
Sensory-Adapted Dental Environment for the Treatment of Patients with Autism Spectrum Disorder

 ,
, 
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
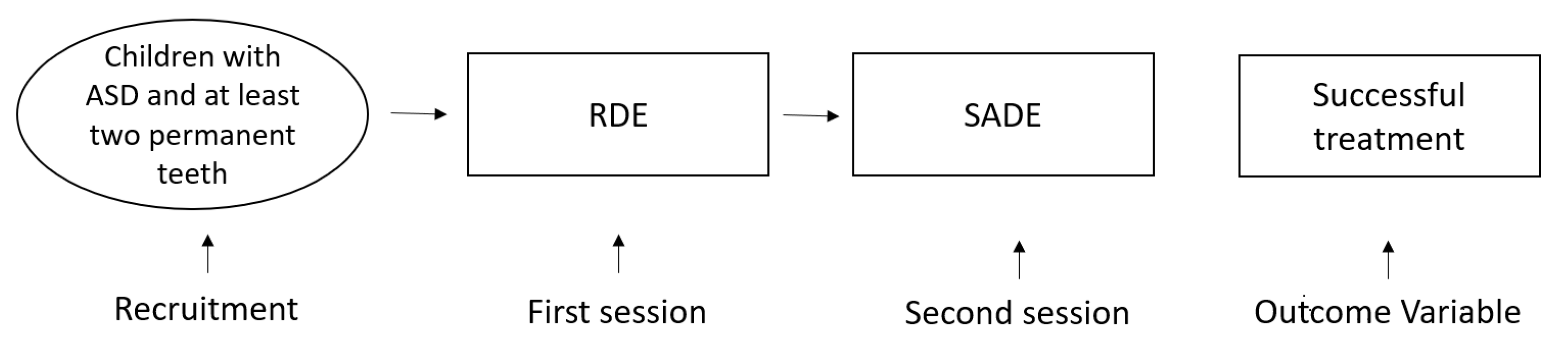
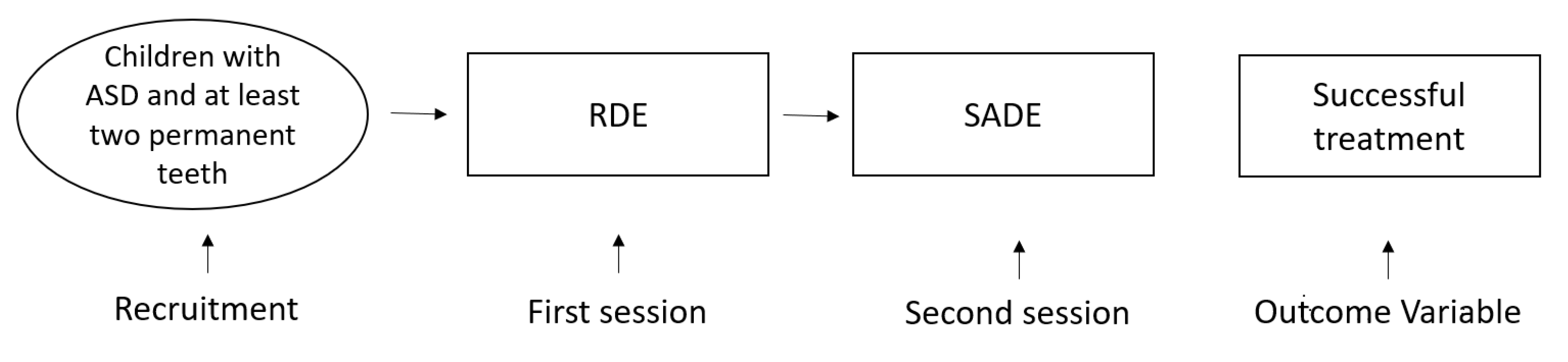
2.2. Procedures: Environment
- -
- A regular dental environment (RDE);
- -
- A sensory-adapted dental environment (SADE).
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Blomqvist, M.; Dahllöf, G.; Bejerot, S. Experiences of dental care and dental anxiety in adults with autism spectrum disorder. Autism Res. Treat. 2014, 2014, 238764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallea, A.; Zuccarello, R.; Calì, F. Dental anxiety in patients with borderline intellectual functioning and patients with intellectual disabilities. BMC Oral Health 2016, 16, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isong, I.A.; Rao, S.R.; Holifield, C.; Iannuzzi, D.; Hanson, E.; Ware, J.; Nelson, L.P. Addressing dental fear in children with autism spectrum disorders: A randomized controlled pilot study using electronic screen media. Clin. Pediatrics 2014, 53, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Cermak, S.A.; Duker, L.I.S.; Williams, M.E.; Lane, C.J.; Dawson, M.E.; Borreson, A.E.; Polido, J.C. Feasibility of a sensory-adapted dental environment for children with autism. Am. J. Occup. Ther. 2015, 69, 6903220020p1–6903220020p10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, M.; Melmed, R.N.; Sgan-Cohen, H.D.; Eli, I.; Parush, S. Behavioural and physiological effect of dental environment sensory adaptation on children’s dental anxiety. Eur. J. Oral Sci. 2007, 115, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.; Melmed, R.N.; Sgan-Cohen, H.D.; Parush, S. Effect of sensory adaptation on anxiety of children with developmental disabilities: A new approach. Pediatric Dent. 2009, 31, 222–228. [Google Scholar]
- Stein, L.I.; Lane, C.J.; Williams, M.E.; Dawson, M.E.; Polido, J.C.; Cermak, S.A. Physiological and behavioral stress and anxiety in children with autism spectrum disorders during routine oral care. BioMed Res. Int. 2014, 2014, 694876. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.M.; Sheller, B.; Friedman, C.S.; Bernier, R. Educational and therapeutic behavioral approaches to providing dental care for patients with Autism Spectrum Disorder. Spec. Care Dent. 2015, 35, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Bartolomé-Villar, B.; Mourelle-Martínez, M.R.; Diéguez-Pérez, M.; de Nova-García, M.-J. Incidence of oral health in paediatric patients with disabilities: Sensory disorders and autism spectrum disorder. Systematic review II. J. Clin. Exp. Dent. 2016, 8, e344. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.F.; Azmi, T.M.A.T.; Malek, W.M.S.W.A.; Mallineni, S.K. The effect of multisensory-adapted dental environment on children’s behavior toward dental treatment: A systematic review. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 2–8. [Google Scholar] [PubMed]
- Benedetto, L.; Cucinotta, F.; Maggio, R.; Germanò, E.; De Raco, R.; Alquino, A.; Impallomeni, C.; Siracusano, R.; Vetri, L.; Roccella, M. One-year follow-up diagnostic stability of autism spectrum disorder diagnosis in a clinical sample of children and toddlers. Brain Sci. 2021, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Schopler, E.; Reichler, R.J.; Renner, B.R. The Childhood Autism Rating Scale (CARS). Los Angeles: Western Psychological Services. J. Autism. Dev. Dis 1988, 10, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Gizzonio, V. Fenotipi Intermedi Nella Sindrome Autistica: Uno Studio del Profilo Cognitivo di un Gruppo di Fratelli di Bambini con Disturbo Dello Spettro Autistico; Università degli Studi di Parma, Dipartimento di Lettere, Arti, Storia e Società: Parma, Italy, 2014. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. ADI-R. Autism Diagnostic Interview Revised. Manual; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Como, D.H.; Stein Duker, L.I.; Polido, J.C.; Cermak, S.A. Oral health and Autism Spectrum Disorders: A unique collaboration between dentistry and occupational therapy. Int. J. Environ. Res. Public Health 2021, 18, 135. [Google Scholar] [CrossRef] [PubMed]
- Osório, J.M.A.; Rodríguez-Herreros, B.; Richetin, S.; Junod, V.; Romascano, D.; Pittet, V.; Chabane, N.; Jequier Gygax, M.; Maillard, A.M. Sex differences in sensory processing in children with autism spectrum disorder. Autism Res. 2021, 14, 2412–2423. [Google Scholar] [CrossRef] [PubMed]
- Cermak, S.A.; Duker, L.I.S.; Williams, M.E.; Dawson, M.E.; Lane, C.J.; Polido, J.C. Sensory adapted dental environments to enhance oral care for children with autism spectrum disorders: A randomized controlled pilot study. J. Autism Dev. Disord. 2015, 45, 2876–2888. [Google Scholar] [CrossRef] [PubMed]
- Case-Smith, J.; O’Brien, J.C. Occupational Therapy for Children; Mosby/Elsevier: Maryland Heights, MO, USA, 2010. [Google Scholar]
- Shapiro, M.; Sgan-Cohen, H.D.; Parush, S.; Melmed, R.N. Influence of adapted environment on the anxiety of medically treated children with developmental disability. J. Pediatrics 2009, 154, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, A.; Ganta, S.; Nagaraj, A.; Pareek, S.; Atri, M.; Singh, K.; Sidiq, M. Acoustic noise levels of dental equipments and its association with fear and annoyance levels among patients attending different dental clinic setups in Jaipur, India. J. Clin. Diagn. Res. JCDR 2014, 8, ZC29. [Google Scholar] [CrossRef] [PubMed]
- Weil, T.N.; Inglehart, M.R. Dental education and dentists’ attitudes and behavior concerning patients with autism. J. Dent. Educ. 2010, 74, 1294–1307. [Google Scholar] [CrossRef] [PubMed]
- Fux-Noy, A.; Zohar, M.; Herzog, K.; Shmueli, A.; Halperson, E.; Moskovitz, M.; Ram, D. The effect of the waiting room’s environment on level of anxiety experienced by children prior to dental treatment: A case control study. BMC Oral Health 2019, 19, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panda, A.; Garg, I.; Shah, M. Children’s preferences concerning ambiance of dental waiting rooms. Eur. Arch. Paediatr. Dent. 2015, 16, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Moana-Filho, E.J.; Alonso, A.A.; Kapos, F.P.; Leon-Salazar, V.; Durand, S.H.; Hodges, J.S.; Nixdorf, D.R. Multifactorial assessment of measurement errors affecting intraoral quantitative sensory testing reliability. Scand. J. Pain 2017, 16, 93–98. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
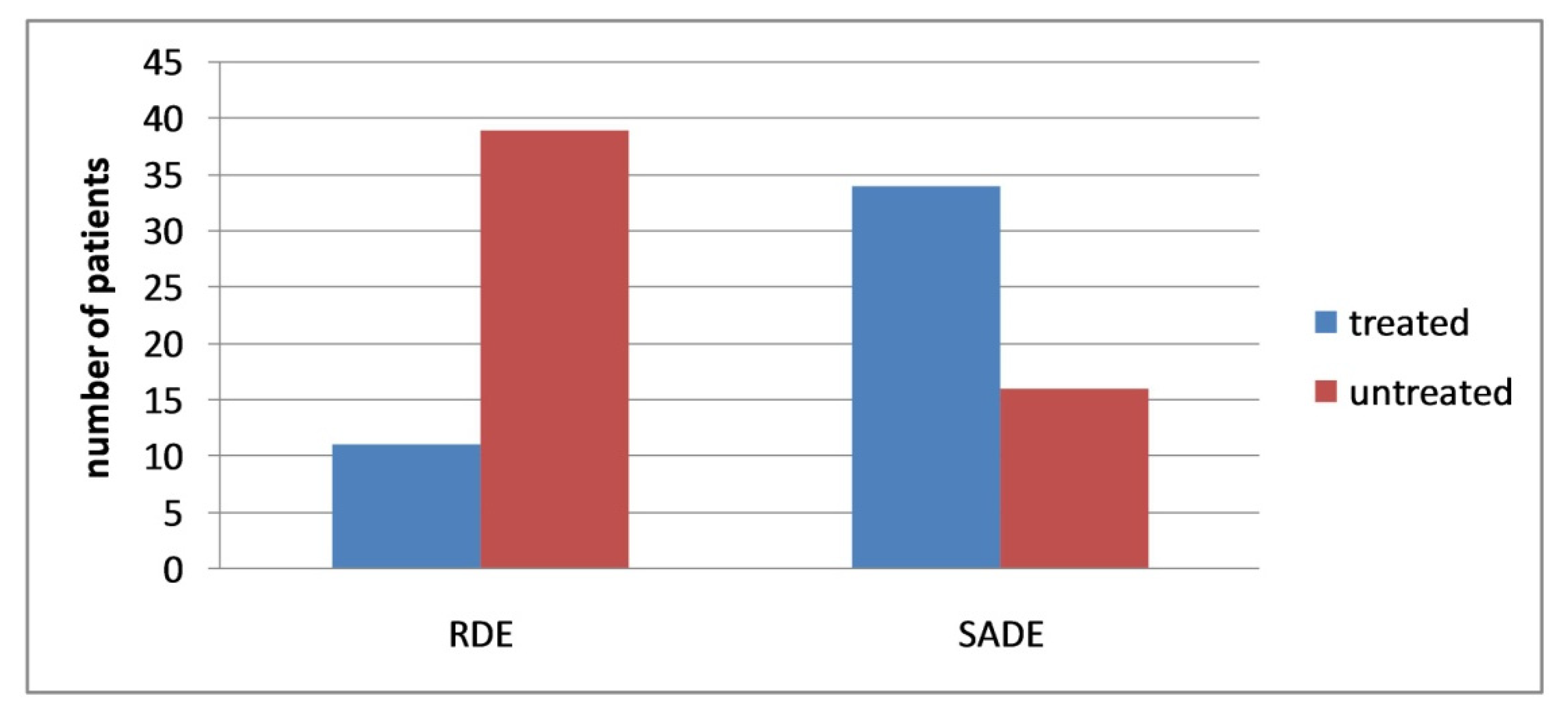
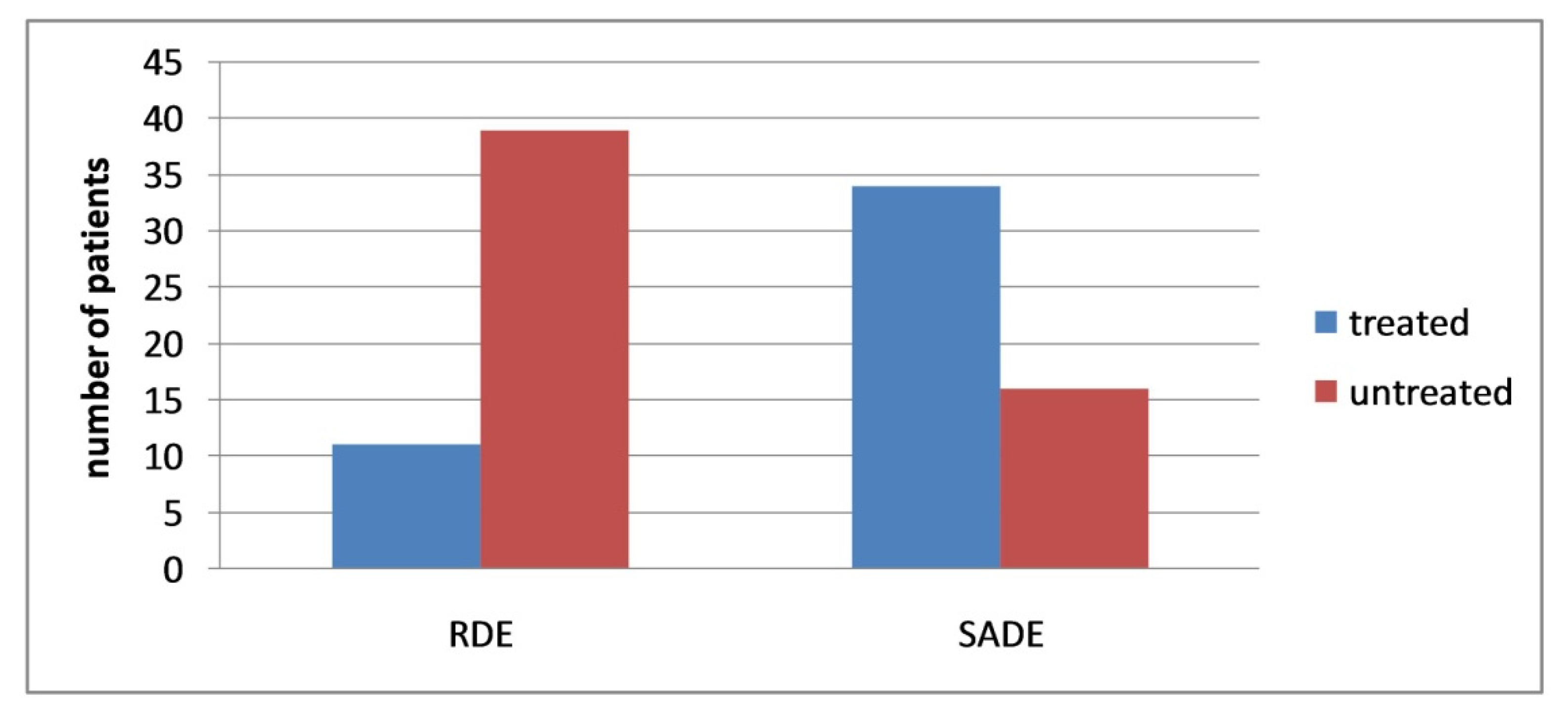
| RDE | Male | % | Female | % |
|---|---|---|---|---|
| Treated | 7 | 19.44 | 4 | 28.57 |
| Untreated | 29 | 80.56 | 10 | 71.43 |
| Tot | 36 | 100 | 14 | 100 |
| SADE | Male | % | Female | % |
| Treated | 25 | 69.44 | 9 | 64.29 |
| Untreated | 11 | 30.56 | 5 | 35.71 |
| Tot | 36 | 100 | 14 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fallea, A.; Zuccarello, R.; Roccella, M.; Quatrosi, G.; Donadio, S.; Vetri, L.; Calì, F. Sensory-Adapted Dental Environment for the Treatment of Patients with Autism Spectrum Disorder. Children 2022, 9, 393. https://doi.org/10.3390/children9030393
Fallea A, Zuccarello R, Roccella M, Quatrosi G, Donadio S, Vetri L, Calì F. Sensory-Adapted Dental Environment for the Treatment of Patients with Autism Spectrum Disorder. Children. 2022; 9(3):393. https://doi.org/10.3390/children9030393
Chicago/Turabian StyleFallea, Antonio, Rosa Zuccarello, Michele Roccella, Giuseppe Quatrosi, Serena Donadio, Luigi Vetri, and Francesco Calì. 2022. "Sensory-Adapted Dental Environment for the Treatment of Patients with Autism Spectrum Disorder" Children 9, no. 3: 393. https://doi.org/10.3390/children9030393
APA StyleFallea, A., Zuccarello, R., Roccella, M., Quatrosi, G., Donadio, S., Vetri, L., & Calì, F. (2022). Sensory-Adapted Dental Environment for the Treatment of Patients with Autism Spectrum Disorder. Children, 9(3), 393. https://doi.org/10.3390/children9030393