
A Comparison of Emergency Department Revisit Rates of Pediatric Patients between Pre-COVID-19 and COVID-19 Periods

 , , , , ,
, , , , ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Period
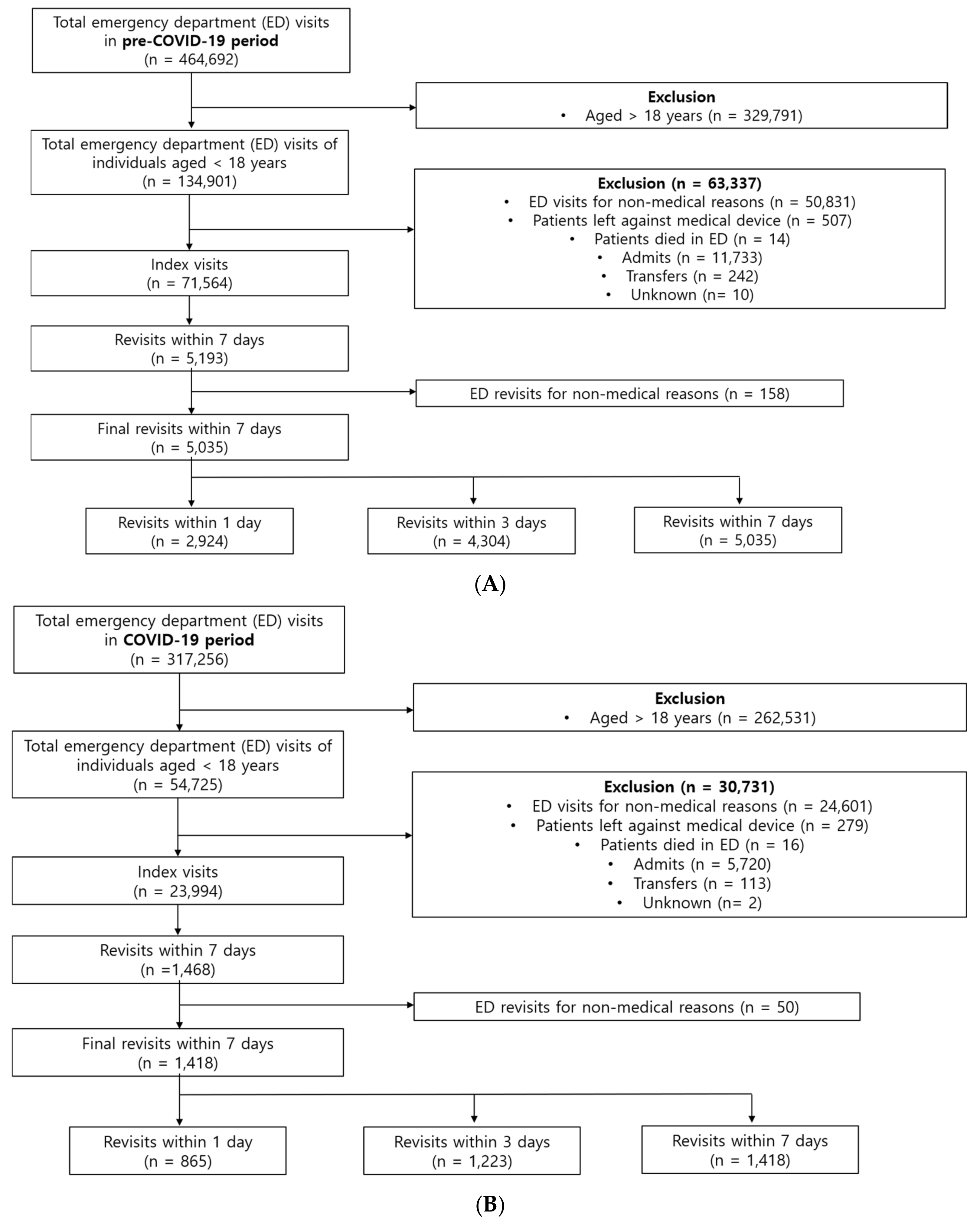
2.2. Study Population
2.3. Identification of Index Visit and Revisit
2.4. Calculation of the Revisit Rate
2.5. Data Collection and Outcome Measurement
2.6. Statistical Analysis
2.7. Ethical Consideration
3. Results
3.1. Revisit Rates in Pre-COVID-19 and COVID-19 Periods
3.2. Baseline Characteristics
3.3. Reduction in the Index Visit and Revisit Rates
3.4. Diagnosis at Revisit According to Age
3.5. Disposition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, K.W.; Lu, Y.H.; Lin, H.J.; Guo, H.R.; Foo, N.P. Unscheduled return visits with and without admission post emergency department discharge. J. Emerg. Med. 2012, 43, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.L.; Wang, F.T.; Chiang, Y.C.; Chiu, Y.F.; Lin, T.G.; Fu, L.F.; Tsai, T.L. Unplanned emergency department revisits within 72 h to a secondary teaching referral hospital in Taiwan. J. Emerg. Med. 2010, 38, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Nuñez, S.; Hexdall, A.; Aguirre-Jaime, A. Unscheduled returns to the emergency department: An outcome of medical errors? Qual. Saf. Health Care 2006, 15, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman, R.D.; Ong, M.; Macpherson, A. Unscheduled return visits to the pediatric emergency department-one-year experience. Pediatr. Emerg. Care 2006, 22, 545–549. [Google Scholar] [CrossRef]
- Safwenberg, U.; Terent, A.; Lind, L. Increased long-term mortality in patients with repeated visits to the emergency department. Eur. J. Emerg. Med. 2010, 17, 274–279. [Google Scholar] [CrossRef]
- Sauvin, G.; Freund, Y.; Saidi, K.; Riou, B.; Hausfater, P. Unscheduled return visits to the emergency department: Consequences for triage. Acad. Emerg. Med. 2013, 20, 33–39. [Google Scholar] [CrossRef]
- Tsai, I.T.; Sun, C.K.; Chang, C.S.; Lee, K.H.; Liang, C.Y.; Hsu, C.W. Characteristics and outcomes of patients with emergency department revisits within 72 h and subsequent admission to the intensive care unit. Ci Ji Yi Xue Za Zhi 2016, 28, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Duseja, R.; Bardach, N.S.; Lin, G.A.; Yazdany, J.; Dean, M.L.; Clay, T.H.; Boscardin, W.J.; Dudley, R.A. Revisit rates and associated costs after an emergency department encounter: A multistate analysis. Ann. Intern. Med. 2015, 162, 750–756. [Google Scholar] [CrossRef]
- Ahmed, A.E.; BI, A.L.; Alrajhi, M.N.; Almazroa, H.R.; AlBuraikan, D.A.; Albaijan, M.A.; Nasim, M.; Alsalamah, M.A.; McClish, D.K.; Al-Jahdali, H. Emergency department 72-h revisits among children with chronic diseases: A Saudi Arabian study. BMC Pediatr. 2018, 18, 205. [Google Scholar] [CrossRef]
- Saunders, N.R.; To, T.; Parkin, P.C.; Guttmann, A. Emergency Department Revisits by Urban Immigrant Children in Canada: A Population-Based Cohort Study. J. Pediatr. 2016, 170, 218–226. [Google Scholar] [CrossRef]
- Akenroye, A.T.; Thurm, C.W.; Neuman, M.I.; Alpern, E.R.; Srivastava, G.; Spencer, S.P.; Simon, H.K.; Tejedor-Sojo, J.; Gosdin, C.H.; Brennan, E.; et al. Prevalence and predictors of return visits to pediatric emergency departments. J. Hosp. Med. 2014, 9, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.S.; Shapiro, D.J.; Cabana, M.D.; Maselli, J.H.; Hersh, A.L. A national depiction of children with return visits to the emergency department within 72 h, 2001–2007. Pediatr. Emerg. Care 2012, 28, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, G.; Ghirardo, S.; Fiorese, I.; Proietti, I.; Monasta, L.; Minute, M.; Barbi, E.; Calligaris, L. Risk of hospitalisation after early-revisit in the emergency department. J. Paediatr. Child. Health 2017, 53, 850–854. [Google Scholar] [CrossRef] [PubMed]
- Kurt, F.; Hanalioğlu, D.; Can, F.; Kurtipek, F.E.; Yakut, H.; Misirlioğlu, E.D. Evaluation of Unscheduled Return Visits to the Pediatric Emergency Department and Risk Factors for Admission After Return Visit. Pediatr. Emerg. Care 2022, 38, e967–e972. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Macaulay, C.B.; Truong, M.; Meckler, G.D.; Doan, Q.H. Return visits to the pediatric emergency department: A multicentre retrospective cohort study. Cjem 2018, 20, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Nijman, R.G.; Borensztajn, D.H.; Zachariasse, J.M.; Hajema, C.; Freitas, P.; Greber-Platzer, S.; Smit, F.J.; Alves, C.F.; van der Lei, J.; Steyerberg, E.W.; et al. A clinical prediction model to identify children at risk for revisits with serious illness to the emergency department: A prospective multicentre observational study. PLoS ONE 2021, 16, e0254366. [Google Scholar] [CrossRef]
- Seiler, M.; Furrer, P.R.; Staubli, G.; Albisetti, M. Unplanned Return Visits to a Pediatric Emergency Department. Pediatr. Emerg. Care 2021, 37, e746–e749. [Google Scholar] [CrossRef] [Green Version]
- Sung, S.F.; Liu, K.E.; Chen, S.C.; Lo, C.L.; Lin, K.C.; Hu, Y.H. Predicting Factors and Risk Stratification for Return Visits to the Emergency Department Within 72 Hours in Pediatric Patients. Pediatr. Emerg. Care 2015, 31, 819–824. [Google Scholar] [CrossRef]
- Kilicaslan, O.; Sonmez, F.T.; Gunes, H.; Temizkan, R.C.; Kocabay, K.; Saritas, A. Short Term Unscheduled Revisits to Paediatric Emergency Department—A Six Year Data. J. Clin. Diagn Res. 2017, 11, SC12–SC15. [Google Scholar] [CrossRef]
- Berry, J.G.; Rodean, J.; Hall, M.; Alpern, E.R.; Aronson, P.L.; Freedman, S.B.; Brousseau, D.C.; Shah, S.S.; Simon, H.K.; Cohen, E.; et al. Impact of Chronic Conditions on Emergency Department Visits of Children Using Medicaid. J. Pediatr. 2017, 182, 267–274. [Google Scholar] [CrossRef]
- Perry, A.M.; Caviness, A.C.; Allen, J.Y. Characteristics and diagnoses of neonates who revisit a pediatric emergency center. Pediatr. Emerg. Care 2013, 29, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Bae, W.; Choi, A.; Kim, K.; Kang, H.M.; Kim, S.Y.; Lee, H.; Yoo, I.H.; Yang, E.A.; Chun, Y.H.; Bin, J.H.; et al. One-year changes in the pediatric emergency department caused by prolonged COVID-19 pandemic. Pediatr. Int. 2021, 23, 142. [Google Scholar] [CrossRef]
- Raucci, U.; Musolino, A.M.; Di Lallo, D.; Piga, S.; Barbieri, M.A.; Pisani, M.; Rossi, F.P.; Reale, A.; Ciofi Degli Atti, M.L.; Villani, A.; et al. Impact of the COVID-19 pandemic on the Emergency Department of a tertiary children’s hospital. Ital. J. Pediatr. 2021, 47, 21. [Google Scholar] [CrossRef]
- Bae, S.J.; Chung, H.S.; Namgung, M.; Choi, Y.H.; Min, J.H.; Lee, D.H. Comparison of the Clinical Process and Outcomes in Patients after Coronavirus Infection 2019 Outbreak. Medicina 2021, 57, 1086. [Google Scholar] [CrossRef] [PubMed]
- Bottari, G.; Stellacci, G.; Ferorelli, D.; Dell’Erba, A.; Aricò, M.; Benevento, M.; Palladino, G.; Solarino, B. Imaging appropriateness in pediatric radiology during COVID-19 Pandemic: A retrospective comparison with no COVID-19 period. Children 2021, 8, 463. [Google Scholar] [CrossRef]
- Cheng, S.Y.; Wang, H.T.; Lee, C.W.; Tsai, T.C.; Hung, C.W.; Wu, K.H. The characteristics and prognostic predictors of unplanned hospital admission within 72 h after ED discharge. Am. J. Emerg. Med. 2013, 31, 1490–1494. [Google Scholar] [CrossRef]
- Panda, P.K.; Gupta, J.; Chowdhury, S.R.; Kumar, R.; Meena, A.K.; Madaan, P.; Sharawat, I.K.; Gulati, S. Psychological and Behavioral Impact of Lockdown and Quarantine Measures for COVID-19 Pandemic on Children, Adolescents and Caregivers: A Systematic Review and Meta-Analysis. J. Trop. Pediatr. 2021, 67, fmaa122. [Google Scholar] [CrossRef]
- Bae, S.J.; Lee, D.H.; Lee, D.H.; Seo, A.Y.; Choi, Y.H. Comparative analysis of characteristics of patients who visited the emergency department due to suicide attempts during coronavirus disease-2019 pandemic. Omega 2022, 302228221106286. [Google Scholar] [CrossRef]
- Leon, S.L.; Polihronis, C.; Cloutier, P.; Zemek, R.; Newton, A.S.; Gray, C.; Cappelli, M. Family factors and repeat pediatric emergency department visits for mental health: A retrospective cohort study. J. Can. Acad. Child. Adolesc. Psychiatry 2019, 28, 9–20. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Pre-COVID-19 Period | COVID-19 Period | |||||
|---|---|---|---|---|---|---|
| Index ED Visits n = 71,564 | Revisits n = 5035 | p-Value | Index ED Visits n = 23,994 | Revisits n = 1418 | p-Value | |
| Age (years) | 4.9 ± 4.7 | 3.8 ± 3.9 | <0.001 | 5.7 ± 5.3 | 4.9 ± 5.3 | <0.001 |
| Triage level (KTAS) | <0.001 | <0.001 | ||||
| Level 1 | 41 (0.1) | 3 (0.2) | 14 (0.1) | 6 (0.3) | ||
| Level 2 | 2244 (3.1) | 9 (0.7) | 871 (3.6) | 90 (4.8) | ||
| Level 3 | 40,308 (56.3) | 552 (40.2) | 12,818 (53.4) | 1198 (63.4) | ||
| Level 4 | 23,468 (32.8) | 645 (47.0) | 8135 (33.9) | 422 (22.3) | ||
| Level 5 | 5503 (7.7) | 163 (11.9) | 2156 (9.0) | 175 (9.3) | ||
| Transportation to the hospital | 0.364 | 0.295 | ||||
| Self-presentation | 68,062 (95.1) | 1316 (95.9) | 22,372 (93.2) | 1775 (93.9) | ||
| Ambulance | 3494 (4.9) | 56 (4.1) | 1622 (6.8) | 116 (6.1) | ||
| Vital signs at presentation | ||||||
| Systolic blood pressure (mmHg) | 113.3 ± 14.5 | 105.7 ± 15.9 | <0.001 | 116.7 ± 15.7 | 114.6 ± 15.0 | 0.001 |
| Diastolic blood pressure (mmHg) | 69.1 ± 10.6 | 65.1 ± 9.8 | <0.001 | 71.2 ± 11.8 | 69.9 ± 11.4 | 0.007 |
| Mean arterial pressure (mmHg) | 83.8 ± 10.7 | 78.7 ± 10.8 | <0.001 | 86.4 ± 11.9 | 84.8 ± 11.5 | 0.001 |
| Pulse rate (times/min) | 122.0 ± 26.9 | 106.5 ± 21.6 | <0.001 | 119.4 ± 27.2 | 123.7 ± 28.4 | <0.001 |
| Respiratory rate (breaths/min) | 24.5 ± 5.1 | 21.9 ± 3.3 | <0.001 | 23.9 ± 5.2 | 24.7 ± 5.6 | <0.001 |
| Body temperature (°C) | 37.6 ± 1.0 | 37.3 ± 1.0 | <0.001 | 37.2 ± 2.5 | 37.2 ± 3.9 | 0.898 |
| ED LOS (minutes) | 105 ± 96 | 113 ± 67 | <0.001 | 107 ± 102 | 169 ± 189 | <0.001 |
| Pre-COVID-19 Period | COVID-19 Period | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| <1 Year | 1–3 Years | 4–6 Years | 7–12 Years | 13–17 Years | <1 Year | 1–3 Years | 4–6 Years | 7–12 Years | 13–17 Years | |
| 1 day | Infectious and parasitic diseases (44.9) | Infectious and parasitic diseases (47.1) | Infectious and parasitic diseases (43.9) | Infectious and parasitic diseases (43.8) | Infectious and parasitic diseases (36.4) | Infectious and parasitic diseases (47.5) | Infectious and parasitic diseases (45.8) | Infectious and parasitic diseases (48.5) | Infectious and parasitic diseases (38.9) | Infectious and parasitic diseases (33.8) |
| Diseases of the respiratory system (33.9) | Diseases of the respiratory system (29.9) | Diseases of the respiratory system (27.2) | Diseases of the respiratory system (20.2) | Diseases of the digestive system (23.8) | Diseases of the respiratory system (20.6) | Diseases of the respiratory system (24.7) | Diseases of the digestive system (19.6) | Diseases of the digestive system (19.8) | Diseases of the digestive system (19.9) | |
| Diseases of the genitourinary system (7.4) | Diseases of the genitourinary system (6.0) | Diseases of the digestive system (13.2) | Diseases of the digestive system (17.3) | Diseases of the respiratory system (13.3) | Diseases of the genitourinary system (16.3) | Diseases of the skin and subcutaneous tissue (6.8) | Diseases of the skin and subcutaneous tissue (9.3) | Diseases of the skin and subcutaneous tissue (11.9) | Diseases of the respiratory system (8.1) | |
| 3 days | Infectious and parasitic diseases (44.3) | Diseases of the respiratory system (47.1) | Infectious and parasitic diseases (44.5) | Infectious and parasitic diseases (43.9) | Infectious and parasitic diseases (35.1) | Infectious and parasitic diseases (45.7) | Infectious and parasitic diseases (47.1) | Infectious and parasitic diseases (43.4) | Infectious and parasitic diseases (37.5) | Infectious and parasitic diseases (32.0) |
| Diseases of the respiratory system (35.5) | Infectious and parasitic diseases (30.8) | Diseases of the respiratory system (28.3) | Diseases of the respiratory system (20.4) | Diseases of the digestive system (23.2) | Diseases of the respiratory system (17.8) | Diseases of the respiratory system (23.8) | Diseases of the digestive system (20.4) | Diseases of the digestive system (22.7) | Diseases of the digestive system (20.0) | |
| Diseases of the genitourinary system (6.7) | Diseases of the digestive system (5.0) | Diseases of the digestive system (11.4) | Diseases of the digestive system (16.3) | Diseases of the respiratory system (11.8) | Diseases of the genitourinary system (14.9) | Diseases of the skin and subcutaneous tissue (7.6) | Diseases of the respiratory system (10.5) | Diseases of the skin and subcutaneous tissue (10.8) | Diseases of the respiratory system (8.0) | |
| 7 days | Infectious and parasitic diseases (43.9) | Diseases of the respiratory system (46.8) | Infectious and parasitic diseases (43.8) | Infectious and parasitic diseases (43.7) | Infectious and parasitic diseases (33.1) | Infectious and parasitic diseases (44.0) | Infectious and parasitic diseases (45.3) | Infectious and parasitic diseases (41.3) | Infectious and parasitic diseases (34.3) | Infectious and parasitic diseases (28.4) |
| Diseases of the respiratory system (35.1) | Infectious and parasitic diseases (29.8) | Diseases of the respiratory system (27.6) | Diseases of the respiratory system (20.1) | Diseases of the digestive system (24.6) | Diseases of the respiratory system (17.3) | Diseases of the respiratory system (23.9) | Diseases of the digestive system (19.0) | Diseases of the digestive system (23.6) | Diseases of the digestive system (22.7) | |
| Diseases of the genitourinary system (6.2) | Diseases of the digestive system (5.3) | Diseases of the digestive system (11.2) | Diseases of the digestive system (15.4) | Diseases of the respiratory system (11.9) | Diseases of the genitourinary system (13.7) | Diseases of the skin and subcutaneous tissue (7.8) | Diseases of the respiratory system (14.5) | Diseases of the skin and subcutaneous tissue (10.2) | Mental and behavioural disorders (7.6) | |
| Pre-COVID-19 Period | COVID-19 Period | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Disposition | <1 Year | 1–3 Years | 4–6 Years | 7–12 Years | 13–17 Years | <1 Year | 1–3 Years | 4–6 Years | 7–12 Years | 13–17 Years | |
| 1 day | Discharge, n (%) | 301 (58.6) | 999 (68.5) | 323 (68.6) | 231 (68.8) | 83 (58.0) | 77 (54.6) | 234 (64.1) | 53 (54.6) | 66 (52.4) | 79 (58.1) |
| General ward, n (%) | 211 (41.1) | 456 (31.3) | 147 (31.2) | 103 (30.7) | 57 (39.9) | 63 (44.7) | 130 (35.6) | 43 (44.3) | 59 (46.8) | 54 (39.7) | |
| ICU, n (%) | 1 (0.2) | 1 (0.1) | 1 (0.2) | 1 (0.3) | 1 (0.7) | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | |
| Transfer, n (%) | 1 (0.2) | 2 (0.1) | 0 (0.0) | 1 (0.3) | 2 (1.4) | 0 (0.0) | 1 (0.3) | 1 (1.0) | 1 (0.8) | 2 (1.5) | |
| Death, n (%) | 0 (0.0) | 1 (0.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 3 days | Discharge, n (%) | 478 (62.4) | 1538 (71.6) | 473 (69.0) | 316 (68.7) | 129 (61.1) | 117 (56.3) | 345 (67.4) | 96 (63.2) | 94 (53.4) | 112 (64.0) |
| General ward, n (%) | 286 (37.3) | 638 (29.3) | 212 (30.9) | 142 (30.9) | 79 (37.4) | 88 (42.3) | 166 (32.4) | 55 (36.2) | 80 (45.5) | 60 (34.3) | |
| ICU, n (%) | 1 (0.1) | 1 (0.0) | 1 (0.1) | 1 (0.2) | 1 (0.5) | 2 (1.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.6) | |
| Transfer, n (%) | 1 (0.1) | 2 (0.1) | 0 (0.0) | 1 (0.2) | 2 (0.9) | 1 (0.5) | 1 (0.2) | 1 (0.7) | 2 (1.1) | 2 (1.1) | |
| Death, n (%) | 0 (0.0) | 1 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 7 days | Discharge, n (%) | 576 (64.9) | 1871 (72.8) | 560 (71.4) | 371 (69.6) | 171 (65.8) | 146 (58.9) | 386 (68.4) | 118 (65.9) | 123 (56.9) | 136 (64.5) |
| General ward, n (%) | 309 (34.8) | 694 (27.0) | 223 (28.4) | 160 (30.0) | 86 (33.1) | 99 (39.9) | 177 (31.4) | 60 (33.5) | 91 (42.1) | 72 (34.1) | |
| ICU, n (%) | 1 (0.1) | 1 (0.0) | 1 (0.1) | 1 (0.2) | 1 (0.4) | 2 (0.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.5) | |
| Transfer, n (%) | 1 (0.1) | 3 (0.1) | 0 (0.0) | 1 (0.2) | 2 (0.8) | 1 (0.4) | 1 (0.2) | 1 (0.6) | 2 (0.9) | 2 (0.9) | |
| Death, n (%) | 0 (0.0) | 1 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namgung, M.; Lee, D.H.; Bae, S.J.; Chung, H.S.; Park, J.Y.; Kim, K.; Lee, C.A.; Kim, D.H.; Kim, E.C.; Lim, J.Y.; et al. A Comparison of Emergency Department Revisit Rates of Pediatric Patients between Pre-COVID-19 and COVID-19 Periods. Children 2022, 9, 1003. https://doi.org/10.3390/children9071003
Namgung M, Lee DH, Bae SJ, Chung HS, Park JY, Kim K, Lee CA, Kim DH, Kim EC, Lim JY, et al. A Comparison of Emergency Department Revisit Rates of Pediatric Patients between Pre-COVID-19 and COVID-19 Periods. Children. 2022; 9(7):1003. https://doi.org/10.3390/children9071003
Chicago/Turabian StyleNamgung, Myeong, Dong Hoon Lee, Sung Jin Bae, Ho Sub Chung, Ji Young Park, Keon Kim, Choung Ah Lee, Duk Ho Kim, Eui Chung Kim, Jee Yong Lim, and et al. 2022. "A Comparison of Emergency Department Revisit Rates of Pediatric Patients between Pre-COVID-19 and COVID-19 Periods" Children 9, no. 7: 1003. https://doi.org/10.3390/children9071003
APA StyleNamgung, M., Lee, D. H., Bae, S. J., Chung, H. S., Park, J. Y., Kim, K., Lee, C. A., Kim, D. H., Kim, E. C., Lim, J. Y., Han, S. S., & Choi, Y. H. (2022). A Comparison of Emergency Department Revisit Rates of Pediatric Patients between Pre-COVID-19 and COVID-19 Periods. Children, 9(7), 1003. https://doi.org/10.3390/children9071003