
Burden of Respiratory Syncytial Virus Related Acute Lower Respiratory Tract Infection in Hospitalized Thai Children: A 6-Year National Data Analysis

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collections
2.3. Statistical Analyses
3. Results
3.1. Demographics Data
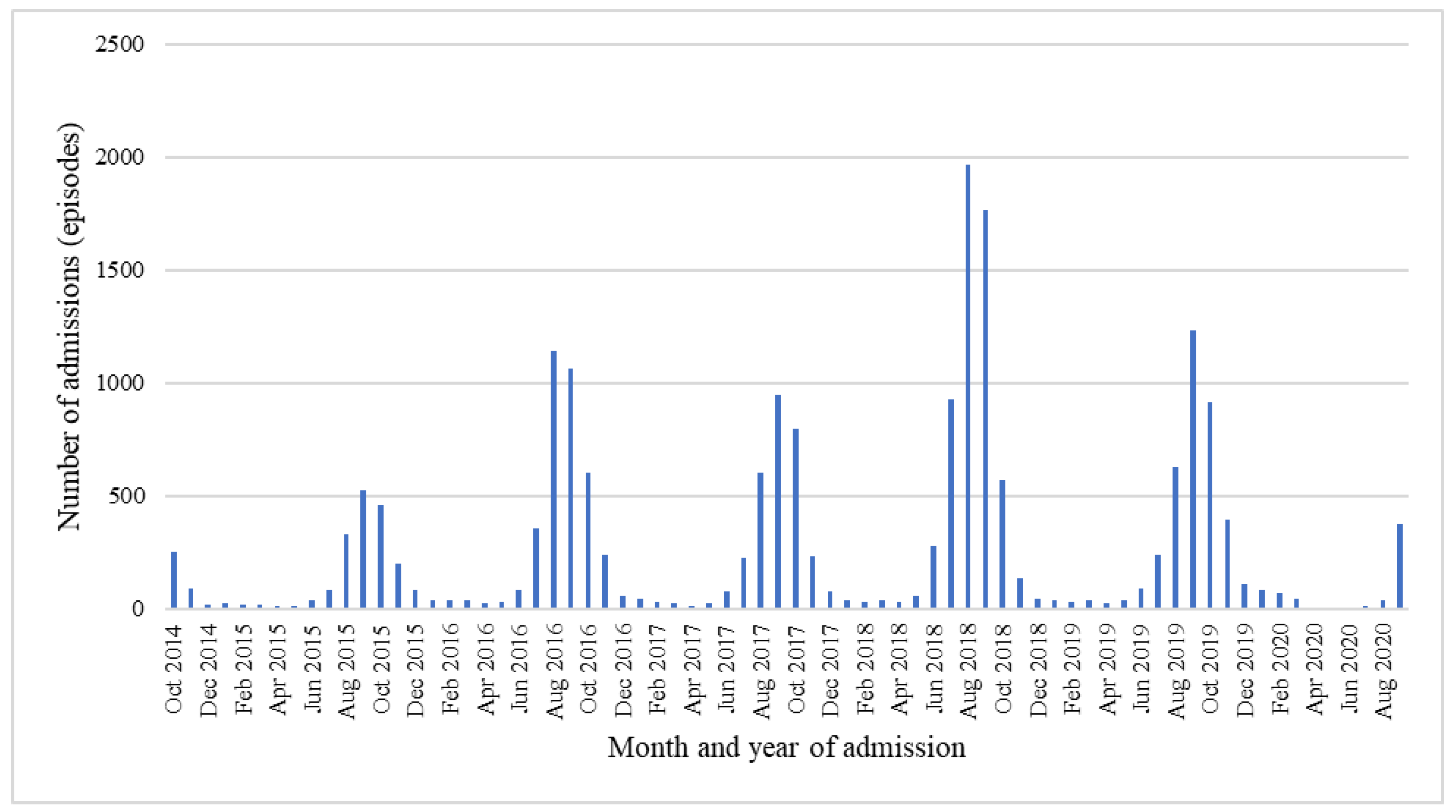
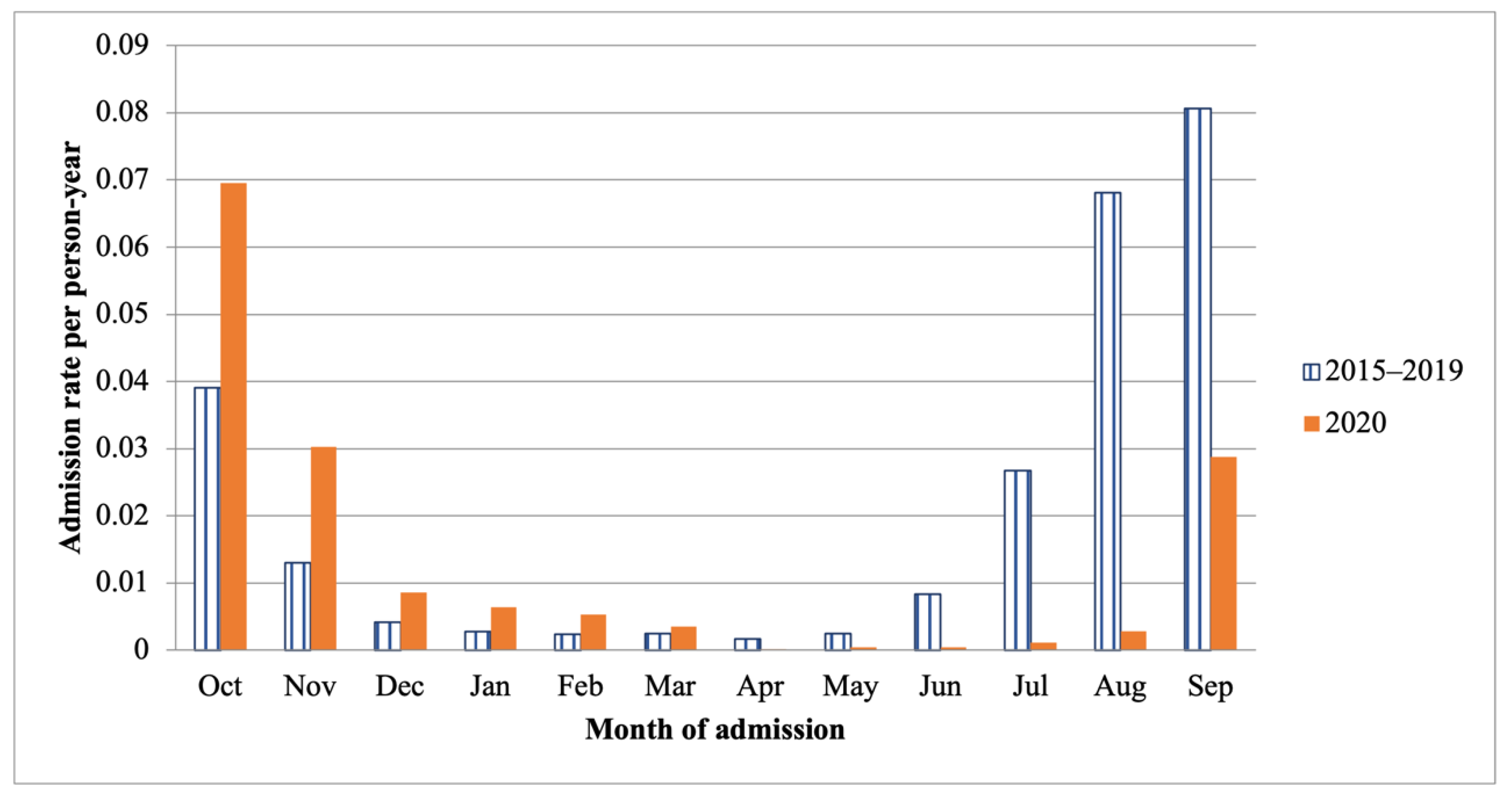
3.2. Annual Trend of Admission
3.3. Outcome of Treatment
3.4. Respiratory Failure Required Intubation
3.5. RSV-Related LRTI Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collins, P.L.; Fearns, R.; Graham, B.S. Respiratory Syncytial Virus: Virology, Reverse Genetics, and Pathogenesis of Disease. Curr. Top Microbiol. Immunol. 2013, 372, 3–38. [Google Scholar] [CrossRef] [PubMed]
- Florin, T.A.; Plint, A.C.; Zorc, J.J. Viral bronchiolitis. Lancet 2017, 389, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B.; Weinberg, G.A.; Iwane, M.K.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Auinger, P.; Griffin, M.R.; Poehling, K.A.; Erdman, D.; et al. The Burden of Respiratory Syncytial Virus Infection in Young Children. N. Engl. J. Med. 2009, 360, 588–598. [Google Scholar] [CrossRef]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef]
- Li, X.; Willem, L.; Antillon, M.; Bilcke, J.; Jit, M.; Beutels, P. Health and Economic Burden of Respiratory Syncytial Virus (RSV) Disease and the Cost-Effectiveness of Potential Interventions against RSV among Children under 5 Years in 72 Gavi-Eligible Countries. BMC Med. 2020, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Haddadin, Z.; Beveridge, S.; Fernandez, K.; Rankin, D.A.; Probst, V.; Spieker, A.J.; Markus, T.M.; Stewart, L.S.; Schaffner, W.; Lindegren, M.L.; et al. Respiratory Syncytial Virus Disease Severity in Young Children. Clin. Infect. Dis. 2020, 73, e4384–e4391. [Google Scholar] [CrossRef] [PubMed]
- Bunthi, C.; Rhodes, J.; Thamthitiwat, S.; Higdon, M.M.; Chuananon, S.; Amorninthapichet, T.; Paveenkittiporn, W.; Chittaganpitch, M.; Sawatwong, P.; Hammitt, L.L.; et al. Etiology and Clinical Characteristics of Severe Pneumonia Among Young Children in Thailand. Pediatr. Infect. Dis. J. 2021, 40, S91–S100. [Google Scholar] [CrossRef]
- Teeratakulpisarn, J.; Uppala, R.; Thepsuthammarat, K.; Sutra, S. Burden of Acute Lower Respiratory Infection in Children in Thailand in 2010: Have We Achieved the National Target in Under-Five Morbidity and Mortality? J. Med. Assoc. Thail. 2012, 95, 10. [Google Scholar]
- Sumriddetchkajorn, K.; Shimazaki, K.; Ono, T.; Kusaba, T.; Sato, K.; Kobayashi, N. Universal Health Coverage and Primary Care, Thailand. Bull. World Health Organ. 2019, 97, 415–422. [Google Scholar] [CrossRef]
- van Summeren, J.; Meijer, A.; Aspelund, G.; Casalegno, J.S.; Erna, G.; Hoang, U.; Lina, B.; VRS Study Group in Lyon; de Lusignan, S.; Teirlinck, A.C.; et al. Low Levels of Respiratory Syncytial Virus Activity in Europe during the 2020/21 Season: What Can We Expect in the Coming Summer and Autumn/Winter? Euro Surveill. 2021, 26, 2100639. [Google Scholar] [CrossRef]
- Rybak, A.; Levy, C.; Angoulvant, F.; Auvrignon, A.; Gembara, P.; Danis, K.; Vaux, S.; Levy-Bruhl, D.; van der Werf, S.; Béchet, S.; et al. Association of Nonpharmaceutical Interventions During the COVID-19 Pandemic with Invasive Pneumococcal Disease, Pneumococcal Carriage, and Respiratory Viral Infections Among Children in France. JAMA Netw. Open 2022, 5, e2218959. [Google Scholar] [CrossRef]
- O’Brien, K.L.; Baggett, H.C.; Brooks, W.A.; Feikin, D.R.; Hammitt, L.L.; Higdon, M.M.; Howie, S.R.C.; Knoll, M.D.; Kotloff, K.L.; Levine, O.S.; et al. Causes of Severe Pneumonia Requiring Hospital Admission in Children without HIV Infection from Africa and Asia: The PERCH Multi-Country Case-Control Study. Lancet 2019, 394, 757–779. [Google Scholar] [CrossRef] [PubMed]
- Naorat, S.; Chittaganpitch, M.; Thamthitiwat, S.; Henchaichon, S.; Sawatwong, P.; Srisaengchai, P.; Lu, Y.; Chuananon, S.; Amornintapichet, T.; Chantra, S.; et al. Hospitalizations for Acute Lower Respiratory Tract Infection Due to Respiratory Syncytial Virus in Thailand, 2008–2011. J. Infect. Dis. 2013, 208 (Suppl. S3), S238–S245. [Google Scholar] [CrossRef] [PubMed]
- Pensaengon, K. Tackling Thailand’s Middle-Income Trap by Entrepreneur Society. Humanit. Arts Soc. Sci. Stud. 2022, 22, 227–234. [Google Scholar]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Children Younger than 5 Years in 2019: A Systematic Analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Staadegaard, L.; Caini, S.; Wangchuk, S.; Thapa, B.; de Almeida, W.A.F.; de Carvalho, F.C.; Fasce, R.A.; Bustos, P.; Kyncl, J.; Novakova, L.; et al. Defining the Seasonality of Respiratory Syncytial Virus around the World: National and Subnational Surveillance Data from 12 Countries. Influenza Other Respir. Viruses 2021, 15, 732–741. [Google Scholar] [CrossRef]
- Aikphaibul, P.; Theerawit, T.; Sophonphan, J.; Wacharachaisurapol, N.; Jitrungruengnij, N.; Puthanakit, T. Risk Factors of Severe Hospitalized Respiratory Syncytial Virus Infection in Tertiary Care Center in Thailand. Influenza Other Respir. Viruses 2021, 15, 64–71. [Google Scholar] [CrossRef]
- Kamigaki, T.; Chaw, L.; Tan, A.G.; Tamaki, R.; Alday, P.P.; Javier, J.B.; Olveda, R.M.; Oshitani, H.; Tallo, V.L. Seasonality of Influenza and Respiratory Syncytial Viruses and the Effect of Climate Factors in Subtropical–Tropical Asia Using Influenza-Like Illness Surveillance Data, 2010–2012. PLoS ONE 2016, 11, e167712. [Google Scholar] [CrossRef]
- Paynter, S.; Yakob, L.; Simões, E.A.F.; Lucero, M.G.; Tallo, V.; Nohynek, H.; Ware, R.S.; Weinstein, P.; Williams, G.; Sly, P.D. Using Mathematical Transmission Modelling to Investigate Drivers of Respiratory Syncytial Virus Seasonality in Children in the Philippines. PLoS ONE 2014, 9, e90094. [Google Scholar] [CrossRef]
- Chan, P.W.K.; Chew, F.T.; Tan, T.N.; Chua, K.B.; Hooi, P.S. Seasonal Variation in Respiratory Syncytial Virus Chest Infection in the Tropics. Pediatr. Pulmonol. 2002, 34, 47–51. [Google Scholar] [CrossRef]
- Pica, N.; Bouvier, N.M. Environmental Factors Affecting the Transmission of Respiratory Viruses. Curr. Opin. Virol. 2012, 2, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Paynter, S. Humidity and Respiratory Virus Transmission in Tropical and Temperate Settings. Epidemiol. Infect. 2015, 143, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Wilkesmann, A.; Ammann, R.A.; Schildgen, O.; Eis-Hübinger, A.M.; Müller, A.; Seidenberg, J.; Stephan, V.; Rieger, C.; Herting, E.; Wygold, T.; et al. Hospitalized Children with Respiratory Syncytial Virus Infection and Neuromuscular Impairment Face an Increased Risk of a Complicated Course. Pediatr. Infect. Dis. J. 2007, 26, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Heppe-Montero, M.; Walter, S.; Hernández-Barrera, V.; Gil-Prieto, R.; Gil-de-Miguel, Á. Burden of Respiratory Syncytial Virus-Associated Lower Respiratory Infections in Children in Spain from 2012 to 2018. BMC Infect. Dis. 2022, 22, 315. [Google Scholar] [CrossRef] [PubMed]
- Brady, M.T.; Byington, C.L.; Davies, H.D.; Edwards, K.M.; Jackson, M.A.; Maldonado, Y.A.; Murray, D.L.; Orenstein, W.A.; Rathore, M.H.; Sawyer, M.H.; et al. Updated Guidance for Palivizumab Prophylaxis Among Infants and Young Children at Increased Risk of Hospitalization for Respiratory Syncytial Virus Infection. Pediatrics 2014, 134, 415–420. [Google Scholar] [CrossRef]
- Anderson, E.J.; Carosone-Link, P.; Yogev, R.; Yi, J.; Simões, E.A.F. Effectiveness of Palivizumab in High-Risk Infants and Children: A Propensity Score Weighted Regression Analysis. Pediatr. Infect. Dis. J. 2017, 36, 699–704. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ICD-10 TM | J12.1 | J21.0 | J20.5 | Total |
|---|---|---|---|---|
| Principal Diagnosis | RSV Pneumonia (N = 13,684) | Acute Bronchiolitis Due to RSV (N = 2849) | Acute Bronchitis Due to RSV (N = 2807) | (N = 19,340) |
| Fiscal year, No. (%) | ||||
| 2015 | 969 (7.08) | 187 (6.66) | 283 (9.93) | 1439 (7.44) |
| 2016 | 2499 (18.26) | 514 (18.31) | 558 (19.59) | 3571 (18.46) |
| 2017 | 2062 (15.07) | 385 (13.72) | 454 (15.94) | 2901 (15.00) |
| 2018 | 4460 (32.59) | 964 (34.34) | 822 (28.85) | 6246 (32.30) |
| 2019 | 2196 (16.05) | 474 (16.89) | 452 (15.87) | 3122 (16.14) |
| 2020 | 1498 (10.95) | 283 (10.08) | 280 (9.83) | 2061 (10.66) |
| Gender, No. (%) | ||||
| Male | 7854 (57.4) | 1573 (56.04) | 1715 (61.1) | 11,142 (57.61) |
| Female | 5830 (42.6) | 1276 (43.96) | 1092 (38.9) | 8198 (42.39) |
| Age group, No. (%) | ||||
| <1 year | 6798 (49.68) | 1056 (37.62) | 1481 (51.98) | 9335 (48.27) |
| 1-<5 years | 6641 (48.53) | 1622 (57.78) | 1318 (46.26) | 9581 (49.54) |
| 5-<18 years | 245 (1.79) | 129 (4.6) | 50 (1.76) | 424 (2.19) |
| Level of hospital, No. (%) | ||||
| Primary | 889 (6.5) | 187 (6.66) | 117 (4.11) | 1193 (6.17) |
| Secondary | 2944 (21.51) | 865 (30.82) | 1462 (51.32) | 5271 (27.26) |
| Tertiary | 8368 (61.15) | 1134 (40.4) | 1118 (39.24) | 10,620 (54.91) |
| Private | 1483 (10.84) | 621 (22.12) | 152 (5.34) | 2256 (11.66) |
| Age Group (Years) | Admission | Mortality | ||
|---|---|---|---|---|
| Number | Admission Rate (/1000 Person Time) | Number | Mortality Rate (/100,000 Person Time) | |
| <1 | 9335 | 2.60 | 65 | 1.75 |
| 1–<5 | 9581 | 0.58 | 35 | 0.21 |
| 5–<18 | 424 | 0.01 | 6 | 0.01 |
| Fiscal Year | Number of Admissions | Admission Rate /1000 People |
|---|---|---|
| 2015 | 1439 | 0.10 |
| 2016 | 3571 | 0.26 |
| 2017 | 2901 | 0.21 |
| 2018 | 6246 | 0.46 |
| 2019 | 3122 | 0.23 |
| 2020 | 2061 | 0.16 |
| Number of Intubations N, (%) | Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|---|
| Crude OR | 95%CI | p-Value | Adjusted OR | 95%CI | p-Value | ||
| Chronic respiratory disease | |||||||
| No | 1283 (96.39) | 1 | - | 1 | - | ||
| Yes | 48 (3.61) | 1.56 | 1.15–2.12 | 0.004 | 1.67 | 1.20–2.32 | 0.002 |
| Congenital heart disease | |||||||
| No | 1130 (84.90) | 1 | - | 1 | - | ||
| Yes | 201 (15.10) | 8.44 | 7.01–10.17 | <0.001 | 5.19 | 4.22–6.40 | <0.001 |
| Hematologic malignancy | |||||||
| No | 1318 (99.02) | 1 | - | 1 | - | ||
| Yes | 13 (0.08) | 1.82 | 1.02–3.27 | 0.044 | 1.31 | 0.70–2.46 | 0.397 |
| Malnutrition | |||||||
| No | 1279 (96.09) | 1 | - | 1 | - | ||
| Yes | 52 (3.91) | 7.01 | 4.99–9.88 | <0.001 | 3.02 | 1.99–4.59 | <0.001 |
| Neurological disease | |||||||
| No | 1302 (97.82) | 1 | - | 1 | - | ||
| Yes | 29 (2.18) | 4.16 | 2.73–6.34 | <0.001 | 2.57 | 1.55–4.29 | <0.001 |
| Number of Deaths N, (%) | Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|---|
| Crude OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | ||
| Congenital heart disease | |||||||
| No | 70 (66.04) | 1 | - | 1 | - | ||
| Yes | 36 (33.96) | 17.89 | 11.86–27.00 | <0.001 | 10.09 | 6.21–16.37 | <0.001 |
| Hematologic malignancy | |||||||
| No | 98 (92.45) | 1 | - | 1 | - | ||
| Yes | 8 (7.55) | 15.30 | 7.24–32.33 | <0.001 | 10.34 | 4.17–25.63 | <0.001 |
| Malnutrition | |||||||
| No | 100 (94.34) | 1 | - | 1 | - | ||
| Yes | 6 (5.66) | 7.63 | 3.29–17.67 | <0.001 | 1.52 | 0.54–4.32 | 0.428 |
| Neurological disease | |||||||
| No | 102 (96.23) | 1 | - | 1 | - | ||
| Yes | 4 (3.77) | 6.19 | 2.24–17.10 | <0.001 | 3.50 | 1.13–10.89 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sitthikarnkha, P.; Uppala, R.; Niamsanit, S.; Sutra, S.; Thepsuthammarat, K.; Techasatian, L.; Niyomkarn, W.; Teeratakulpisarn, J. Burden of Respiratory Syncytial Virus Related Acute Lower Respiratory Tract Infection in Hospitalized Thai Children: A 6-Year National Data Analysis. Children 2022, 9, 1990. https://doi.org/10.3390/children9121990
Sitthikarnkha P, Uppala R, Niamsanit S, Sutra S, Thepsuthammarat K, Techasatian L, Niyomkarn W, Teeratakulpisarn J. Burden of Respiratory Syncytial Virus Related Acute Lower Respiratory Tract Infection in Hospitalized Thai Children: A 6-Year National Data Analysis. Children. 2022; 9(12):1990. https://doi.org/10.3390/children9121990
Chicago/Turabian StyleSitthikarnkha, Phanthila, Rattapon Uppala, Sirapoom Niamsanit, Sumitr Sutra, Kaewjai Thepsuthammarat, Leelawadee Techasatian, Watit Niyomkarn, and Jamaree Teeratakulpisarn. 2022. "Burden of Respiratory Syncytial Virus Related Acute Lower Respiratory Tract Infection in Hospitalized Thai Children: A 6-Year National Data Analysis" Children 9, no. 12: 1990. https://doi.org/10.3390/children9121990
APA StyleSitthikarnkha, P., Uppala, R., Niamsanit, S., Sutra, S., Thepsuthammarat, K., Techasatian, L., Niyomkarn, W., & Teeratakulpisarn, J. (2022). Burden of Respiratory Syncytial Virus Related Acute Lower Respiratory Tract Infection in Hospitalized Thai Children: A 6-Year National Data Analysis. Children, 9(12), 1990. https://doi.org/10.3390/children9121990