 | 77.00 | 95.00 | 89.89 | 4.25 | 75.00 | 95.00 | 0.846 |
| Measurement | Responsive Group (N = 28) | Non-Responsive Group (N = 35) | Total (N = 63) | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Skeletal measurement | ||||
| SNBa (degree) | 132.22 ± 4.32 | 130.27 ± 4.31 | 131.13 ± 4.39 | 0.041 * |
| SNA (degree) | 80.49 ± 2.39 | 81.43 ± 3.73 | 81.01 ± 3.22 | 0.391 |
| SNB (degree) | 75.59 ± 2.50 | 76.97 ± 3.93 | 76.36 ± 3.42 | 0.139 |
| ANB (degree) | 4.80 ± 2.19 | 4.49 ± 2.45 | 4.62 ± 2.33 | 0.580 |
| SNPP (degree) | 8.56 ± 2.86 | 8.49 ± 2.93 | 8.52 ± 2.87 | 0.994 |
| SNMP (degree) | 37.87 ± 3.96 | 37.75 ± 4.32 | 37.80 ± 4.13 | 0.928 |
| Go Angle (degree) | 126.11 ± 5.41 | 128.98 ± 5.78 | 127.70 ± 5.75 | 0.058 |
| UGo Angle (degree) | 48.46 ± 4.15 | 49.59 ± 4.86 | 49.09 ± 4.56 | 0.290 |
| LGo Angle (degree) | 77.65 ± 3.33 | 79.38 ± 2.95 | 78.61 ± 3.22 | 0.017 * |
| SN (mm) | 63.84 ± 3.53 | 66.15 ± 4.31 | 65.12 ± 4.12 | 0.029 * |
| SBa (mm) | 43.82 ± 4.07 | 44.95 ± 4.68 | 44.45 ± 4.42 | 0.189 |
| SGo (mm) | 72.75 ± 8.82 | 75.74 ± 8.96 | 74.41 ± 8.95 | 0.116 |
| NMe (mm) | 113.55 ± 11.66 | 117.76 ± 10.49 | 115.89 ± 11.14 | 0.184 |
| Dental measurement | ||||
| Overjet (mm) | 3.64 ± 1.57 | 3.17 ± 2.31 | 3.38 ± 2.01 | 0.422 |
| Overbite (mm) | 2.75 ± 1.77 | 3.04 ± 2.11 | 2.91 ± 1.96 | 0.494 |
| Hyoid b. measurement | ||||
| MPH (mm) | 10.94 ± 5.76 | 12.76 ± 5.07 | 11.95 ± 5.42 | 0.118 |
| HRGN (mm) | 30.25 ± 7.08 | 30.94 ± 7.12 | 30.63 ± 7.06 | 0.552 |
| HyC3 (mm) | 32.24 ± 5.43 | 34.26 ± 5.12 | 33.36 ± 5.31 | 0.118 |
| Airway measurement | ||||
| LSP (mm) | 31.05 ± 4.27 | 32.00 ± 3.88 | 31.58 ± 4.05 | 0.251 |
| PNSNPhp (mm) | 15.41 ± 3.67 | 15.56 ± 3.72 | 15.49 ± 3.67 | 0.846 |
| MinRPA (mm) | 6.84 ± 2.83 | 7.44 ± 2.87 | 7.18 ± 2.85 | 0.430 |
| MinRGA (mm) | 11.87 ± 3.08 | 12.42 ± 3.52 | 12.17 ± 3.32 | 0.520 |
| PNSAD1 (mm) | 20.64 ± 4.07 | 20.66 ± 5.02 | 20.65 ± 4.59 | 0.750 |
| PNSAD2 (mm) | 15.98 ± 3.92 | 15.86 ± 3.76 | 15.91 ± 3.81 | 0.978 |
| Variable | Beta * | Odds Ratio (95% Confidence Interval) | p-Value |
|---|---|---|---|
| LGo Angle, Degrees | −0.210 | 0.811 (0.678–0.970) | 0.022 |
| SN, Millimeters | −0.171 | 0.843 (0.733–0.970) | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, Y.-J.; Huang, Y.-S.; Lian, Y.-C.; Lee, Y.-H.; Hervy-Auboiron, M.; Li, C.-H.; Lin, C.-H.; Chuang, L.-C. Craniofacial Morphologic Predictors for Passive Myofunctional Therapy of Pediatric Obstructive Sleep Apnea Using an Oral Appliance with a Tongue Bead. Children 2022, 9, 1073. https://doi.org/10.3390/children9071073
Hwang Y-J, Huang Y-S, Lian Y-C, Lee Y-H, Hervy-Auboiron M, Li C-H, Lin C-H, Chuang L-C. Craniofacial Morphologic Predictors for Passive Myofunctional Therapy of Pediatric Obstructive Sleep Apnea Using an Oral Appliance with a Tongue Bead. Children. 2022; 9(7):1073. https://doi.org/10.3390/children9071073
Chicago/Turabian StyleHwang, Yi-Jing, Yu-Shu Huang, Yun-Chia Lian, Yu-Hsuan Lee, Michele Hervy-Auboiron, Chung-Hsing Li, Cheng-Hui Lin, and Li-Chuan Chuang. 2022. "Craniofacial Morphologic Predictors for Passive Myofunctional Therapy of Pediatric Obstructive Sleep Apnea Using an Oral Appliance with a Tongue Bead" Children 9, no. 7: 1073. https://doi.org/10.3390/children9071073
APA StyleHwang, Y.-J., Huang, Y.-S., Lian, Y.-C., Lee, Y.-H., Hervy-Auboiron, M., Li, C.-H., Lin, C.-H., & Chuang, L.-C. (2022). Craniofacial Morphologic Predictors for Passive Myofunctional Therapy of Pediatric Obstructive Sleep Apnea Using an Oral Appliance with a Tongue Bead. Children, 9(7), 1073. https://doi.org/10.3390/children9071073