
Role of Volume Replacement during Neonatal Resuscitation in the Delivery Room

 ,
,
Abstract
1. Introduction
2. Discussion
2.1. Current American Recommendations on Volume Replacement in the Delivery Room
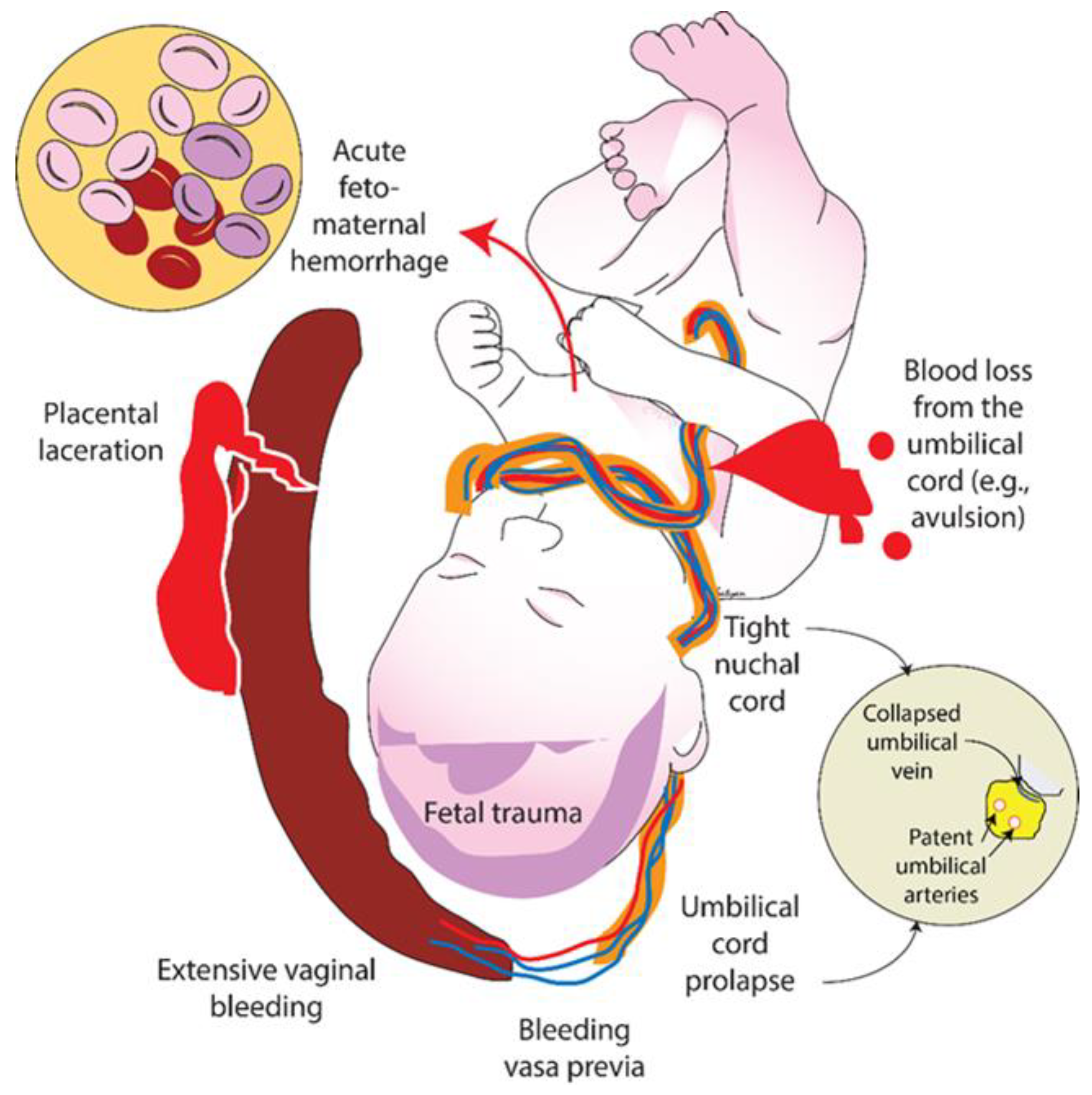
2.2. Clinical Suspicion of Hypovolemia due to Blood Loss
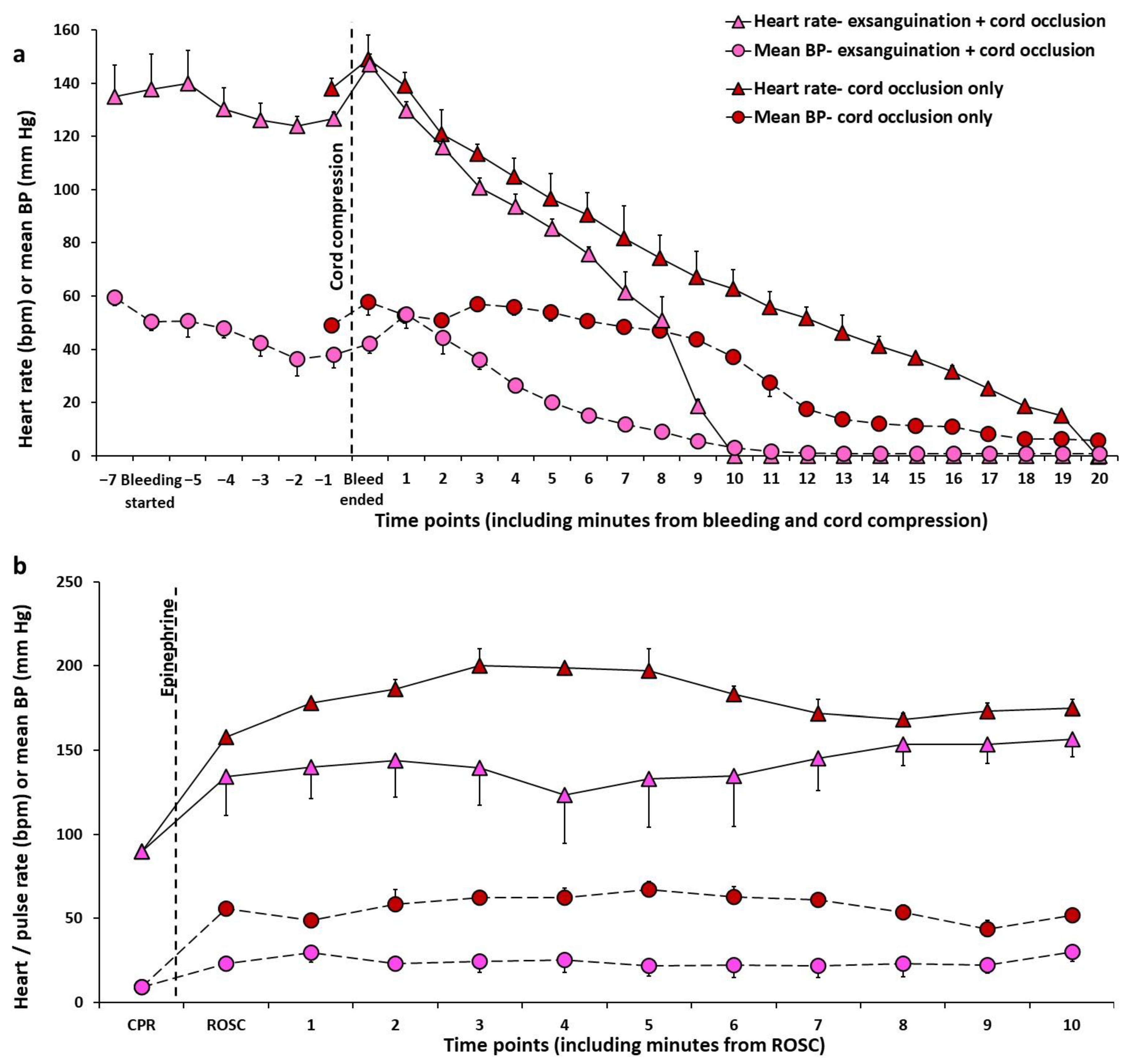
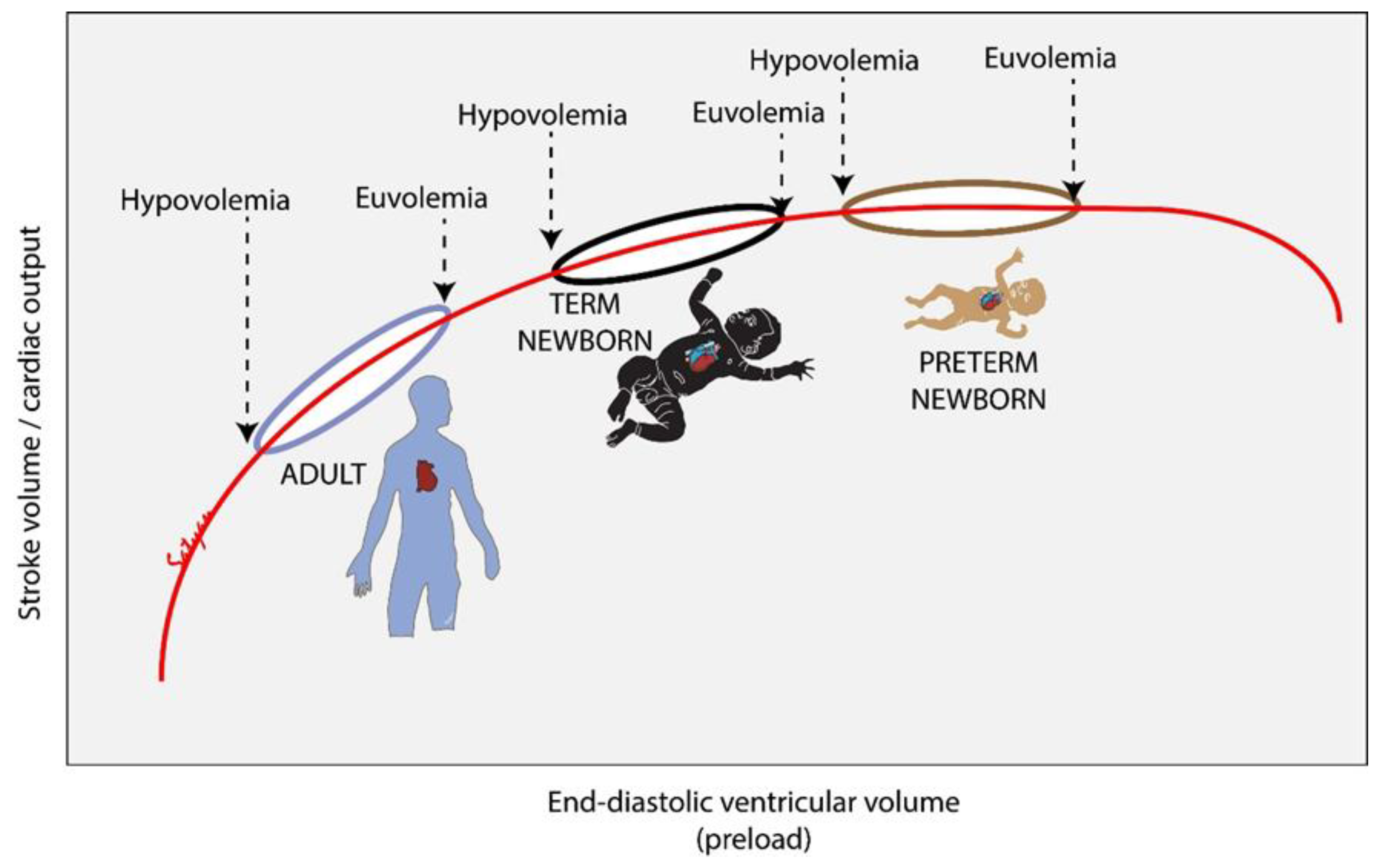
2.3. How Does the Fetus Respond to Hypovolemia?
2.4. Evidence on Volume Replacement in Asphyxiated Neonates from Animal Studies
2.5. Evidence on Volume Replacement from Clinical Studies
2.6. Potential Harm from Volume Replacement in the Delivery Room
2.7. What Is the Optimal Fluid for Volume Replacement-Crystalloid (Normal Saline-NS vs. Lactated Ringer’s—LR) or Colloid (5% Albumin)?
2.8. Role of Deferred Cord Clamping in Hypovolemic Neonates
2.9. Umbilical Cord Milking in Non-Vigorous Neonates as a Source of Blood Volume
2.10. What Happens to Fetal Blood Volume in the Case of Tight Nuchal Cord?
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weiner, G.M.; Zaichkin, J. Textbook of Neonatal Resuscitation, 8th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2021. [Google Scholar]
- Lawn, J.E.; Blencowe, H.; Oza, S.; You, D.; Lee, A.C.; Waiswa, P.; Lalli, M.; Bhutta, Z.; Barros, A.J.; Christian, P.; et al. Every Newborn: Progress, priorities, and potential beyond survival. Lancet 2014, 384, 189–205. [Google Scholar] [CrossRef]
- Foglia, E.E.; Weiner, G.; de Almeida, M.F.B.; Wyllie, J.; Wyckoff, M.H.; Rabi, Y.; Guinsburg, R. Duration of Resuscitation at Birth, Mortality, and Neurodevelopment: A Systematic Review. Pediatrics 2020, 146, e20201449. [Google Scholar] [CrossRef] [PubMed]
- Rainaldi, A.M.; Perlman, J.M. Pathophysiology of birth asphyxia. Clin. Perinatol. 2016, 43, 409–422. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; de Almeida, M.F.; Fabres, J.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2020, 142, S185–S221. [Google Scholar] [CrossRef] [PubMed]
- Finn, D.; Roehr, C.C.; Ryan, C.A.; Dempsey, E.M. Optimising Intravenous Volume Resuscitation of the Newborn in the Delivery Room: Practical Considerations and Gaps in Knowledge. Neonatology 2017, 112, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Perlman, J.M.; Laptook, A.R. Use of volume expansion during delivery room resuscitation in near-term and term infants. Pediatrics 2005, 115, 950–955. [Google Scholar] [CrossRef]
- Aziz, K.; Lee, H.C.; Escobedo, M.B.; Hoover, A.V.; Kamath-Rayne, B.D.; Kapadia, V.S.; Magid, D.J.; Niermeyer, S.; Schmolzer, G.M.; Szyld, E.; et al. Part 5: Neonatal Resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S524–S550. [Google Scholar] [CrossRef] [PubMed]
- Polglase, G.R.; Ong, T.; Hillman, N.H. Cardiovascular Alterations and Multiorgan Dysfunction After Birth Asphyxia. Clin. Perinatol. 2016, 43, 469–483. [Google Scholar] [CrossRef]
- O’Donnell, C.P.; Kamlin, C.O.; Davis, P.G.; Carlin, J.B.; Morley, C.J. Clinical assessment of infant colour at delivery. Arch. Dis. Child. Fetal Neonatal. Ed. 2007, 92, F465–F467. [Google Scholar] [CrossRef]
- Yao, A.C.; Moinian, M.; Lind, J. Distribution of blood between infant and placenta after birth. Lancet 1969, 2, 871–873. [Google Scholar] [CrossRef]
- Robillard, J.E.; Weitzman, R.E.; Fisher, D.A.; Smith, F.G. The dynamics of vasopressin release and blood volume regulation during fetal hemorrhage in the lamb fetus. Pediatr. Res. 1979, 13, 606–610. [Google Scholar] [CrossRef][Green Version]
- Zanjani, E.D.; Peterson, E.N.; Gordon, A.S.; Washerman, L.R. Erythropoietin production in the fetus: Role of the kidney and maternal anemia. J. Lab. Clin. Med. 1974, 83, 281–287. [Google Scholar]
- Baylen, B.G.; Ogata, H.; Ikegami, M.; Jacobs, H.; Jobe, A.; Emmanouilides, G.C. Left ventricular performance and contractility before and after volume infusion: A comparative study of preterm and full-term newborn lambs. Circulation 1986, 73, 1042–1049. [Google Scholar] [CrossRef]
- Wyckoff, M.; Garcia, D.; Margraf, L.; Perlman, J.; Laptook, A. Randomized Trial of Volume Infusion During Resuscitation of Asphyxiated Neonatal Piglets. Pediatr. Res. 2007, 61, 415–420. [Google Scholar] [CrossRef]
- Mendler, M.R.; Schwarz, S.; Hechenrieder, L.; Kurth, S.; Weber, B.; Höfler, S.; Kalbitz, M.; Mayer, B.; Hummler, H.D. Successful Resuscitation in a Model of Asphyxia and Hemorrhage to Test Different Volume Resuscitation Strategies. A Study in Newborn Piglets After Transition. Front. Pediatr. 2018, 6, 192. [Google Scholar] [CrossRef]
- Sankaran, D.; Chandrasekharan, P.K.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nair, J.; Mathew, B.; Rawat, M.; Vali, P.; Nielsen, L.; et al. Randomised trial of epinephrine dose and flush volume in term newborn lambs. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 578–583. [Google Scholar] [CrossRef]
- Sankaran, D.; Vali, P.; Chandrasekharan, P.; Chen, P.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nair, J.; Mathew, B.; Rawat, M.; et al. Effect of a Larger Flush Volume on Bioavailability and Efficacy of Umbilical Venous Epinephrine during Neonatal Resuscitation in Ovine Asphyxial Arrest. Children 2021, 8, 464. [Google Scholar] [CrossRef]
- Osborn, A.D.; Evans, N.J. Early volume expansion for prevention of morbidity and mortality in very preterm infants. Cochrane Database Syst. Rev. 2004, 2004, CD002055. [Google Scholar] [CrossRef]
- Keir, A.; Froessler, B.; Stanworth, S. QUESTION 2: Are intravenous fluid boluses beneficial in late preterm or term infants with suspected haemodynamic compromise? Arch. Dis. Child. 2016, 101, 201–202. [Google Scholar] [CrossRef]
- Keir, A.K.; Karam, O.; Hodyl, N.; Stark, M.J.; Liley, H.G.; Shah, P.S.; Stanworth, S.J.; NeoBolus Study Group. International, multicentre, observational study of fluid bolus therapy in neonates. J. Paediatr. Child. Health 2019, 55, 632–639. [Google Scholar] [CrossRef]
- Shalish, W.; Olivier, F.; Aly, H.; Sant’Anna, G. Uses and Misuses of Albumin during Resuscitation and in the Neonatal Intensive Care Unit. In Seminars in Fetal and Neonatal Medicine; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Piquereau, J.; Ventura-Clapier, R. Maturation of Cardiac Energy Metabolism During Perinatal Development. Front. Physiol. 2018, 9, 959. [Google Scholar] [CrossRef]
- Rios, D.R.; Lapointe, A.; Schmolzer, G.M.; Mohammad, K.; VanMeurs, K.P.; Keller, R.L.; Sehgal, A.; Lakshminrusimha, S.; Giesinger, R.E. Hemodynamic optimization for neonates with neonatal encephalopathy caused by a hypoxic ischemic event: Physiological and therapeutic considerations. Semin. Fetal Neonatal Med. 2021, 26, 101277. [Google Scholar] [CrossRef]
- Nestaas, E.; Støylen, A.; Brunvand, L.; Fugelseth, D. Longitudinal strain and strain rate by tissue Doppler are more sensitive indices than fractional shortening for assessing the reduced myocardial function in asphyxiated neonates. Cardiol. Young 2011, 21, 1–7. [Google Scholar] [CrossRef]
- Vrancken, S.L.; van Heijst, A.F.; de Boode, W.P. Neonatal Hemodynamics: From Developmental Physiology to Comprehensive Monitoring. Front. Pediatr. 2018, 6, 87. [Google Scholar] [CrossRef]
- Massaro, A.N.; Govindan, R.B.; Vezina, G.; Chang, T.; Andescavage, N.N.; Wang, Y.; Al-Shargabi, T.; Metzler, M.; Harris, K.; Plessis, A.J.D. Impaired cerebral autoregulation and brain injury in newborns with hypoxic-ischemic encephalopathy treated with hypothermia. J. Neurophysiol. 2015, 114, 818–824. [Google Scholar] [CrossRef]
- Oca, M.J.; Nelson, M.; Donn, S.M. Randomized trial of normal saline versus 5% albumin for the treatment of neonatal hypotension. J. Perinatol. 2003, 23, 473–476. [Google Scholar] [CrossRef]
- Lynch, S.; Mullett, M.; Graeber, J.; Polak, M. A comparison of albumin-bolus therapy versus normal saline-bolus therapy for hypotension in neonates. J. Perinatol. 2008, 28, 29–33. [Google Scholar] [CrossRef]
- Todd, S.R.; Malinoski, D.; Muller, P.J.; Schreiber, M.A. Lactated Ringer’s is Superior to Normal Saline in the Resuscitation of Uncontrolled Hemorrhagic Shock. J. Trauma Acute Care Surg. 2007, 62, 636–639. [Google Scholar] [CrossRef]
- Healey, M.A.; Davis, R.E.; Liu, F.C.; Loomis, W.H.; Hoyt, D.B. Lactated Ringer’s is superior to normal saline in a model of massive hemorrhage and resuscitation. J. Trauma Acute Care Surg. 1998, 45, 894–899. [Google Scholar] [CrossRef]
- Eisenhut, M. Adverse effects of rapid isotonic saline infusion. Arch. Dis. Child. 2006, 91, 797. [Google Scholar] [CrossRef]
- Bullivant, E.; Wilcox, C.; Welch, W. Intrarenal vasoconstriction during hyperchloremia: Role of thromboxane. Am. J. Physiol.-Ren. Physiol. 1989, 256, F152–F157. [Google Scholar] [CrossRef]
- Brill, S.A.; Stewart, T.R.; Brundage, S.I.; Schreiber, M.A. Base deficit does not predict mortality when secondary to hyperchloremic acidosis. Shock 2002, 17, 459–462. [Google Scholar] [CrossRef]
- Linderkamp, O.; Versmold, H.T.; Messow-Zahn, K.; Müller-Holve, W.; Riegel, K.P.; Betke, K. The effect of intra-partum and intra-uterine asphyxia on placental transfusion in premature and full-term infants. Eur. J. Pediatr. 1978, 127, 91–99. [Google Scholar] [CrossRef]
- Oh, W.; Omori, K.; Emmanouilides, G.C.; Phelps, D.L. Placenta to lamb fetus transfusion in utero during acute hypoxia. Am. J. Obs. Gynecol. 1975, 122, 316–322. [Google Scholar] [CrossRef]
- Yao, A.C.; Lind, J. Blood volume in the asphyxiated term neonate. Biol Neonate 1972, 21, 199–209. [Google Scholar] [CrossRef]
- Koo, J.; Katheria, A.C.; Polglase, G. A Newborn’s “Life Line”—A Review of Umbilical Cord Management Strategies. In Seminars in Perinatology; WB Saunders: Philadelphia, PA, USA, 2022; p. 151621. [Google Scholar]
- Katheria, A.C.; Clark, E.; Yoder, B.; Schmölzer, G.M.; Law, B.H.Y.; El-Naggar, W.; Rittenberg, D.; Sheth, S.; Mohamed, M.A.; Martin, C.; et al. Umbilical cord milking in non-vigorous infants: A cluster-randomized crossover trial. Am. J. Obs. Gynecol 2022. [Google Scholar] [CrossRef]
- Katheria, A.; Reister, F.; Essers, J.; Mendler, M.; Hummler, H.; Subramaniam, A.; Carlo, W.; Tita, A.; Truong, G.; Davis-Nelson, S.; et al. Association of Umbilical Cord Milking vs. Delayed Umbilical Cord Clamping with Death or Severe Intraventricular Hemorrhage Among Preterm Infants. JAMA 2019, 322, 1877–1886. [Google Scholar] [CrossRef]
- Peesay, M. Nuchal cord and its implications. Matern Health Neonatol. Perinatol. 2017, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Henry, E.; Andres, R.L.; Christensen, R.D. Neonatal outcomes following a tight nuchal cord. J. Perinatol. 2013, 33, 231–234. [Google Scholar] [CrossRef][Green Version]
- Larson, J.D.; Rayburn, W.F.; Crosby, S.; Thurnau, G.R. Multiple nuchal cord entanglements and intrapartum complications. Am. J. Obstet. Gynecol. 1995, 173, 1228–1231. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Asphyxiation Method | Comparison Groups | Results and Comments |
|---|---|---|---|
| Wyckoff et al. [15] 2007— Newborn piglets age 8 ± 4 days | Ventilatory gases changed to 7.5% CO2 and 5.3% O2, ventilatory rate reduced by 10/min every 15 min until pH < 7.0, PaCO2 > 100 mm Hg, MAP < 20 mm Hg, HR < 100 bpm. | 10 mL/kg IV over 5 min of either 5% albumin, normal saline and no bolus (Sham). After a 2 min pause, a second bolus of 10 mL/kg administered over 5 min. | MAP was similar during resuscitation in 5% albumin and normal saline groups and was lower with normal saline (29 ± 10 mm Hg) at 2 h post-resuscitation compared to 5% albumin (43 ± 19 mm Hg) and sham (48 ± 13 mm Hg). Volume expansion was associated with increased pulmonary edema. In absence of hypovolemia, volume expansion is not beneficial. |
| Mendler et al. [16] 2018— Newborn piglets age 32 h (12–44 h) | Progressive hypoxia by reducing FiO2 to 0.08, adding CO2 (FiCO2 0.07), reducing ventilatory rate by 10/min every 10 min. At 12 min or when pH < 7.0, hypovolemic was induced by removal of blood 2 mL/kg/min from arterial line, until cardiac arrest/asystole. | Crystalloid group vs. early transfusion group: normal saline or animal’s own anticoagulated blood administered at 10 mL/kg over 2 min, maximum 3 boluses immediately after each other. | ROSC occurred before volume infusion in 25% of the subjects. Among the piglets that received volume expansion, there was no difference in time to ROSC between crystalloid vs. early transfusion groups. No difference in epinephrine use. |
| Study | Topic | Number of Articles Included | Findings and Recommendations |
|---|---|---|---|
| Finn et al., 2017 [6], narrative review | Volume resuscitation in the delivery room | none | No current clinical tools allow differentiation of an asphyxiated infant who will benefit from volume replacement from a normovolemic asphyxiated infant who may deteriorate with volume replacement. Consider volume expansion in the setting of presumed blood loss, with fresh blood if available, or with crystalloid. |
| Keir et al., 2016 [20], systematic review | Late preterm and term neonates with hemodynamic compromise, excluding acute hemorrhage | Two studies | No robust evidence to support fluid bolus for infants with hemodynamic compromise without acute blood loss. Complications of fluid boluses include volume overload (affecting end-organ function), dilutional coagulopathy, electrolyte imbalance with hyperchloremic metabolic acidosis after normal saline and adverse effects from blood transfusions. Routine use of fluid boluses is to be avoided in absence of acute hemorrhage. |
| Shalish et al., 2017 [22], systematic review | Albumin use as volume expander in various settings including the delivery room. | none | Albumin appears to be equally effective as crystalloids in improving hemodynamics such as blood pressure but is associated with higher mortality. In asphyxiated infants, albumin may increase oncotic pressure and cause transudation of fluid in interstitial space. Crystalloids (normal saline) are preferred for fluid resuscitation over albumin. |
| Keir et al., 2019 [21], cross-sectional survey | International multicenter observational study in 41 neonatal units—fluid bolus for suspected hemodynamic compromise | 5/163 infants received a fluid bolus for neonatal resuscitation. No further details provided. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sankaran, D.; Lane, E.C.A.; Valdez, R.; Lesneski, A.L.; Lakshminrusimha, S. Role of Volume Replacement during Neonatal Resuscitation in the Delivery Room. Children 2022, 9, 1484. https://doi.org/10.3390/children9101484
Sankaran D, Lane ECA, Valdez R, Lesneski AL, Lakshminrusimha S. Role of Volume Replacement during Neonatal Resuscitation in the Delivery Room. Children. 2022; 9(10):1484. https://doi.org/10.3390/children9101484
Chicago/Turabian StyleSankaran, Deepika, Emily C. A. Lane, Rebecca Valdez, Amy L. Lesneski, and Satyan Lakshminrusimha. 2022. "Role of Volume Replacement during Neonatal Resuscitation in the Delivery Room" Children 9, no. 10: 1484. https://doi.org/10.3390/children9101484
APA StyleSankaran, D., Lane, E. C. A., Valdez, R., Lesneski, A. L., & Lakshminrusimha, S. (2022). Role of Volume Replacement during Neonatal Resuscitation in the Delivery Room. Children, 9(10), 1484. https://doi.org/10.3390/children9101484