
Parent-Reported Perceived Cognitive Functioning Identifies Cognitive Problems in Children Who Survived Neonatal Critical Illness

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Measures
2.4. Data Analyses
- Cohen’s d (= mean–population mean/sample SD): small = 0.2, medium = 0.5, large = 0.8.
- r (= standardized test statistic/√N): small = 0.1, medium = 0.3, large = 0.5.
- Cohen’s f (= (√η2/1 − η2)): small = 0.1, medium = 0.25, large = 0.4.
- Strengths of the Kendall tau correlation coefficients were interpreted as followed [35]: τ: weak = 0.1, moderate = 0.4, strong = 0.7.
3. Results
3.1. Participants
3.2. Questionnaire Outcomes
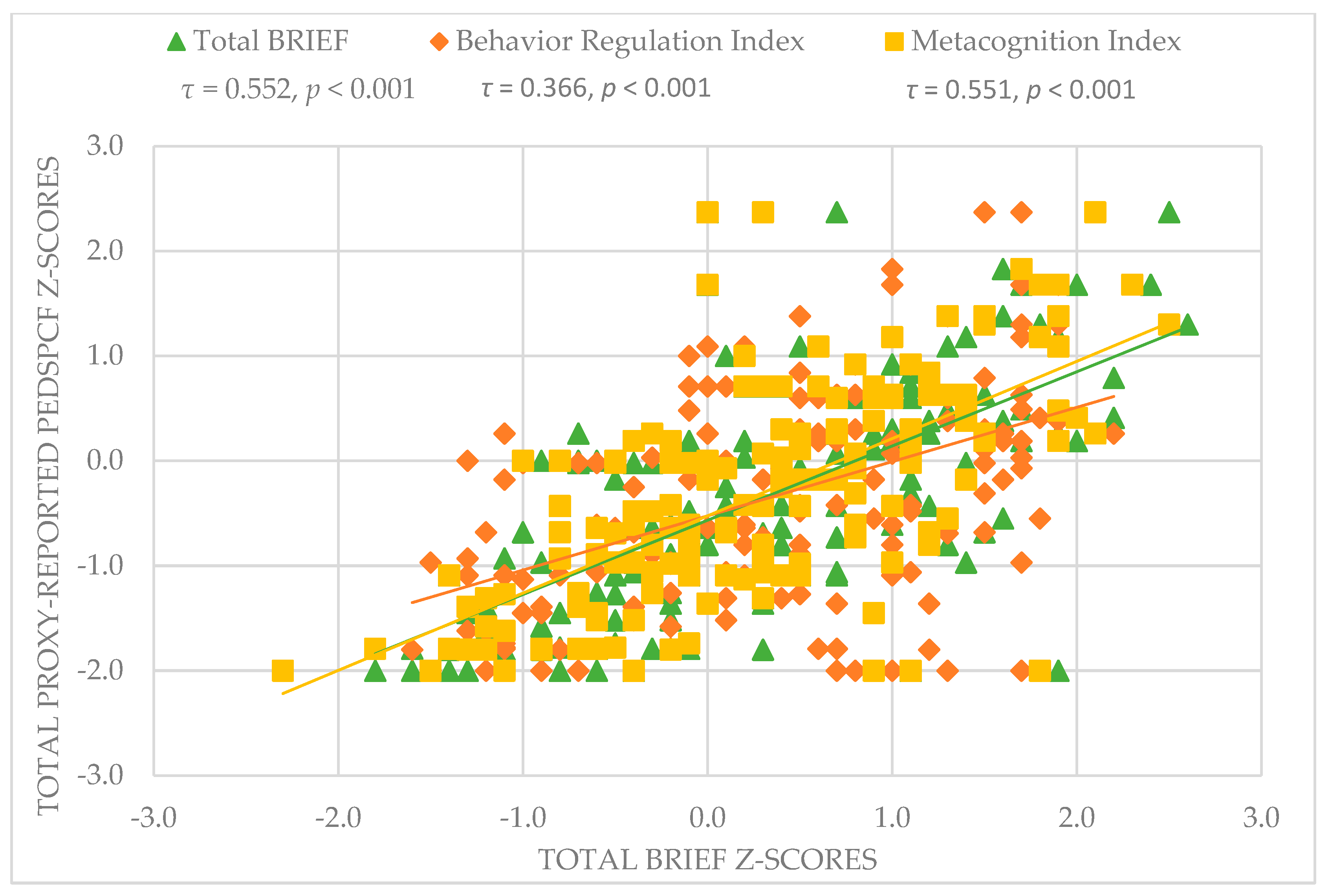
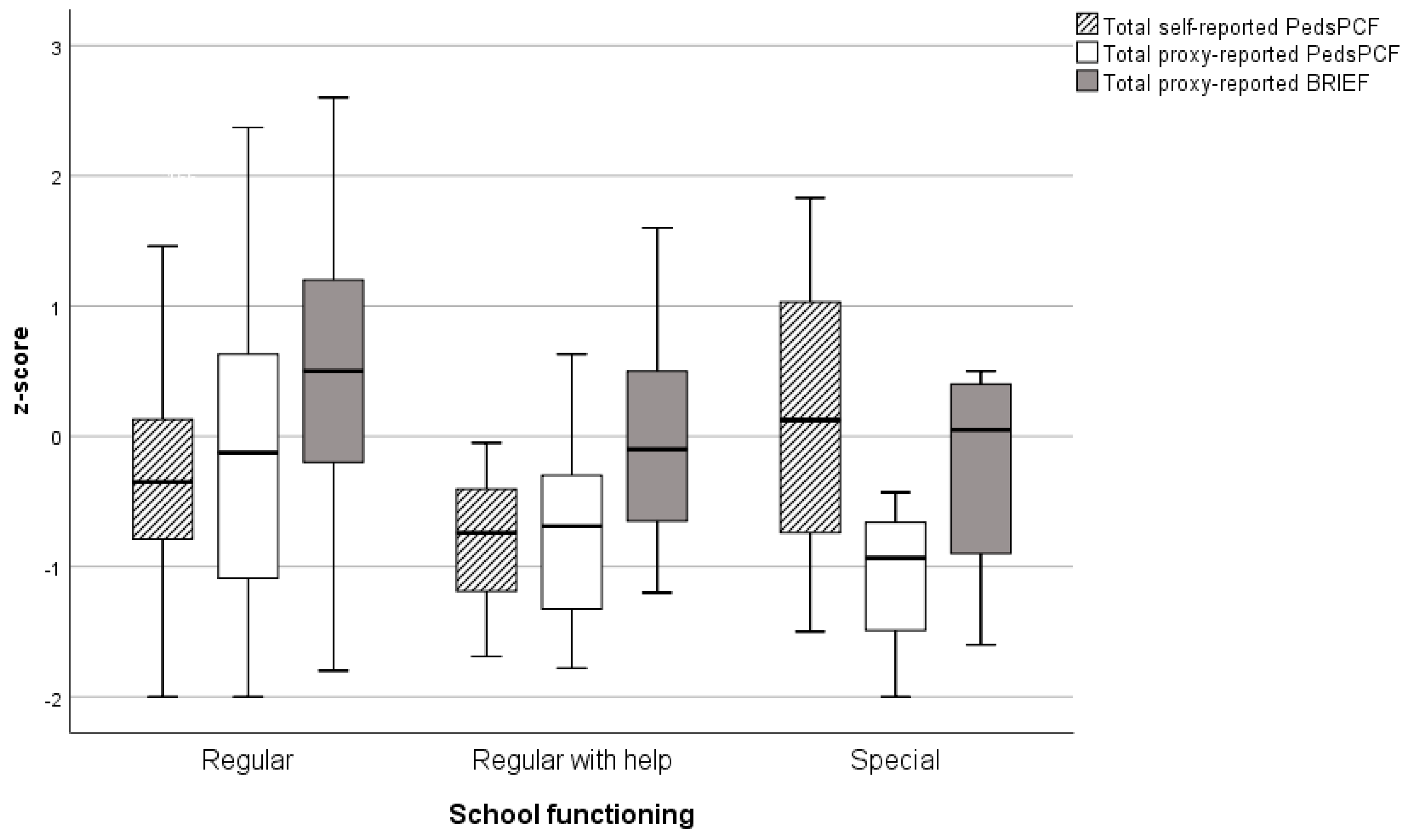
3.3. Associations of PedsPCF with BRIEF, Outcomes of NPA, and School Functioning
3.4. Associations of 30- and 10-Item PedsPCF
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glinianaia, S.V.; Morris, J.K.; Best, K.E.; Santoro, M.; Coi, A.; Armaroli, A.; Rankin, J. Long-term survival of children born with congenital anomalies: A systematic review and meta-analysis of population-based studies. PLoS Med. 2020, 17, e1003356. [Google Scholar] [CrossRef] [PubMed]
- UK collaborative randomised trial of neonatal extracorporeal membrane oxygenation. UK Collaborative ECMO Trail Group. Lancet 1996, 348, 75–82. [CrossRef]
- Harmsen, W.J.; Aarsen, F.J.; Zijp, M.H.M.va.; van Rosmalen, J.M.; Wijnen, R.M.H.; Tibboel, D.; IJsselstijn, H. Developmental problems in patients with oesophageal atresia: A longitudinal follow-up study. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F214–F219. [Google Scholar] [CrossRef] [PubMed]
- Leeuwen, L.; Schiller, R.M.; Rietman, A.B.; van Rosmalen, J.; Wildschut, E.D.; Houmes, R.J.M.; Tibboel, D.; IJsselstijn, H. Risk Factors of Impaired Neuropsychologic Outcome in School-Aged Survivors of Neonatal Critical Illness. Crit. Care Med. 2018, 46, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Madderom, M.J.; Reuser, J.J.; Utens, E.M.; van Rosmalen, J.; Raets, M.; Govaert, P.; Steiner, K.; Gischler, S.J.; Tibboel, D.; van Heijst, A.F.J.; et al. Neurodevelopmental, educational and behavioral outcome at 8 years after neonatal ECMO: A nationwide multicenter study. Intensive Care Med. 2013, 39, 1584–1593. [Google Scholar] [CrossRef]
- Madderom, M.J.; Schiller, R.M.; Gischler, S.J.; van Heijst, A.F.; Tibboel, D.; Aarsen, F.K.; IJsselstijn, H. Growing Up After Critical Illness: Verbal, Visual-Spatial, and Working Memory Problems in Neonatal Extracorporeal Membrane Oxygenation Survivors. Crit. Care Med. 2016, 44, 1182–1190. [Google Scholar] [CrossRef]
- Madderom, M.J.; Toussaint, L.; Zijp, M.H.M.v.-d.C.-v.; Gischler, S.J.; Wijnen, R.M.; Tibboel, D.; IJsselstijn, H. Congenital diaphragmatic hernia with(out) ECMO: Impaired development at 8 years. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F316–F322. [Google Scholar] [CrossRef]
- Mazer, P.; Gischler, S.J.; Zijp, M.H.M.V.D.C.-V.; Tibboel, D.; Bax, N.M.; IJsselstijn, H.; Dijk, M.V.A.N.; Duivenvoorden, H.J. Early developmental assessment of children with major non-cardiac congenital anomalies predicts development at the age of 5 years. Dev. Med. Child Neurol. 2010, 52, 1154–1159. [Google Scholar] [CrossRef]
- Schiller, R.M.; Madderom, M.J.; Reuser, J.J.; Steiner, K.; Gischler, S.J.; Tibboel, D.; van Heijst, A.F.J.; IJsselstijn, H. Neuropsychological Follow-up After Neonatal ECMO. Pediatrics 2016, 138, e20161313. [Google Scholar] [CrossRef] [PubMed]
- Schiller, R.; IJsselstijn, H.; Hoskote, A.; White, T.; Verhulst, F.; van Heijst, A.; Tibboel, D. Memory deficits following neonatal critical illness: A common neurodevelopmental pathway. Lancet Child Adolesc. Health 2018, 2, 281–289. [Google Scholar] [CrossRef]
- Gischler, S.J.; Mazer, P.; Duivenvoorden, H.J.; van Dijk, M.; Bax, N.M.; Hazebroek, F.W.; Tibboel, D. Interdisciplinary structural follow-up of surgical newborns: A prospective evaluation. J. Pediatr. Surg. 2009, 44, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- IJsselstijn, H.; Gischler, S.J.; Wijnen, R.M.H.; Tibboel, D. Assessment and significance of long-term outcomes in pediatric surgery. Semin. Pediatr. Surg. 2017, 26, 281–285. [Google Scholar] [CrossRef]
- IJsselstijn, H.; Gischler, S.J.; Toussaint, L.; Spoel, M.; Zijp, M.H.; Tibboel, D. Growth and development after oesophageal atresia surgery: Need for long-term multidisciplinary follow-up. Paediatr. Respir. Rev. 2016, 19, 34–38. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sreeram, I.I.; Ten Kate, C.A.; van Rosmalen, J.; Schnater, J.M.; Gischler, S.J.; Wijnen, R.M.H.; IJsselstijn, H.; Rietman, A.B. Patient-Reported Outcome Measures and Clinical Outcomes in Children with Foregut Anomalies. Children 2021, 8, 587. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Butt, Z.; Zelko, F.; Cella, D.; Krull, K.R.; Kieran, M.W.; Goldman, S. Development of a parent-report cognitive function item bank using item response theory and exploration of its clinical utility in computerized adaptive testing. J. Pediatr. Psychol. 2011, 36, 766–779. [Google Scholar] [CrossRef]
- Lai, J.S.; Zelko, F.; Butt, Z.; Cella, D.; Kieran, M.W.; Krull, K.R.; Magasi, S.; Goldman, S. Parent-perceived child cognitive function: Results from a sample drawn from the US general population. Childs Nerv. Syst. 2011, 27, 285–293. [Google Scholar] [CrossRef]
- Marchal, J.P.; de Vries, M.; Conijn, J.; Rietman, A.B.; IJsselstijn, H.; Tibboel, D.; Haverman, L.; Maurice-Stam, H.; Oostrom, K.J.; Grootenhuis, M.A. Pediatric Perceived Cognitive Functioning: Psychometric Properties and Normative Data of the Dutch Item Bank and Short Form. J. Int. Neuropsychol. Soc. 2019, 25, 845–856. [Google Scholar] [CrossRef]
- Hijkoop, A.; Rietman, A.B.; Wijnen, R.M.H.; Tibboel, D.; Cohen-Overbeek, T.E.; van Rosmalen, J.; IJsselstijn, H. Omphalocele at school age: What do parents report? A call for long-term follow-up of complex omphalocele patients. Early Hum. Dev. 2019, 137, 104830. [Google Scholar] [CrossRef] [PubMed]
- Hijkoop, A.; Rietman, A.B.; Wijnen, R.M.H.; Tibboel, D.; Cohen-Overbeek, T.E.; van Rosmalen, J.; IJsselstijn, H. Gastroschisis at school age: What do parents report? Eur. J. Pediatr. 2019, 178, 1405–1412. [Google Scholar] [CrossRef]
- Lai, J.S.; Bregman, C.; Zelko, F.; Nowinski, C.; Cella, D.; Beaumont, J.J.; Goldman, S. Parent-reported cognitive function is associated with leukoencephalopathy in children with brain tumors. Qual. Life Res. 2017, 26, 2541–2550. [Google Scholar] [CrossRef]
- Ohnemus, D.; Neighbors, K.; Sorensen, L.G.; Lai, J.S.; Alonso, E.M. A Pilot Study of a Screening Tool for Pediatric Minimal Hepatic Encephalopathy. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Gioia, G.A.; Isquith, P.K.; Guy, S.C.; Kenworthy, L. Behavior Rating Inventory of Executive Function BRIEF: Professional Manual; Psychological Assessment Resources(PAR): Lutz, FL, USA, 2000. [Google Scholar]
- Smidts, D.P.; Huizinga, M. BRIEF Behavior Rating Inventory of Executive Function-Manual 2. Norms (Dutch: Executieve Functies Gedragsvragenlijsten: Handleiding), 4-23; Hogrefe: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Kort, W.; Schittekatte, M.; Dekker, P.H.; Verhaeghe, P.; Compaan, E.L.; Bosmans, M.; Vermeir, G. WISC-III NL Wechsler Intelligence Scale for Children. Handleiding en Verantwoording [Dutch version of the WISC-III], 3rd ed.; Harcourt Test Publishers/Nederlands Instituut voor Psychologen: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Pearson. WAIS-IV-NL, Nederlandstalige berwerking. In Technische Handleiding; Pearson Assessment & Information: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Pearson. WAIS-IV-NL, Nederlandstalige bewerking. In Afname En Scoringshandleiding; Pearson Assessment & Information: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Emslie, H.; WIlson, F.C.; Burden, V. Behavioral Assessment of the Dysexecutive Syndrome for Children (BADS-C), Dutch Version; Amsterdam Harcourt: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W. Neuropsychological Assessment, 4th ed; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Schmand, B.; Houx, P.; De Koning, I. Dutch Norms for STROOP Color-Word Test, Trail Making Test, Rey Auditory Verbal-Learning Test, Verbal Fluency, and Story Recall of Rivermead Behavioural Memory Test; Division Neuropsychology of the Dutch Institute for Psychology: Amsterdam, The Netherlands, 2003. [Google Scholar]
- van den Burg, W.; Kingma, A. Performance of 225 Dutch school children on Rey’s Auditory Verbal Learning Test (AVLT): Parallel test-retest reliabilities with an interval of 3 months and normative data. Arch. Clin. Neuropsychol. 1999, 14, 545–559. [Google Scholar] [PubMed]
- Vos, P. Bourdon-Vos. Handleiding (Manual Dot Cancellation Test); Swets en Zeitlinger: Lisse, The Netherlands, 1992. [Google Scholar]
- Watanabe, K.; Ogino, T.; Nakano, K.; Hattori, J.; Kado, Y.; Sanada, S.; Ohtsuka, Y. The Rey-Osterrieth Complex Figure as a measure of executive function in childhood. Brain Dev. 2005, 27, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D.; Naglieri, J.A. Wechsler Nonverbal Scale of Ability; Pearson: San Antonio, TX, USA, 2006. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Goyal, S.; Park, A.; Zeglam, A.; Brown, H.; Pemberton, J.D. Choroidal Ganglioneuroma and Orbital Plexiform Neurofibroma Presenting as Buphthalmos in an Infant With Neurofibromatosis Type 1. Ophthalmic. Plast Reconstr. Surg. 2016, 32, e87–e89. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Marquez de Prado, B.; Russo, A.F.; Hammond, D.L. Heat hyperalgesia and mechanical hypersensitivity induced by calcitonin gene-related peptide in a mouse model of neurofibromatosis. PLoS ONE 2014, 9, e106767. [Google Scholar]
- Petrie, A.; Sabin, C. Medical Statistics at a Glance, 3rd ed; Wiley-Blackwell: Oxford, UK, 2009. [Google Scholar]
- Bone, M.F.; Feinglass, J.M.; Goodman, D.M. Risk factors for acquiring functional and cognitive disabilities during admission to a PICU*. Pediatr. Crit. Care Med. 2014, 15, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Heath, N.L.; Glen, T. Positive illusory bias and the self-protective hypothesis in children with learning disabilities. J. Clin. Child Adolesc. Psychol. 2005, 34, 272–281. [Google Scholar] [CrossRef] [PubMed]
- IJsselstijn, H.; Breatnach, C.; Hoskote, A.; Greenough, A.; Patel, N.; Capolupo, I.; Morini, F.; Scharbatke, H.; Kipfmueller, F.; Ertresvag, K.; et al. Defining outcomes following congenital diaphragmatic hernia using standardised clinical assessment and management plan (SCAMP) methodology within the CDH EURO consortium. Pediatr. Res. 2018, 84, 181–189. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Characteristics | |
| Sex | |
| Male | 99 (59%) |
| Female | 69 (41%) |
| Clinical characteristics | |
| Diagnosis | |
| CDH | 57 (34%) |
| without ECMO treatment | 46 (81%) |
| with ECMO treatment | 11 (19%) |
| EA | 54 (32%) |
| CLM | 20 (12%) |
| Neonatal ECMO, non-CDH | 37 (22%) |
| Gestational age (weeks) | 39.0 (37.1–40.4) |
| Birth weight (grams) | 3150 (2725–3530) |
| Duration of initial hospital stay (days) | 22 (13–48) |
| Duration of initial ventilation (days) | 7 (2–16) |
| At follow-up | |
| Age at assessment | |
| 8 years | 57 (34%) |
| 12 years | 64 (38%) |
| 17 years | 47 (28%) |
| School functioning | |
| Regular | 130 (78%) |
| Regular with help | 22 (13%) |
| Special educational needs | 14 (8%) |
| Missing | 2 (1%) |
| Measurement | Mean (SD) | p-Value | Effect Size (d/r) | |
|---|---|---|---|---|
| Self-reported | PedsPCF 30-item | −0.35 (0.88) | <0.001 | 0.40 1 |
| Proxy-reported | PedsPCF 30-item | −0.36 (1.06) | <0.001 | 0.33 1 |
| Total BRIEF | 0.33 (0.98) | <0.001 | 0.34 2 | |
| BRI | 0.37 (0.97) | <0.001 | 0.35 1 | |
| MCI | 0.26 (0.96) | 0.001 | 0.27 2 |
| Variable | Mean (SD) | p-Value | Effect Size (d/r) | |
|---|---|---|---|---|
| Intelligence | Total IQ | 100 (18) | 0.951 | 0.00 2 |
| Attention | TMTA t | 0.30 (1.15) | <0.001 *** | 0.37 1 |
| Stroop IF | −0.23 (1.19) | 0.051 | 0.16 1 | |
| DCT-ST | −0.93 (1.28) | <0.001 *** | 0.60 1 | |
| DCT-SD | −1.17 (1.52) | <0.001 *** | 0.60 1 | |
| Verbal Memory | Total Digit Span | 0.04 (1.00) | 0.565 | 0.04 1 |
| RAVLT total | −0.35 (1.26) | <0.001 *** | 0.28 2 | |
| RAVLT recall | −0.64 (1.38) | <0.001 *** | 0.40 1 | |
| Visuospatial Memory | WNV-SS total | −0.21 (0.92) | 0.004 ** | 0.23 2 |
| WNV-SS forward | −0.07 (1.04) | 0.298 | 0.08 1 | |
| RCFT immediate | −0.62 (1.23) | <0.001 *** | 0.42 1 | |
| RCFT delayed | −0.76 (1.26) | <0.001 *** | 0.51 1 | |
| RCFT recognition | −0.08 (1.21) | 0.933 | 0.01 1 | |
| Executive Functioning | BADS-C Key Search | 0.18 (1.10) | 0.052 | 0.15 1 |
| BADS-C Modified Six Elements | −0.48 (0.81) | <0.001 *** | 0.50 1 | |
| TMTB t | 0.09 (1.08) | 0.013 * | 0.20 1 | |
| WNV-SS backwards | −0.29 (0.86) | <0.001 *** | 0.35 1 | |
| PSI | −0.04 (1.13) | 0.620 | 0.04 2 |
| Variable | Cases (n) | B (SE) | 95% CI of B | R2 | p-Value | |
|---|---|---|---|---|---|---|
| Intelligence | WISC-III-NL Total IQ | 158 | 0.022 (0.004) | 0.013–0.031 | 0.141 | <0.001 *** |
| Attention | TMTA t | 155 | 0.223 (0.071) | 0.082–0.364 | 0.060 | 0.002 ** |
| Stroop IF | 149 | 0.067 (0.074) | −0.079–0.213 | 0.006 | 0.365 | |
| DCT-ST | 151 | 0.139 (0.066) | 0.009–0.269 | 0.029 | 0.036 * | |
| DCT-SD | 151 | 0.106 (0.056) | −0.004–0.271 | 0.024 | 0.059 | |
| Verbal Memory | WISC-III-NL Total Digit Span | 157 | 0.255 (0.083) | 0.090–0.419 | 0.057 | 0.003 ** |
| RAVLT total | 158 | 0.231 (0.065) | 0.103–0.359 | 0.075 | <0.001 *** | |
| RAVLT recall | 158 | 0.188 (0.060) | 0.070–0.305 | 0.060 | 0.002 ** | |
| Visuospatial Memory | WNV-SS total | 155 | 0.266 (0.091) | 0.085–0.446 | 0.052 | 0.004 ** |
| WNV-SS forwards | 155 | 0.159 (0.082) | −0.003–0.322 | 0.024 | 0.055 | |
| RCFT immediate | 155 | 0.191 (0.067) | 0.059–0.323 | 0.051 | 0.005 ** | |
| RCFT delayed | 155 | 0.191 (0.066) | 0.061–0.321 | 0.052 | 0.004 ** | |
| RCFT recognition | 156 | 0.164 (0.071) | 0.024–0.304 | 0.034 | 0.022 * | |
| Executive Functioning | BADS-C Key Search | 155 | 0.208 (0.076) | 0.058–0.358 | 0.047 | 0.007 ** |
| BADS-C Modified Six Elements | 88 **** | 0.083 (0.144) | −0.202–0.369 | 0.004 | 0.563 | |
| TMTB t | 147 | 0.236 (0.083) | 0.071–0.400 | 0.052 | 0.005 ** | |
| WNV-SS backwards | 155 | 0.275 (0.097) | 0.082–0.467 | 0.049 | 0.005 ** | |
| Processing Speed Index | 158 | 0.319 (0.069) | 0.183–0.456 | 0.120 | <0.001 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilik, Y.; IJsselstijn, H.; Gischler, S.J.; van Gils-Frijters, A.; Schnater, J.M.; Rietman, A.B. Parent-Reported Perceived Cognitive Functioning Identifies Cognitive Problems in Children Who Survived Neonatal Critical Illness. Children 2022, 9, 900. https://doi.org/10.3390/children9060900
Ilik Y, IJsselstijn H, Gischler SJ, van Gils-Frijters A, Schnater JM, Rietman AB. Parent-Reported Perceived Cognitive Functioning Identifies Cognitive Problems in Children Who Survived Neonatal Critical Illness. Children. 2022; 9(6):900. https://doi.org/10.3390/children9060900
Chicago/Turabian StyleIlik, Yerel, Hanneke IJsselstijn, Saskia J. Gischler, Annabel van Gils-Frijters, Johannes M. Schnater, and Andre B. Rietman. 2022. "Parent-Reported Perceived Cognitive Functioning Identifies Cognitive Problems in Children Who Survived Neonatal Critical Illness" Children 9, no. 6: 900. https://doi.org/10.3390/children9060900
APA StyleIlik, Y., IJsselstijn, H., Gischler, S. J., van Gils-Frijters, A., Schnater, J. M., & Rietman, A. B. (2022). Parent-Reported Perceived Cognitive Functioning Identifies Cognitive Problems in Children Who Survived Neonatal Critical Illness. Children, 9(6), 900. https://doi.org/10.3390/children9060900