
Evaluation of the Versius Robotic Surgical System for Procedures in Small Cavities

 ,
, 
Abstract
:1. Introduction
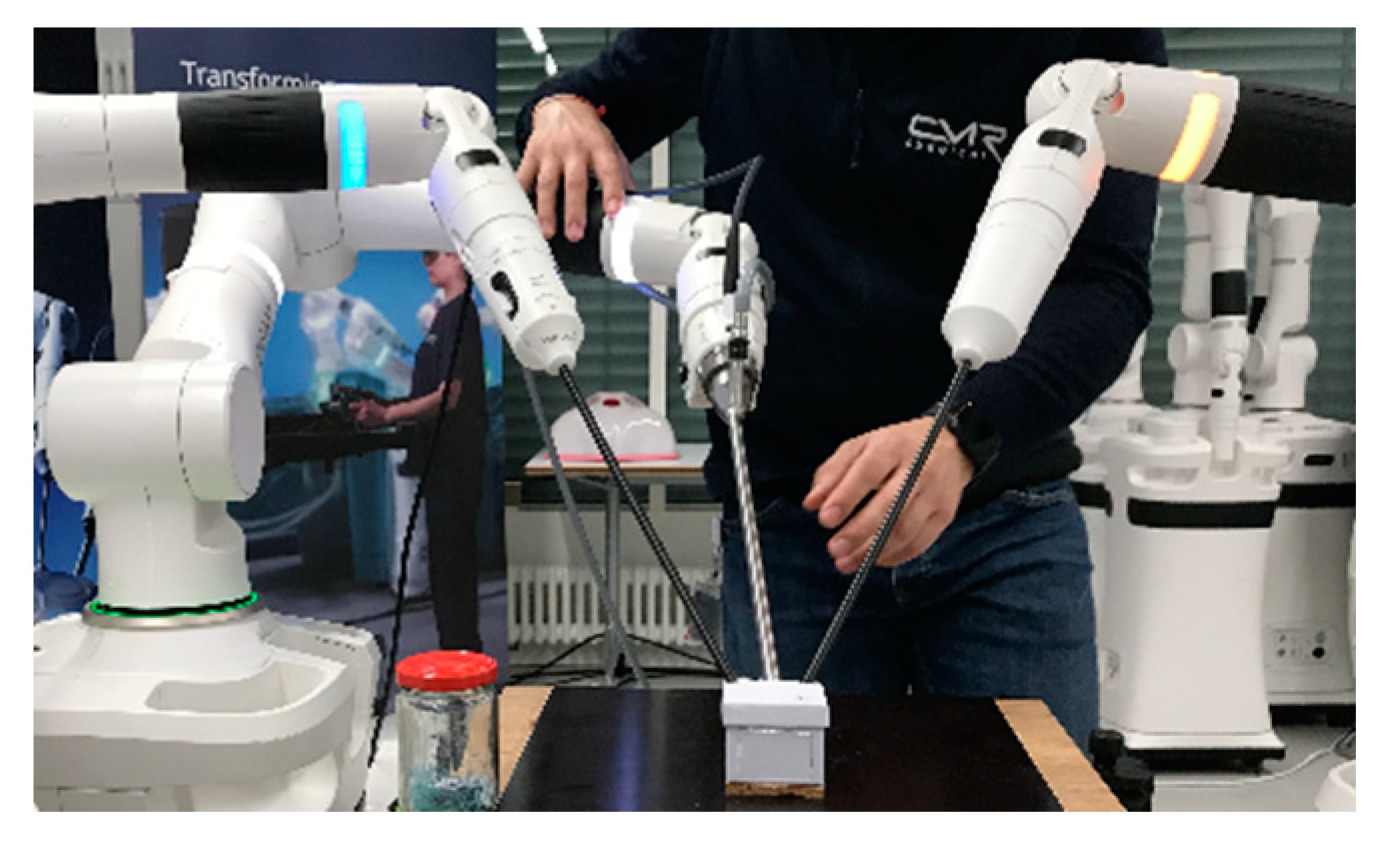
2. Materials and Methods
3. Results
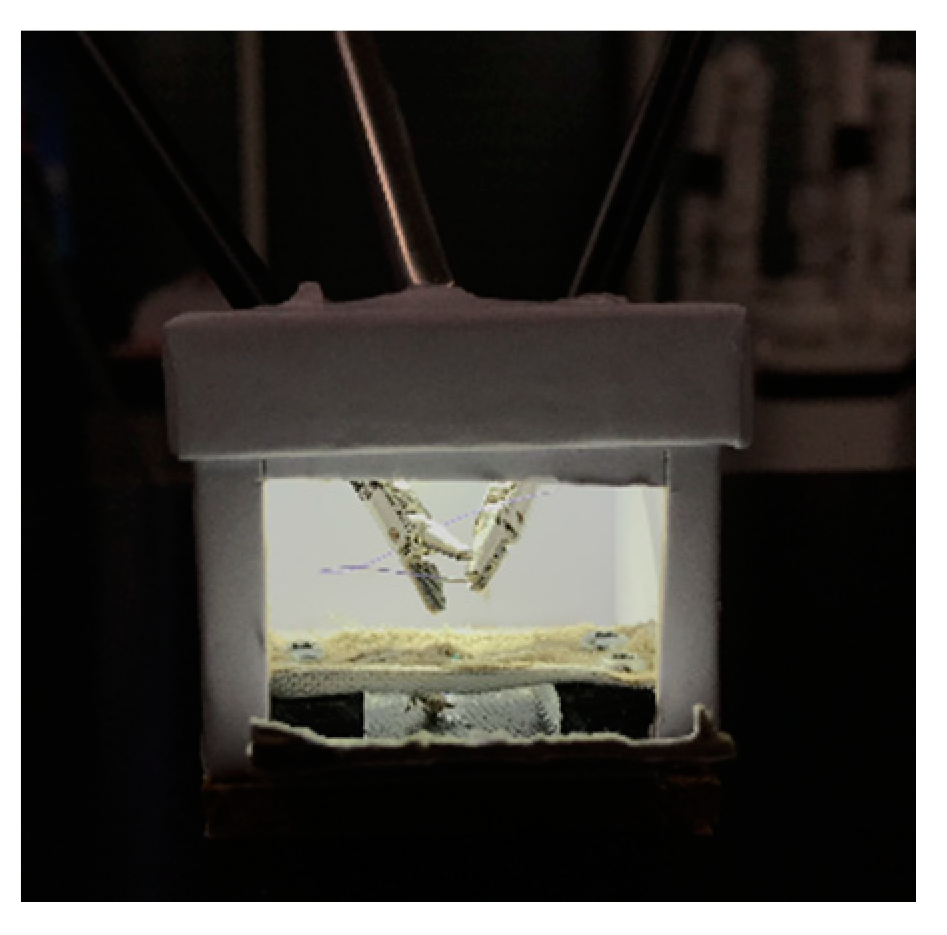
3.1. Instrumentation and Pivot Point Work-Around for Small Cavities
3.2. Procedure Time and Collisions
4. Discussion
4.1. Comparison of the Versius® System to the Senhance® and da Vinci®
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bergholz, R.; Botden, S.; Verweij, J.; Tytgat, S.; Van Gemert, W.; Boettcher, M.; Ehlert, H.; Reinshagen, K.; Gidaro, S. Evaluation of a new robotic-assisted laparoscopic surgical system for procedures in small cavities. J. Robot. Surg. 2019, 14, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Chen, W.; Wang, S.; Wang, Y. Single-site umbilical laparoscopic pyloromyotomy in neonates less than 21-day old. Surg Today 2009, 45, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Anderberg, M.; Kockum, C.C.; Arnbjornsson, E. Morgagni hernia repair in a small child using da Vinci robotic instruments--a case report. Eur. J. Pediatr. Surg. 2009, 19, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Kawal, T.; Srinivasan, A.K.; Shrivastava, D.; Chu, D.I.; Van Batavia, J.; Weiss, D.; Long, C.; Shukla, A.R. Pediatric robotic-assisted laparoscopic pyeloplasty: Does age matter? J. Pediatr Urol. 2018, 14, 540.e1–540.e6. [Google Scholar] [CrossRef] [PubMed]
- Meehan, J.J. Robotic surgery in small children: Is there room for this? J Laparoendosc Adv Surg Tech A 2009, 19, 707–712. [Google Scholar] [CrossRef] [PubMed]
- George, E.I.; Brand, T.C.; LaPorta, A.; Marescaux, J.; Satava, R.M. Origins of Robotic Surgery: From Skepticism to Standard of Care. JSLS 2018, 22, e2018.00039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballouhey, Q.; Clermidi, P.; Cros, J.; Grosos, C.; Rosa-Arsène, C.; Bahans, C.; Caire, F.; Longis, B.; Compagnon, R.; Fourcade, L. Comparison of 8 and 5 mm robotic instruments in small cavities: 5 or 8 mm robotic instruments for small cavities? Surg. Endosc. 2018, 32, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Marcus, H.J.; Hughes-Hallett, A.; Cundy, T.P.; Yang, G.-Z.; Darzi, A.; Nandi, D. da Vinci robot-assisted keyhole neurosurgery: A cadaver study on feasibility and safety. Neurosurg. Rev. 2015, 38, 367–371; discussion 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ackermann, J.; Wedel, T.; Hagedorn, H.; Maass, N.; Mettler, L.; Heinze, T.; Alkatout, I. Establishment and evaluation of a training course in advanced laparoscopic surgery based on human body donors embalmed by ethanol-glycerol-lysoformin fixation. Surg. Endosc. 2021, 35, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I.; Dhanawat, J.; Ackermann, J.; Freytag, D.; Peters, G.; Maass, N.; Mettler, L.; Pape, J.M. Video Feedback and Video Modeling in Teaching Laparoscopic Surgery: A Visionary Concept from Kiel. J. Clin. Med. 2021, 10, 163. [Google Scholar] [CrossRef] [PubMed]
- Boettcher, J.; Klippgen, L.; Mietzsch, S.; Grube, F.; Krebs, T.; Bergholz, R.; Reinshagen, K.; Boettcher, M. Spaced Education Improves the Retention of Laparoscopic Suturing Skills: A Randomized Controlled Study. Eur. J. Pediatr. Surg. 2020, 30, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Boettcher, J.; Mietzsch, S.; Wenkus, J.; Mokhaberi, N.; Klinke, M.; Reinshagen, K.; Boettcher, M. The Spaced Learning Concept Significantly Improves Acquisition of Laparoscopic Suturing Skills in Students and Residents: A Randomized Control Trial. Eur. J. Pediatr. Surg. 2021, 31, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Boettcher, M.; Boettcher, J.; Mietzsch, S.; Krebs, T.; Bergholz, R.; Reinshagen, K. The spaced learning concept significantly improves training for laparoscopic suturing: A pilot randomized controlled study. Surg. Endosc. 2018, 32, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.C.; Slack, M.; Hussain, M.; Barber, N.; Pradhan, A.; Dinneen, E.; Stewart, G.D. Preclinical Evaluation of the Versius Surgical System, a New Robot-assisted Surgical Device for Use in Minimal Access Renal and Prostate Surgery. Eur. Urol. Focus 2021, 7, 444–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakre, A.A.; Bailly, Y.; Sun, L.W.; Van Meer, F.; Yeung, C.K. Is smaller workspace a limitation for robot performance in laparoscopy? J. Urol. 2008, 179, 1138–1142; discussion 1142–1143. [Google Scholar] [CrossRef] [PubMed]
- Van Haasteren, G.; Levine, S.; Hayes, W. Pediatric Robotic Surgery: Early Assessment. Pediatrics 2009, 124, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- Krauss, A.; Neumuth, T.; Wachowiak, R.; Donaubauer, B.; Korb, W.; Burgert, O.; Muensterer, O.J. Laparoscopic versus robot-assisted Nissen fundoplication in an infant pig model. Pediatr. Surg. Int. 2012, 28, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Krebs, T.F.; Egberts, J.-H.; Lorenzen, U.; Krause, M.F.; Reischig, K.; Meiksans, R.; Baastrup, J.; Meinzer, A.; Alkatout, I.; Cohrs, G.; et al. Robotic infant surgery with 3 mm instruments: A study in piglets of less than 10 kg body weight. J. Robot. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Chapman, B.; O’Callaghan, C.; Coxon, R.; Glover, P.; Jaroszkiewicz, G.; Howseman, A.; Mansfield, P.; Small, P.; Milner, A.D.; Coupland, R.E. Estimation of lung volume in infants by echo planar imaging and total body plethysmography. Arch. Dis. Child. 1990, 65, 168–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
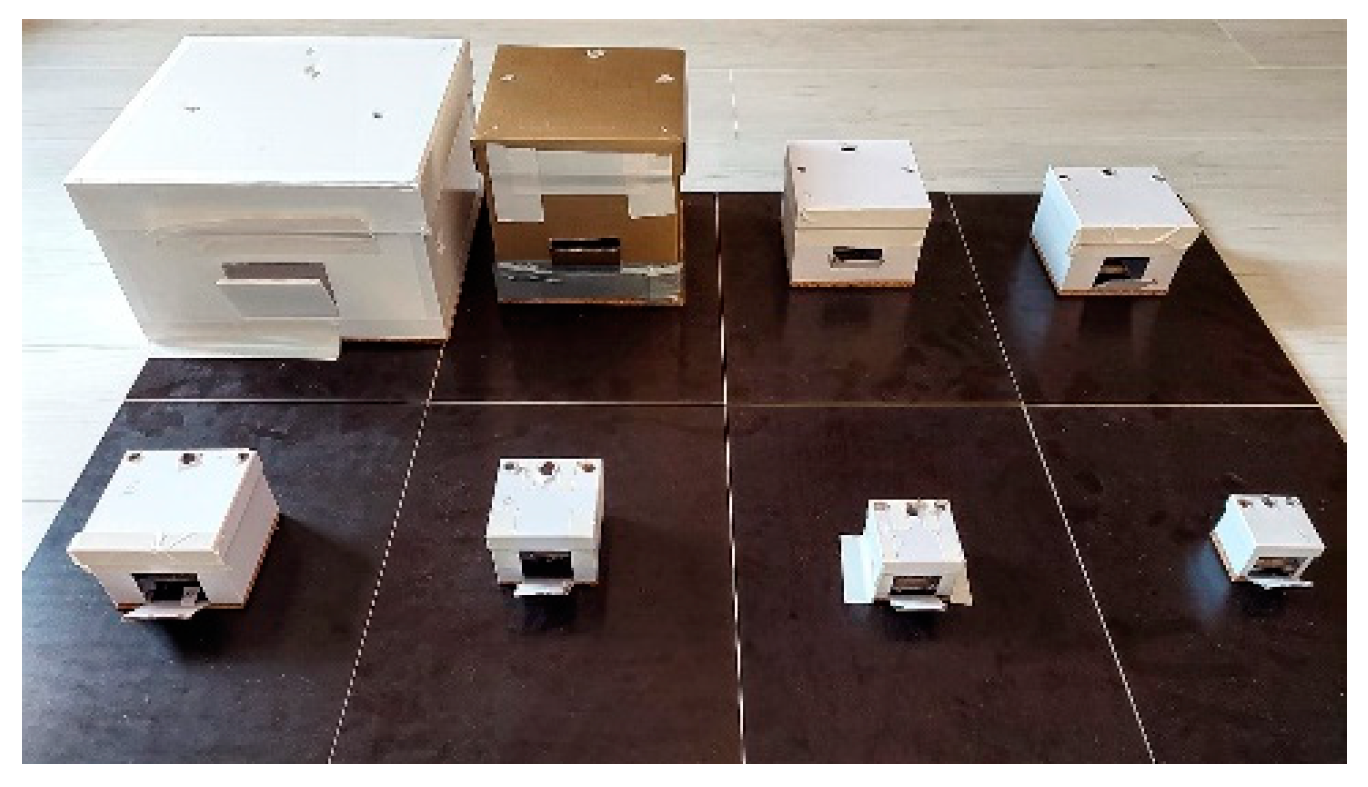
| Box No. | Width (cm) | Height (cm) | Depth (cm) | Volume * | ΔLC (cm) | ΔRC (cm) | ΔLR (cm) |
|---|---|---|---|---|---|---|---|
| 1 | 17.5 | 30 | 30 | 15.75 L | 13 | 12.5 | 19 |
| 2 | 18.5 | 19.5 | 19.5 | 7.04 L | 10 | 11.5 | 17 |
| 3 | 13.9 | 13.9 | 9.7 | 1.87 L | 8 | 8 | 12.5 |
| 4 | 8.6 | 11.9 | 11.9 | 1.22 L | 5.5 | 5.5 | 11 |
| 5 | 7.4 | 9.9 | 9.9 | 725 mL | 4.5 | 4.5 | 9 |
| 6 | 6.2 | 7.9 | 7.9 | 387 mL | 4 | 3.5 | 7 |
| 7 | 5 | 5.9 | 5.9 | 174 mL | 2.5 | 2.5 | 5 |
| 8 | 4.4 | 4.9 | 4.9 | 106 mL | 2.5 | 2.4 | 4.5 |
| Box | Median Procedure Time (Sec) | Shortest Procedure Time (Sec) | Longest Procedure Time (Sec) | Internal Instrument/Instrument Collisions per Knot | Internal Instrument/Box Collisions per Knot | External Instrument/Instrument Collisions per Knot | |
|---|---|---|---|---|---|---|---|
| Versius inexperienced Surgeons (n = 6) | 1 | 264.5 | 177.0 | 489.0 | 5.42 | 0.42 | 0 |
| 2 | 203 | 92.0 | 283.0 | 5.25 | 0.75 | 0 | |
| 3 | 162.5 | 64.0 | 248.0 | 4.4 | 0.2 | 0 | |
| 4 | 151 | 132.0 | 179.0 | 4.7 | 0.8 | 0 | |
| 5 | 228.5 | 107.0 | 304.0 | 7.11 | 0.78 | 0.44 | |
| 6 | 250 | 134.0 | 425.0 | 5.82 | 0.55 | 0.73 | |
| 7 | 252 | 183.0 | 380.0 | 4.17 | 1.33 | 1.17 | |
| 8 | 307 | 176.0 | 666.0 | 7.36 | 2.55 | 1.82 | |
| Versius experienced Surgeon (n = 1) | 1 | 215.5 | 181.0 | 250.0 | 0 | 0 | 0 |
| 2 | 108.0 | 90.0 | 126.0 | 1.50 | 0 | 0 | |
| 3 | 88.5 | 86.0 | 91.0 | 0 | 0 | 0 | |
| 4 | 108.0 | 85.0 | 131.0 | 1 | 0 | 0 | |
| 5 | 105.5 | 93.0 | 118.0 | 1 | 1.50 | 0 | |
| 6 | 154.0 | 120.0 | 188.0 | 2.50 | 1 | 0 | |
| 7 | 166.0 | 148.0 | 184.0 | 0.50 | 0 | 2.5 | |
| 8 | 200.0 | 190.0 | 210.0 | 0.50 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kayser, M.; Krebs, T.F.; Alkatout, I.; Kayser, T.; Reischig, K.; Baastrup, J.; Meinzer, A.; Ulrich, K.; Osmonov, D.; Bergholz, R. Evaluation of the Versius Robotic Surgical System for Procedures in Small Cavities. Children 2022, 9, 199. https://doi.org/10.3390/children9020199
Kayser M, Krebs TF, Alkatout I, Kayser T, Reischig K, Baastrup J, Meinzer A, Ulrich K, Osmonov D, Bergholz R. Evaluation of the Versius Robotic Surgical System for Procedures in Small Cavities. Children. 2022; 9(2):199. https://doi.org/10.3390/children9020199
Chicago/Turabian StyleKayser, Marit, Thomas Franz Krebs, Ibrahim Alkatout, Timo Kayser, Katja Reischig, Jonas Baastrup, Andreas Meinzer, Katja Ulrich, Daniar Osmonov, and Robert Bergholz. 2022. "Evaluation of the Versius Robotic Surgical System for Procedures in Small Cavities" Children 9, no. 2: 199. https://doi.org/10.3390/children9020199
APA StyleKayser, M., Krebs, T. F., Alkatout, I., Kayser, T., Reischig, K., Baastrup, J., Meinzer, A., Ulrich, K., Osmonov, D., & Bergholz, R. (2022). Evaluation of the Versius Robotic Surgical System for Procedures in Small Cavities. Children, 9(2), 199. https://doi.org/10.3390/children9020199