
Chronic Nocturnal Abdominal Pain as the Presentation of Inverted Meckel Diverticulum: A Case Report

Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hansen, C.C.; Søreide, K. Systematic review of epidemiology, presentation, and management of Meckel’s diverticulum in the 21st century. Medicine 2018, 97, e12154. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.; Xu, X.; Geng, L.; Huang, Y.; Ding, G.; Ji, H. The Clinical Manifestation Variety and Management Choice of Meckel’s Diverticulum with Complication: A Single Center Experience. Gastroenterol. Res. Pract. 2021, 2021, 6640660. [Google Scholar] [CrossRef] [PubMed]
- Loukas, M.; Pellerin, M.; Kimball, Z.; de la Garza-Jordan, J.; Tubbs, R.S.; Jordan, R. Intussusception: An anatomical perspective with review of the literature. Clin. Anat. 2011, 24, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Fiegel, H.; Gfroerer, S.; Rolle, U. Systematic review shows that pathological lead points are important and frequent in intussusception and are not limited to infants. Acta Paediatr. 2016, 105, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Park, S.H.; Ha, H.K. Case 156: Inverted Meckel diverticulum. Radiology 2010, 255, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Bains, L.; Bhatia, R.; Kaushik, R.; Lal, P.; Rajpaul, G. Inverted Meckel’s diverticulum: A case report. J. Med. Case Rep. 2021, 15, 264. [Google Scholar] [CrossRef] [PubMed]
- Spangler, H.; Fisher, J. The rule of two’s didn’t work: Meckel’s diverticulum with hemorrhagic shock in an adolescent. Am. J. Emerg. Med. 2020, 38, 1541.e1–1541.e2. [Google Scholar] [CrossRef] [PubMed]
- Giroux, P.; Collier, A.; Nowicki, M. Recurrent lymphoma presenting as painless, chronic intussusception: A case report. World J. Clin. Cases 2020, 8, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Han, S.A.; Won, K.Y. Chronic Intussusception Caused by Diffuse Large B-Cell Lymphoma in a 6-Year-Old Girl Presenting with Abdominal Pain and Constipation for 2 Months. J. Korean Med. Sci. 2016, 31, 321–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.Y.; Ho, K.Y.; Yeoh, K.G.; Guan, R. Chronic upper abdominal pain due to duodenal ulcer and other structural and functional causes: Its localization and nocturnal occurrence. J. Gastroenterol. Hepatol. 1996, 11, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Orfei, M.; Gasparetto, M.; Hensel, K.O.; Zellweger, F.; Heuschkel, R.B.; Zilbauer, M. Guidance on the interpretation of faecal calprotectin levels in children. PLoS ONE 2021, 16, e0246091. [Google Scholar] [CrossRef] [PubMed]
- Brandler, J.; Chey, W.D. Fishing for Irritable Bowel Syndrome: Which Alarm Features Weave the Best Net? Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hunt, R.; Armstrong, D.; Katelaris, P.; Afihene, M.; Bane, A.; Bhatia, S.; Chen, M.H.; Choi, M.G.; Melo, A.C.; Fock, K.M.; et al. World Gastroenterology Organisation Global Guidelines: GERD Global Perspective on Gastroesophageal Reflux Disease. J. Clin. Gastroenterol. 2017, 51, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Sheth, R.A.; Gervais, D.A.; Gee, M.A. Imaging of Pediatric Gastrointestinal Disease. In Walker’s Pediatric Gastrointestinal Disease: Pathology, Diagnosis, Management, 6th ed.; Kleinman, R.E., Goulet, O.J., Mieli-Vergani, G., Sanderson, I.R., Sherman, P.M., Shneider, B.L., Eds.; PMPH USA, Ltd.: Raleigh, NC, USA, 2018; p. 5443. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Date | Hospital | Event |
|---|---|---|
| Seven months prior to this admission | A regional hospital | Intussusception was suspected on abdominal sonography, and it was resolved by lower gastrointestinal (LGI) series reduction |
| Three months prior to this admission | The same regional hospital as the 1st episode | Sonography suspected intussusception but LGI series revealed no evidence of intussusception. Incompletely obstructing intussusception was suspected. |
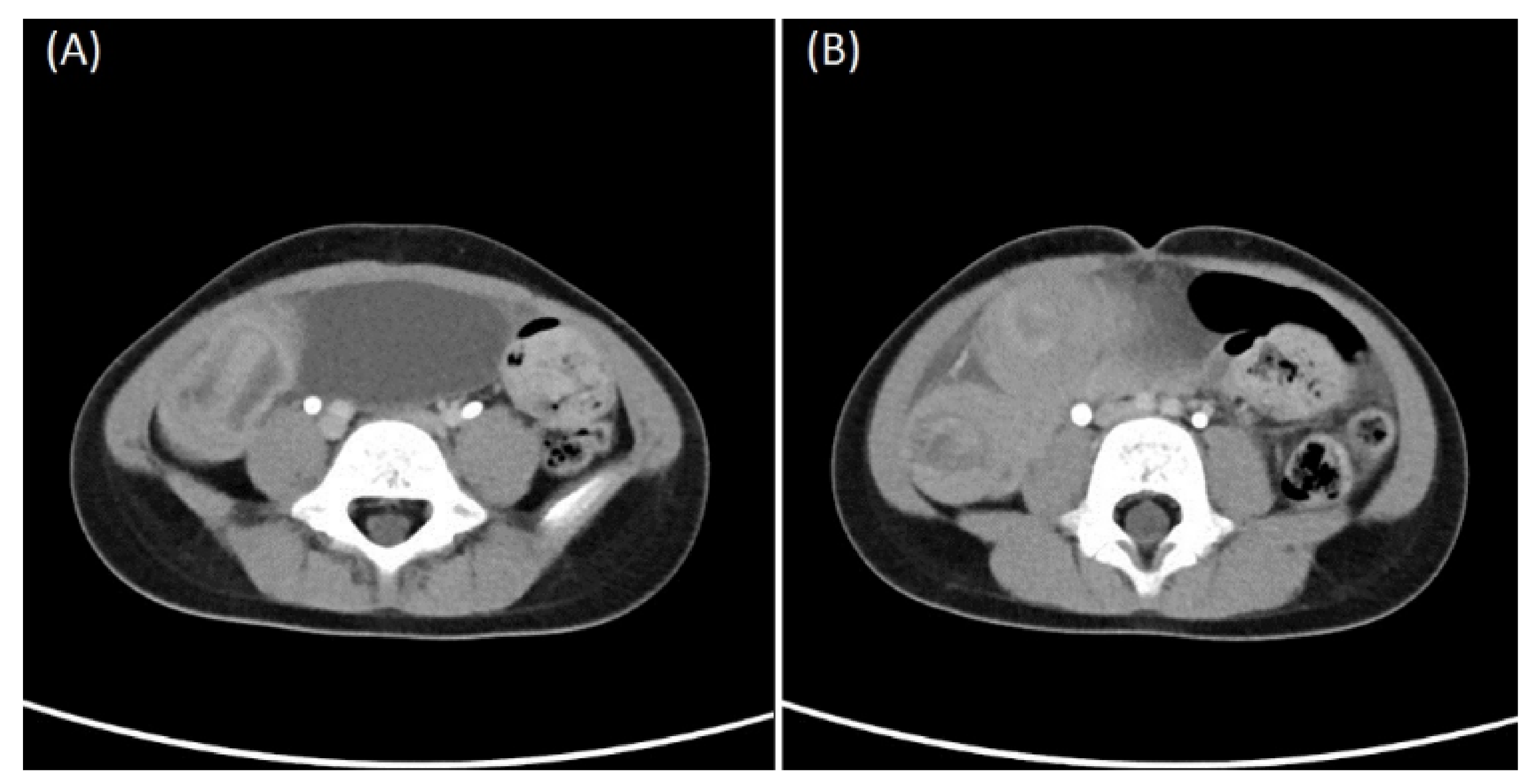
| One month prior to this admission | A medical center | Computed tomography (CT) suspected intussusception but upper gastrointestinal series showed negative finding. Incompletely obstructing intussusception was suspected again. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-Y.; Su, Y.-T.; Ko, P.-J.; Chen, Y.-L.; Shih, H.-H.; Tsai, C.-C. Chronic Nocturnal Abdominal Pain as the Presentation of Inverted Meckel Diverticulum: A Case Report. Children 2022, 9, 69. https://doi.org/10.3390/children9010069
Wang T-Y, Su Y-T, Ko P-J, Chen Y-L, Shih H-H, Tsai C-C. Chronic Nocturnal Abdominal Pain as the Presentation of Inverted Meckel Diverticulum: A Case Report. Children. 2022; 9(1):69. https://doi.org/10.3390/children9010069
Chicago/Turabian StyleWang, Ting-Yu, Yu-Tsun Su, Po-Jui Ko, Yea-Ling Chen, Hsiang-Hung Shih, and Ching-Chung Tsai. 2022. "Chronic Nocturnal Abdominal Pain as the Presentation of Inverted Meckel Diverticulum: A Case Report" Children 9, no. 1: 69. https://doi.org/10.3390/children9010069
APA StyleWang, T.-Y., Su, Y.-T., Ko, P.-J., Chen, Y.-L., Shih, H.-H., & Tsai, C.-C. (2022). Chronic Nocturnal Abdominal Pain as the Presentation of Inverted Meckel Diverticulum: A Case Report. Children, 9(1), 69. https://doi.org/10.3390/children9010069