
The STEP Program—A Qualitative Study of the Supportive Therapeutic Excursion Program and Its Effect on Enabling Parental Self-Efficacy and Connectedness after the Stress-Experience of the NICU

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Method
2.2. Sampling
2.3. Data Collection
2.4. Data Processing and Analysis
3. Results
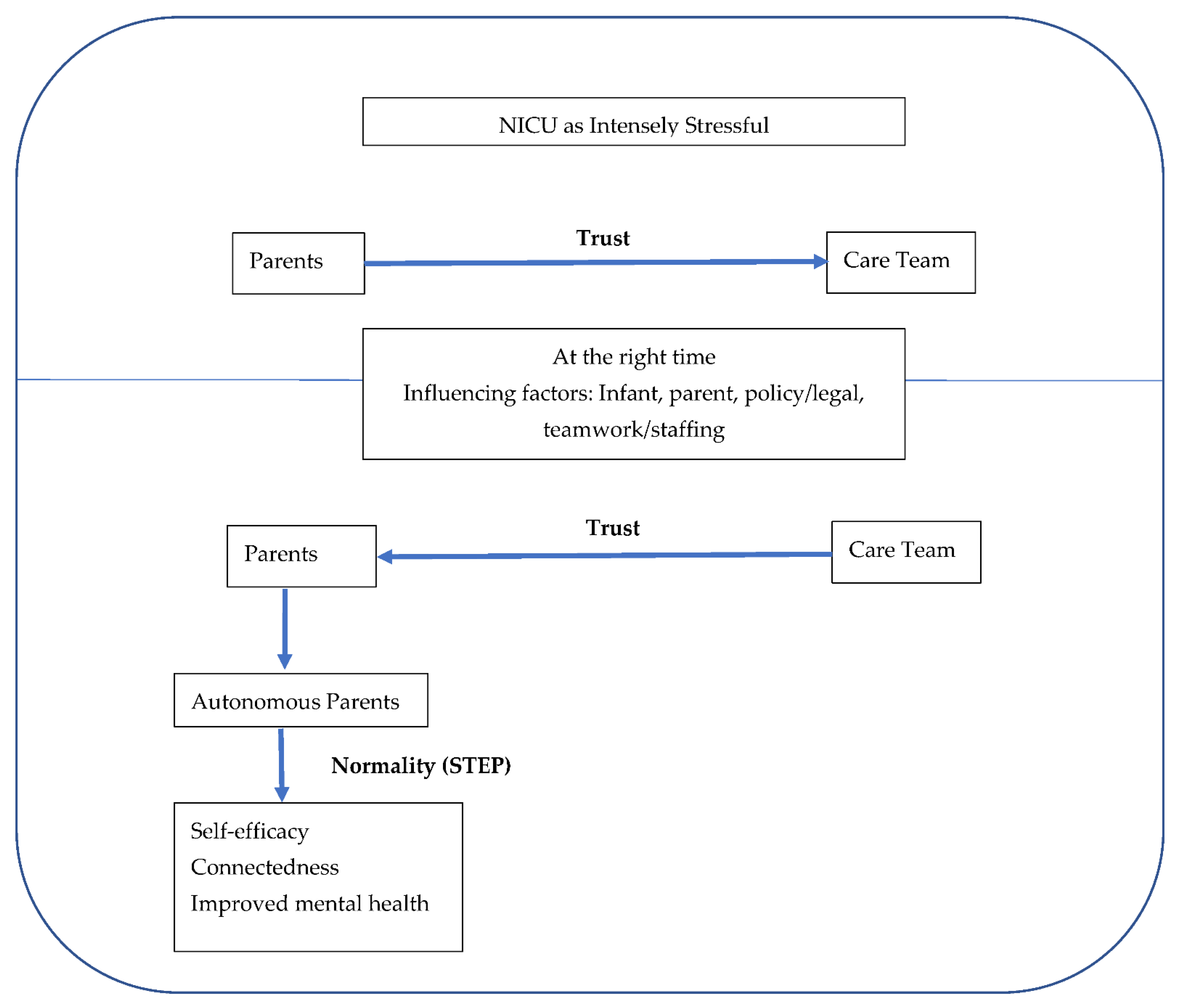
3.1. NICU as an Intensely Stressful Experience
“It was the worst time; it was horrible…. NICU changes you. And like, I went from being a realist to being a pessimist, like, very much.”Participant 5 (parent)
“It was honestly the toughest time of our lives I guess”Participant 1 (parent)
“Stressful, very stressful. I mean, everyone was helpful, and it wasn’t anything to do with the care, just being there was stressful.”Participant 13 (parent)
“I had some already latent mental health concerns and then the NICU just brought that up.”Participant 12 (parent)
“One of our goals was to just completely defer our trust to the doctors and to not sort of be marked down by some of the panic and the fear.”Participant 6 (parent)
“Just because like we trusted the doctor so much…so I had full faith that if they’re ready, I’m definitely ready.”Participant 1 (parent)
3.2. At the Right Time
3.2.1. On the Institution of STEP
“Doing something that a normal family would get to do, like going for a walk is just probably as normal as breathing. Right? For the NICU parents, they’ve been deprived of a lot of things. Yeah, they likely haven’t had the baby shower they’ve maybe not ever had, they haven’t had the prenatal education classes because they already had a baby, the baby. You know, they haven’t had, the mother…. hasn’t had that experience of having a huge belly and everybody asking… so there’s all these things that are normal in the walk of pregnancy that are our moms don’t get. So trying to bring them these pieces of normal; I think it’s so important.”Participant 7 (staff)
3.2.2. On Eligibility Factors
“I mean, they have to be for sure stable, physically stable, from a cardiac respiratory point of view, or the one that has the odd desaturation or bradycardia, the parents know how to respond. And we’ve been through this scenario many times, so it’s an older baby with reflux. And every once in a while, for sure they have a bit of reflux. And, you know, they do some breath holding, they dipped down quickly, but right back up, and the parents know how to intervene. And this is something that they’ll be dealing with at home, then I don’t have a problem with that. But if I was in the same scenario, if it was a parent who couldn’t demonstrate that they knew what to do, that I’m not okay with that.”Participant 2 (staff)
3.2.3. On Legal/Policy Factors
“The stroller walks, the big concern as well, like liability. And what if you know, something happens when they’re out with their baby? I mean, you’re the one that’s caring for their baby. But if you don’t go with them, how much of that is your responsibility? And I think that’s where the resistance comes from. I think a lot of the nurses that are concerned, feel like should something happen when the moms go out with the baby, that’s our, our license, essentially, by sending them out there. So I think that is the huge, the huge part of the resistance.”Participant 4 (staff)
3.2.4. On Teamwork and Staffing
“It just requires me to reorganise maybe my time a little, you know, if I’m, if I’m truly busy, I’ll say to them, you know, right now, I’m sorry, I can’t take you outside right now, if you want to go for a walk in the hallways feel free to do that. This is the time that I will be available, or I’ll negotiate with a colleague, maybe who’s, who’s free to go and take them out. So it’s just a little bit of juggling, and it’s what we do all the time in the NICU anyways.”Participant 20 (staff)
“There are cons to the nurses too. If the nurse has got a really difficult assignment, like if you’ve got a baby that’s a little bit sicker with a baby that Mom wants to take it out for a stroll. I mean, it becomes like, Okay, well, [not now] because I’ve got this baby getting a blood transfusion or, we’re short staffed. And if we’re really short staffed, and if we’re really, you know, it shouldn’t matter, but it does matter. Right? And so, you know, sometimes it becomes a negative having to [send this] baby out for a walk, because, because you’ve got so many things to do. So you know, you’re encouraging the family unit and developmentally and, and all the things that go with it as, as sending out positive parents and positive vibes. But as I say that that one negative is the acuity of the unit.”Participant 9 (staff)
3.3. Trust Transfer
“Okay, well, you’re the parent, you’re the mom, you know, so we’re going to transition you into more making those decisions. And I felt like that was very, very helpful for me because, like I was quite freaked out. Like I didn’t know, I didn’t know how to be a parent, right? Like, I actually felt really supported. And also it was a bit of a necessary push for me to take ownership over, like making some decisions I hadn’t made previously really.”Participant 10 (parent)
“I think it’s definitely good for parents to participate [in taking on more decisions], just because it gets them into that next level. When I was with and in the NICU, like, I want to know what’s the next the next step and, and getting him home.”Participant 13 (parent)
3.4. Autonomy, Self-Efficacy and Connectedness
“I was [now] in charge of my child. And that it was up to me to decide how to be safe or not safe. And to give myself a little bit of self-confidence, and I think that’s important for moms, especially when you’re getting closer to discharge, it’s the lack of self-confidence and knowledge in your own capabilities of being a mother because it’s stripped from you right at the door.”Participant 12 (parent)
“I have had a baby who’s had a small episode of spitting up or vomiting while they went out for a walk. But the parents, the parents managed it very appropriately, they turned the baby on his side, they wiped his mouth. They came back. And obviously they reported to me what had happened, but they weren’t, they weren’t more anxious. They weren’t, they weren’t freaked out about it, they, they handled it really well. I’ve never had a baby who had an actual spell, sometimes the monitor will go off because the baby’s kicking. But by that time, usually I find the parents because they have been present. They understand they look at their baby, they see their baby is pink and breathing. And they realise that the monitor is not picking up the reading properly. So that it’s not a concern with the baby. It’s really just a problem with the, with the connection.”Participant 20 (staff)
“I remember putting on my jacket and tucking to the wind and like walking onto the elevator and it felt so normal. You don’t really think about when you’re in the NICU because you are so isolated… and everybody there is in the same position like physical and mental space. I also didn’t socialise that much because you just invariably end up talking about, you compare your babies and did they get this steroid and what how much food are they taking and how much weight did they gain and it feels like even though it starts off wholesome it always kind of ends in a weird I never really felt like I liked it. So anyway, it felt so nice just be able to, like I was just a regular mom walking through the halls with her baby.”Participant 6 (parent)
“It feels good that the medical professionals are putting their faith and confidence in you as a parent to be alone with your kid…. I went up there and I got a coffee and that was that was pretty great. Like [with] the stroller finally I could just sit with her. She’d like sort of be sleeping or just kind of relaxing and I could finally just have a coffee. And then I was like walking the hallway. And I ran into some of the other moms that I knew. And so that was really nice to be able to be like, ‘here’s my kid. She’s doing great’. And one of the other moms, I think, a few, like, twice, maybe three times, she happened to be on a stroller walk with her baby at the same time as me as well. So we kind of like walked a little bit together. And that was pretty great. That felt pretty, like normal, you know, mom behaviour.”Participant 10 (parent)
3.5. Mental Health
“It was nice. It was really nice because it gave us a break from the old little room, just like to breathe outside and just not constantly look at the numbers and have you fixated with the issues that she could have.”Participant 1 (parent)
“I think it was like 109 days, I kind of went a bit crazy. And I was like, I’m not a prisoner in here and I just need to get outside. So this led up to us going outside for a walk. I was like, ‘I just need to go outside like I can’t be in this. I’ve been in here since June and it is now Thanksgiving and I just need to go outside’.”Participant 6 (parent)
“I think stroller walks and especially being able to go outside with your infant, even if it’s just around the grounds; it gives them a chance to sort of improve their mental health and then ground them a little bit more with their, with their child.”Participant 4 (staff)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Category | NICU |
| Sub-Category | Policies and Guidelines Folder |
| Title: | Infant Sign out of Neonatal Intensive Care Unit |
| Policy Number | |
| Old Policy Number: | |
| Issued By: | |
| Approved By: | Inter-professional Policy Committee |
| Department: | Dan Women and Babies Program NICU |
| Original: | TBD |
| Reviewed: (mm/dd/yyyy) | |
| Revised: (mm/dd/yyyy) | |
| Next Review Date | |
| Review Reminder: | 30 and 60 Day Reminders |
| Reviewer’s Email Address: | jo-ann.alfred@sunnybrook.ca; Paige.Church@sunnybrook.ca |
| Essential Elements | Rationale | |
| 1. | An updated order to be written as required by the MRP in the chart once infant deemed safe for Off Unit Time and risk/benefit discussed with SDM(s) | Provides permission for infant to leave the unit with SDM(s) |
| 2. | Verbal agreement between SDM(s) and nurse to leave the NICU, specifying timing of outing and confirming agreement with the Policy requirements | Allows for open communication between team and SDM(s) confirming the exact timing that infant will be off unit and that the understand and agree to the requirements of this policy |
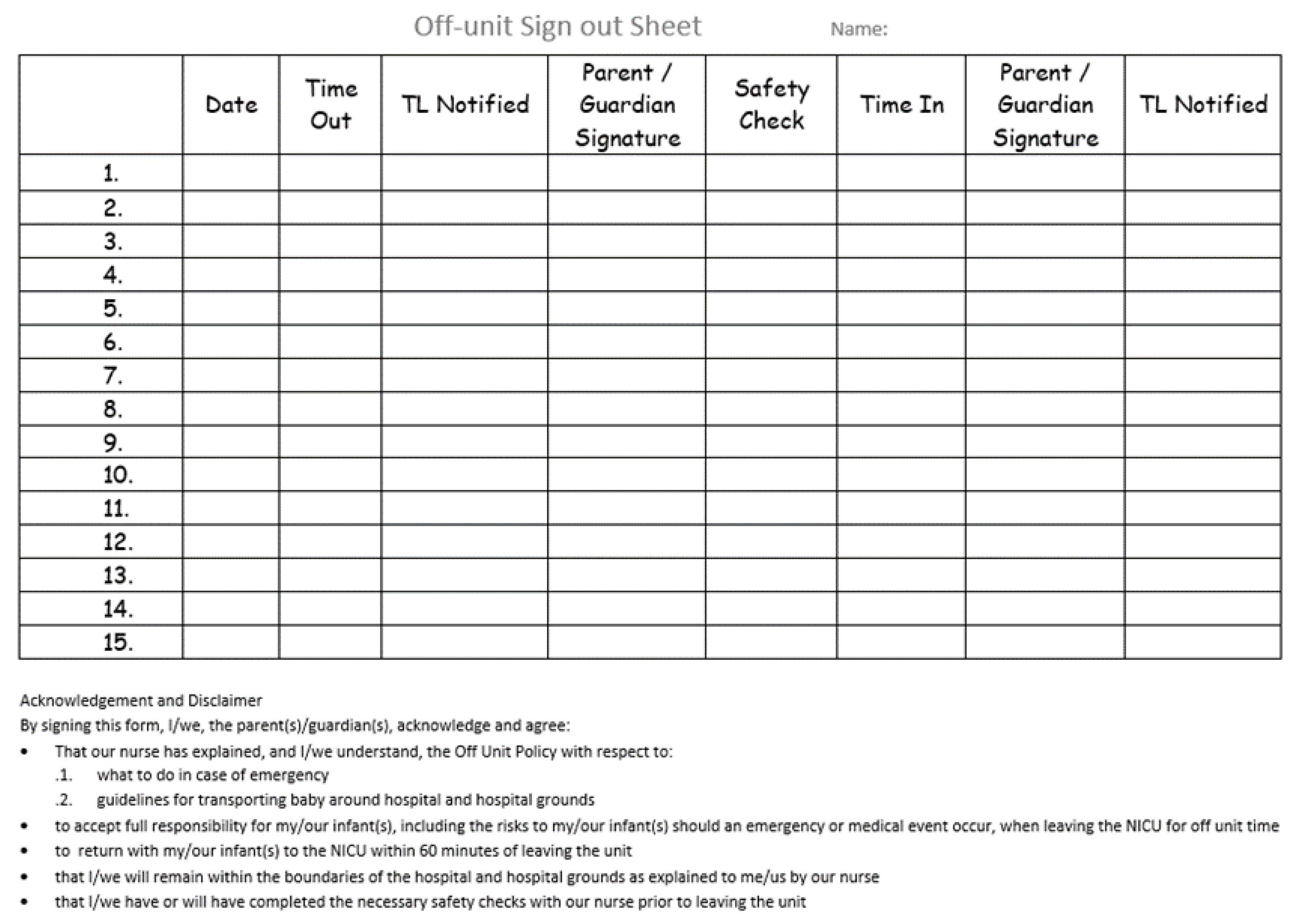
| 3. | SDM(s) to sign “Out” of and “In” to the NICU using Individualized Off Unit Time sign out sheet (Figure A2). | Records Off Unit Time and confirms verbal agreement and that SDM(s) acknowledge and agree to accept responsibility for their infant and risks related to Off Unit Time |
| 4. | SDM(s) must advise nurse of destination location and estimated time of return | Provides information on location of infants and ensures that nurse can locate SDM(s) in case of emergency |
| 5. | Safety checks completed by bedside nurse
| Ensures safety of infant following NICU safety check guidelines. |
| 6. | Off Unit Time sign out sheet to be kept with the infant’s chart | Ensures accurate record keeping of events |


Appendix B
- What is your role in the NICU?
- How many years have you worked in any NICU? And how many years have you been working at the NICU at Sunnybrook?
- What activities do you encourage parents to do as they near discharge to prepare the parents for discharge? (examples, bathing, giving medications, feeding)
- Are you familiar with the concept of having parents take their baby for a walk in a stroller outside of the NICU but while still an inpatient in the NICU?
- Have you cared for a family that participated in this program?
- What, if any, were the concerns you had prior to the walk starting?
- What, if any, were the concerns you had after the walks got started
- What, if any, were the benefits of the walks for families?
- How did the walks affect your workload?
- How do you think that the walks affected your ability to do your job?
- Were there things that made it harder for you to help a family go for a walk?
- Were there things that made it easier to help a family to take their child for a walk?
- Do you think that families in the NICU should be taking their babies out for walks? Please share your thoughts.
- Please tell us about your baby who was in the NICU at Sunnybrook.
- Is your baby a boy or girl? Singleton or twins?
- Was this child your first child or did you have other children at home?
- How many weeks gestation (or how far along in your pregnancy were you when you had your baby?)
- How long did your baby stay in the hospital? Do you remember when you went home?
- When was your baby in the hospital (months and year)?
- Did your baby go home on oxygen? Did your baby require surgery or medicine for their eyes for retinopathy of prematurity?
- Was your baby enrolled on the BOOST (Building Opportunities for Optimal and Smooth Transitions) team?
- Had you heard about BOOST before being enrolled? If so, what had you heard?
- Did you take your baby for a walk in a stroller while in the NICU?
- Did you take your baby around the NICU or within the hospital?
- Did you take your child outside of the hospital?
- What did you feel as you took your first walk? Were you scared/excited/nervous?
- How did you feel once you had your first walk? (Proud, excited…)
- Did you go for more walks?
- If yes, why did you keep going for walks?
- Did you experience barriers to taking your baby for a walk?
- Were there things that you could do or the staff could do to help make the walks more available to you?
References
- Pichler-Stachl, E.; Pichler, G.; Baik, N.; Urlesberger, B.; Alexander, A.; Urlesberger, P.; Cheung, P.-Y.; Schmölzer, G.M. Maternal stress after preterm birth: Impact of length of antepartum hospital stay. Women Birth 2016, 29, e105–e109. [Google Scholar] [CrossRef] [PubMed]
- Ionio, C.; Colombo, C.; Brazzoduro, V.; Mascheroni, E.; Confalonieri, E.; Castoldi, F.; Lista, G. Mothers and fathers in NICU: The impact of preterm birth on parental distress. Eur. J. Psychol. 2016, 12, 604–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, S.D.; Vaucher, Y.E. Neonatal Intensive Care Unit: Special Issues for the At-Risk Infant and Family. In Encounters with Children, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2006; pp. 170–199. [Google Scholar] [CrossRef]
- Erdei, C.; Liu, C.H.; Machie, M.; Church, P.T.; Heyne, R. Parent mental health and neurodevelopmental outcomes of children hospitalized in the neonatal intensive care unit. Early Hum. Dev. 2020, 154, 105278. [Google Scholar] [CrossRef] [PubMed]
- Treyvaud, K.; Lee, K.J.; Doyle, L.W.; Anderson, P.J. Very Preterm Birth Influences Parental Mental Health and Family Outcomes Seven Years after Birth. J. Pediatr. 2014, 164, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puthussery, S.; Chutiyami, M.; Tseng, P.-C.; Kilby, L.; Kapadia, J. Effectiveness of early intervention programs for parents of preterm infants: A meta-review of systematic reviews. BMC Pediatr. 2018, 18, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, K.; Robson, K.; Bracht, M.; Cruz, M.; Lui, K.; Alvaro, R.; da Silva, O.; Monterrosa, L.; Narvey, M.; Ng, E.; et al. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: A multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc. Health 2018, 2, 245. [Google Scholar] [CrossRef]
- Benzies, K.M.; Magill-Evans, J.E.; Hayden, K.A.; Ballantyne, M. Key Components of Early Intervention Programs for Preterm Infants and Their Parents: A Systematic Review and Meta-analysis. 2013. Available online: http://www.biomedcentral.com/1471-2393/13/S1/S10 (accessed on 9 March 2022).
- Kavan, M.G.; Elsasser, G.N.; Barone, E.J. The Physician’s Role in Managing Acute Stress Disorder. Am. Fam. Physician 2012, 86, 643–649. Available online: https://www.aafp.org/afp/2012/1001/p643.html (accessed on 9 March 2022). [PubMed]
- Williams, A.B.; Hendricks-Muñoz, K.D.; Parlier-Ahmad, A.B.; Griffin, S.; Wallace, R.; Perrin, P.B.; Rybarczyk, B.; Ward, A. Posttraumatic stress in NICU mothers: Modeling the roles of childhood trauma and infant health. J. Perinatol. 2021, 41, 2009–2018. [Google Scholar] [CrossRef] [PubMed]
- Van den Bos Gary, R. APA Dictionary of Psychology. American Psychological Association. 2007. Available online: https://dictionary.apa.org/self-efficacy (accessed on 18 March 2022).
- Lee, R.M.; Draper, M.; Lee, S. Social connectedness, dysfunctional interpersonal behaviors, and psychological distress: Testing a mediator model. J. Couns. Psychol. 2001, 48, 310–318. Available online: https://psycnet.apa.org/record/2001-07409-008 (accessed on 18 March 2022). [CrossRef]
- Morse, J.M. The Significance of Saturation. Qual. Health Res. 1995, 5, 147–149. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Dejonckheere, M.; Vaughn, L.M. Semistructured interviewing in primary care research: A balance of relationship and rigour. Fam. Med. Community Health 2019, 7, e000057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreiner, G.E. Tabula Geminus: A “both/and” approach to coding and theorizing. In Handbook of Qualitative Organizational Research: Innovative Pathways and Methods; Routledge/Taylor & Francis Group: New York, NY, USA, 2016; pp. 350–361. [Google Scholar]
- Vance, A.J.; Malin, K.J.; Miller, J.; Shuman, C.J.; Moore, T.A.; Benjamin, A. Parents’ pandemic NICU experience in the United States: A qualitative study. BMC Pediatr. 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, E.; Shrira, A. Social Connectedness Moderates the Relationship between Warfare Exposure, PTSD Symptoms, and Health Among Older Adults. Psychiatry 2018, 82, 158–172. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Participant Number | Role | Characteristics | Time between Discharge and Interview (Months) |
|---|---|---|---|
| 1 | Parent | GA at birth 24 + 6 | 10 |
| 3 | Parent | GA at birth 23 + 6 | 21 |
| 5 | Parent | GA at birth 30 + 5 | 22 |
| 6 | Parent | GA at birth 29 | 58 |
| 10 | Parent | GA at birth 25 + 1 | 19 |
| 11 | Parent | GA at birth 25 | 29 |
| 12 | Parent | GA at birth 24 | 41 |
| 13 | Parent | GA at birth 25 + 5 | 23 |
| 14 | Parent | GA at birth 23 + 5 | 10 |
| 15 | Parent | GA at birth 24 | 43 |
| 2 | Staff | Beside Nurse; 33 years of experience | N/A |
| 4 | Staff | Beside Nurse; 18 years of experience | N/A |
| 7 | Staff | Nurse Practitioner; 34 years of experience | N/A |
| 8 | Staff | Nurse Practitioner; 18 years of experience | N/A |
| 9 | Staff | Bedside Nurse; 30 years of experience | N/A |
| 16 | Staff | NICU Team Leader-7 years; Bedside nurse-17 years | N/A |
| 17 | Staff | NICU Team Leader; 31 years of experience | N/A |
| 18 | Staff | Bedside Nurse; 10 years of experience | N/A |
| 19 | Staff | Bedside Nurse; 20 years of experience | N/A |
| 20 | Staff | Bedside Nurse; 22 years of experience | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGuire-Brown, M.; Banihani, R.; Watson, J.; Ng, E.; Rocha, C.; Borges, L.; Church, P.T. The STEP Program—A Qualitative Study of the Supportive Therapeutic Excursion Program and Its Effect on Enabling Parental Self-Efficacy and Connectedness after the Stress-Experience of the NICU. Children 2022, 9, 591. https://doi.org/10.3390/children9050591
McGuire-Brown M, Banihani R, Watson J, Ng E, Rocha C, Borges L, Church PT. The STEP Program—A Qualitative Study of the Supportive Therapeutic Excursion Program and Its Effect on Enabling Parental Self-Efficacy and Connectedness after the Stress-Experience of the NICU. Children. 2022; 9(5):591. https://doi.org/10.3390/children9050591
Chicago/Turabian StyleMcGuire-Brown, Makini, Rudaina Banihani, Jo Watson, Eugene Ng, Colleen Rocha, Laura Borges, and Paige Terrien Church. 2022. "The STEP Program—A Qualitative Study of the Supportive Therapeutic Excursion Program and Its Effect on Enabling Parental Self-Efficacy and Connectedness after the Stress-Experience of the NICU" Children 9, no. 5: 591. https://doi.org/10.3390/children9050591
APA StyleMcGuire-Brown, M., Banihani, R., Watson, J., Ng, E., Rocha, C., Borges, L., & Church, P. T. (2022). The STEP Program—A Qualitative Study of the Supportive Therapeutic Excursion Program and Its Effect on Enabling Parental Self-Efficacy and Connectedness after the Stress-Experience of the NICU. Children, 9(5), 591. https://doi.org/10.3390/children9050591