
Grouping of Ankyloglossia According to Coryllos Anatomical Classification and Follow-Up Results for Breastfeeding: Single-Center, Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Plan
2.2. Neonatal Follow-Up Protocol for Ankyloglossia
2.3. Frenotomy Procedure
2.4. Statistical Analysis
3. Results
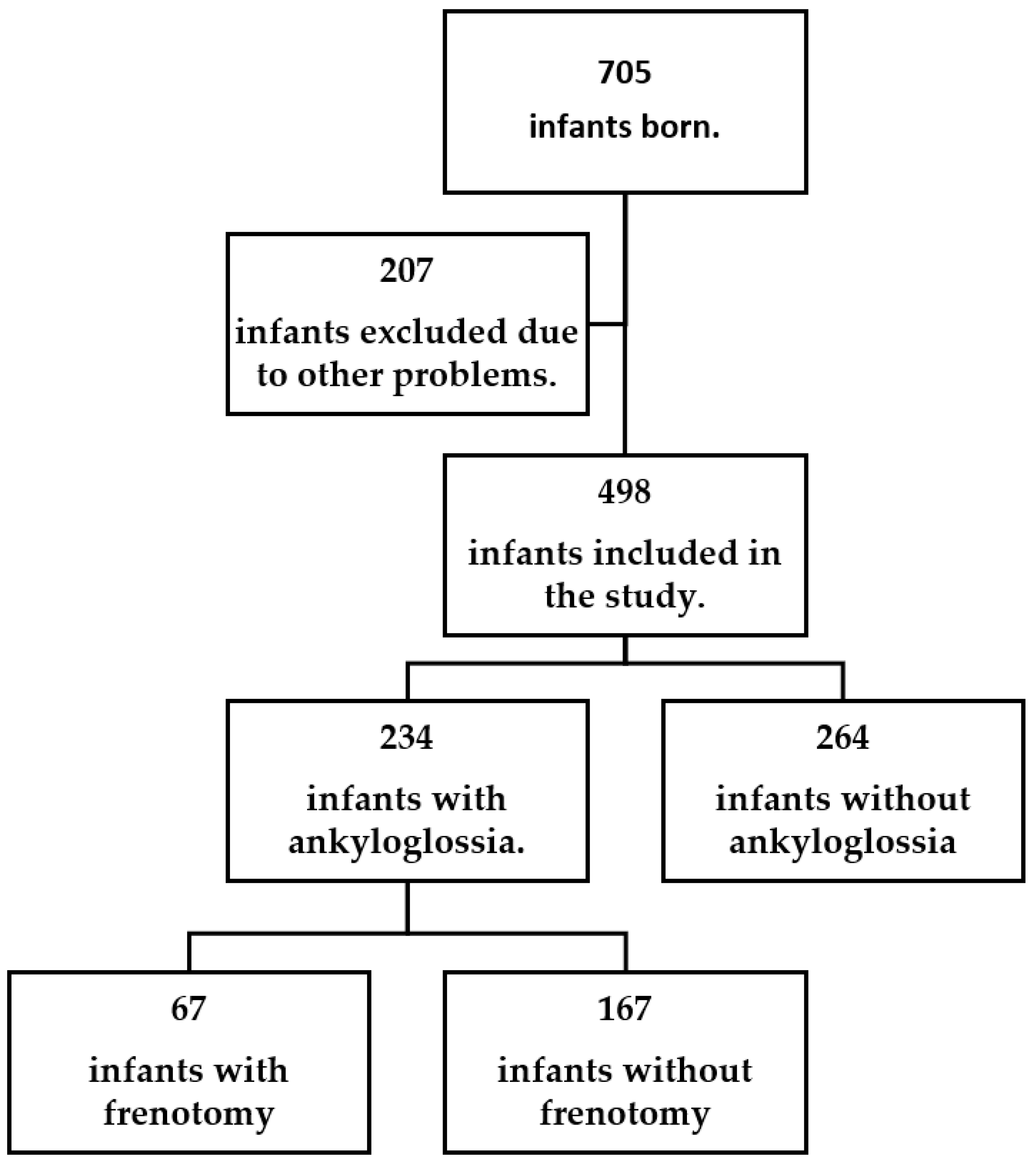
3.1. The Study Group in General
3.2. Ankyloglossia Baby Group
4. Discussion
5. Conclusions
- With screening programs, it will be seen that ankyloglossia is more common than the general literature shows.
- Frenotomy can be performed without delay in patients with ankyloglossia and breastfeeding problems.
- Frenotomy give successful results.
- If difficulties in breastfeeding are noticed in ankyloglossia patients even at the first control, the frenotomy procedure should be recommended in clinical conditions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Messner, A.H.; Walsh, J.; Rosenfeld, R.M.; Schwartz, S.R.; Ishman, S.L.; Baldassari, C.; Brietzke, S.E.; Darrow, D.H.; Goldstein, N.; Levi, J.; et al. Clinical Consensus Statement: Ankyloglossia in Children. Otolaryngol. Head Neck Surg. 2020, 162, 597–611. [Google Scholar] [CrossRef] [PubMed]
- Mills, N.; Pransky, S.M.; Geddes, D.T.; Mirjalili, S.A. What is a tongue tie? Defining the anatomy of the in-situ lingual frenulum. Clin. Anat. 2019, 32, 749–761. [Google Scholar] [CrossRef] [PubMed]
- Dezio, M.; Piras, A.; Gallottini, L.; Denotti, G. Tongue-Tie, from Embriology to Treatment: A Literature Review. J. Pediatr. Neonat. Individ. Med. 2015, 4, e040101. [Google Scholar] [CrossRef]
- Walsh, J.; Links, A.; Boss, E.; Tunkel, D. Ankyloglossia and Lingual Frenotomy: National Trends in Inpatient Diagnosis and Management in the United States, 1997–2012. Otolaryngol. Head Neck Surg. 2017, 156, 735–740. [Google Scholar] [CrossRef]
- Lisonek, M.; Liu, S.; Dzakpasu, S.; Moore, A.M.; Joseph, K.S.; Canadian Perinatal Surveillance System (Public Health Agency of Canada). Changes in the incidence and surgical treatment of ankyloglossia in Canada. Paediatr. Child Health. 2017, 22, 382–386. [Google Scholar] [CrossRef]
- Jin, R.R.; Sutcliffe, A.; Vento, M.; Miles, C.; Travadi, J.; Kishore, K.; Suzuki, K.; Todd, D.; Wooderson, S.; Kamar, A.A.; et al. What does the world think of ankyloglossia? Acta Paediatr. 2018, 107, 1733–1738. [Google Scholar] [CrossRef]
- Ganesan, K.; Girgis, S.; Mitchell, S. Lingual frenotomy in neonates: Past, present, and future. Br. J. Oral Maxillofac. Surg. 2019, 57, 207–213. [Google Scholar] [CrossRef]
- Cetinkaya, M.; Oz, F.T.; Orhan, A.I.; Orhan, K.; Karabulut, B.; Can-Karabulut, D.C.; Ilk, O. Prevalence of oral abnormalities in a Turkish newborn population. Int. Dent. J. 2011, 61, 90–100. [Google Scholar] [CrossRef]
- Maya-Enero, S.; Pérez-Pérez, M.; Ruiz-Guzmán, L.; Duran-Jordà, X.; López-Vílchez, M.Á. Prevalence of neonatal ankyloglossia in a tertiary care hospital in Spain: A transversal cross-sectional study. Eur. J. Pediatr. 2021, 180, 751–757. [Google Scholar] [CrossRef]
- Haham, A.; Marom, R.; Mangel, L.; Botzer, E.; Dollberg, S. Prevalence of breastfeeding difficulties in newborns with a lingual frenulum: A prospective cohort series. Breastfeed Med. 2014, 9, 438–441. [Google Scholar] [CrossRef]
- Ngerncham, S.; Laohapensang, M.; Wongvisutdhi, T.; Ritjaroen, Y.; Painpichan, N.; Hakularb, P.; Gunnaleka, P.; Chaturapitphothong, P. Lingual frenulum and effect on breastfeeding in Thai newborn infants. Paediatr. Int. Child Health 2013, 33, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Daggumati, S.; Cohn, J.E.; Brennan, M.J.; Evarts, M.; McKinnon, B.J.; Terk, A.R. Caregiver perception of speech quality in patients with ankyloglossia: Comparison between surgery and non-treatment. Int. J. Pediatr. Otorhinolaryngol. 2019, 119, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Coryllos, E.; Genna, C.; Salloum, A.C. Congenital tongue-tie and its impact on breastfeeding. Breastfeed. Best Mother Baby Newsl. 2004, 1–6. [Google Scholar]
- Suter, V.G.; Bornstein, M.M. Ankyloglossia: Facts and Myths in Diagnosis and Treatment. J. Periodontol. 2009, 80, 1204–1219. [Google Scholar] [CrossRef] [PubMed]
- Segal, L.M.; Stephenson, R.; Dawes, M.; Feldman, P. Prevalence, diagnosis, and treatment of ankyloglossia: Methodologic review. Can. Fam. Physician 2007, 53, 1027–1033. [Google Scholar]
- Hill, R. Implications of Ankyloglossia on Breastfeeding. MCN Am. J. Matern. Child Nurs. 2019, 44, 73–79. [Google Scholar] [CrossRef]
- Genna, C.; Coryllos, E. Breastfeeding and Tongue-tie. J. Hum. Lact. 2009, 25, 108. [Google Scholar] [CrossRef] [PubMed]
- KotloW, L.A. Ankyloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence Int. 1999, 30, 259–262. [Google Scholar]
- Hazelbaker, A.K. Newborn tongue-tie and breast-feeding. J. Am. Board Fam. Pract. 2005, 18, 326–327. [Google Scholar] [CrossRef]
- Martinelli, R.L.; Marchesan, I.Q.; Berretin-Felix, G. Lingual frenulum protocol with scores for infants. Int. J. Orofac. Myol. 2012, 38, 104–112. [Google Scholar] [CrossRef]
- Martinelli, R.L.; Marchesan, I.Q.; Gusmão, R.J.; Honório, H.M.; Berretin-Felix, G. The effects of frenotomy on breastfeeding. J. Appl. Oral Sci. 2015, 23, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.; Al Khoury, A.; Puzhko, S.; Dobrich, C.; Stern, M.; Mitnick, H.; Goldfarb, L. Frenotomy in Infants with Tongue-Tie and Breastfeeding Problems. J. Hum. Lact. 2019, 35, 706–712. [Google Scholar] [CrossRef]
- Ghaheri, B.A.; Cole, M.; Mace, J.C. Revision Lingual Frenotomy Improves Patient-Reported Breastfeeding Outcomes: A Prospective Cohort Study. J. Hum. Lact. 2018, 34, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.; Griffiths, M.; Westcott, C. A double-blind, randomized, controlled trial of tongue-tie division and its immediate effect on breastfeeding. Breastfeed. Med. 2012, 7, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Emond, A.; Ingram, J.; Johnson, D.; Blair, P.; Whitelaw, A.; Copeland, M.; Sutcliffe, A. Randomised controlled trial of early frenotomy in breastfed infants with mild-moderate tongue-tie. Arch. Dis. Child Fetal Neonatal. Ed. 2014, 99, 189–195. [Google Scholar] [CrossRef]
- Khan, U.; MacPherson, J.; Bezuhly, M.; Hong, P. Comparison of Frenotomy Techniques for the Treatment of Ankyloglossia in Children: A Systematic Review. Otolaryngol. Head Neck Surg. 2020, 163, 428–443. [Google Scholar] [CrossRef]
- Sethi, N.; Smith, D.; Kortequee, S.; Ward, V.M.; Clarke, S. Benefits of frenulotomy in infants with ankyloglossia. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 762–765. [Google Scholar] [CrossRef]
- Auychai, P.; Neff, A.; Pitak-Arnnop, P. Tongue-Tie children with a severe Hazelbaker score or difficult breastfeeding greatly benefit from frenotomy or frenuloplasty with/without anaesthesia—First do or do no harm? J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e76–e81. [Google Scholar] [CrossRef]


{kind=link}
| Type 1: Insertion of the frenulum to the tip of the tongue |
| Type 2: Insertion of the frenulum slightly (2 to 4 mm) behind the tip of the tongue |
| Type 3: Thickened frenulum attached to the mid-tongue and the middle of the floor of the mouth, usually tighter and less elastic |
| Type 4: Thick, shiny, and very inelastic submucosal frenulum that restricts movement at the base of the tongue |
| Frenotomy | Total | p | ||
|---|---|---|---|---|
| Done | Not Done | |||
| Coryllos type 1 | 14 (6.1%) | 0 | 14 (6.1%) | <0.001 |
| Coryllos type 2 | 32 (13.7%) | 12 (5.1%) | 44 (18.8%) | |
| Coryllos type 3 | 15 (6.4%) | 150 (64.1%) | 165 (70.5%) | |
| Coryllos type 4 | 6 (2.5%) | 5 (2.1%) | 11 (4.6%) | |
| Total | 67 (28.7%) | 167 (71.3%) | 234 (100%) | |
| Chi Square | ||||
| Type 1 | Type 2 | Type 3 | Type 4 | Total | ||
|---|---|---|---|---|---|---|
| Frenotomy Procedure | Day 1 | 12 | 8 | 3 | 0 | 23 |
| Day 7 | 2 | 24 | 12 | 4 | 42 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Unable to Breastfeed | Day 1 | 12 | 8 | 3 | 0 | 23 |
| Day 7 | 0 | 0 | 0 | 0 | 0 | |
| Day 28 | 0 | 0 | 0 | 0 | 0 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Weak Grasp | Day 1 | 12 | 8 | 3 | 0 | 23 |
| Day 7 | 0 | 0 | 0 | 0 | 0 | |
| Day 28 | 0 | 0 | 0 | 0 | 0 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Poor Latch | Day 1 | 14 | 32 | 15 | 6 | 67 |
| Day 7 | 2 | 24 | 12 | 6 | 34 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Nipple Slipping Out of the Mouth | Day 1 | 14 | 32 | 15 | 6 | 67 |
| Day 7 | 2 | 24 | 12 | 6 | 34 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Nipple Biting | Day 1 | 14 | 32 | 15 | 6 | 67 |
| Day 7 | 2 | 24 | 12 | 6 | 34 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Weak Suction | Day 1 | 14 | 32 | 15 | 6 | 67 |
| Day 7 | 2 | 24 | 12 | 6 | 34 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Weight Loss | Day 1 | 0 | 0 | 0 | 0 | 0 |
| Day 7 | 0 | 0 | 0 | 0 | 0 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 | |
| Frequent-Short Feeding Durations | Day 1 | 14 | 32 | 15 | 6 | 67 |
| Day 7 | 2 | 24 | 12 | 6 | 34 | |
| Day 28 | 0 | 0 | 0 | 2 | 2 | |
| Day 60 | 0 | 0 | 0 | 0 | 0 | |
| Day 90 | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narsat, M.A.; Beygirci, A.; Özdönmez, G.T.; Yıldız, E. Grouping of Ankyloglossia According to Coryllos Anatomical Classification and Follow-Up Results for Breastfeeding: Single-Center, Cross-Sectional Study. Children 2022, 9, 1860. https://doi.org/10.3390/children9121860
Narsat MA, Beygirci A, Özdönmez GT, Yıldız E. Grouping of Ankyloglossia According to Coryllos Anatomical Classification and Follow-Up Results for Breastfeeding: Single-Center, Cross-Sectional Study. Children. 2022; 9(12):1860. https://doi.org/10.3390/children9121860
Chicago/Turabian StyleNarsat, Mehmet Ali, Abdulvehhap Beygirci, Gökçen Tuğçe Özdönmez, and Eren Yıldız. 2022. "Grouping of Ankyloglossia According to Coryllos Anatomical Classification and Follow-Up Results for Breastfeeding: Single-Center, Cross-Sectional Study" Children 9, no. 12: 1860. https://doi.org/10.3390/children9121860
APA StyleNarsat, M. A., Beygirci, A., Özdönmez, G. T., & Yıldız, E. (2022). Grouping of Ankyloglossia According to Coryllos Anatomical Classification and Follow-Up Results for Breastfeeding: Single-Center, Cross-Sectional Study. Children, 9(12), 1860. https://doi.org/10.3390/children9121860