
Fundamental Movement Skills and Physical Activity of 3–4-Year-Old Children within Early Childhood Centers in New Zealand

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.2.1. Fundamental Movement Skill Assessment
2.2.2. Physical Activity (Accelerometry)
2.2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gubbels, J.S.; Van Kann, D.H.; Jansen, M.W. Play equipment, physical activity opportunities, and children’s activity levels at childcare. J. Environ. Public Health 2012, 2012, 326520. [Google Scholar] [CrossRef]
- Hnatiuk, J.; Ridgers, N.D.; Salmon, J.; Campbell, K.; McCallum, Z.; Hesketh, K. Physical activity levels and patterns of 19-month-old children. Med. Sci. Sports Exerc. 2012, 44, 1715–1720. [Google Scholar] [CrossRef]
- Cliff, D.P.; McNeill, J.; Vella, S.A.; Howard, S.J.; Santos, R.; Batterham, M.; Melhuish, E.; Okely, A.D.; de Rosnay, M. Adherence to 24-h movement guidelines for the early years and associations with social-cognitive development among Australian preschool children. BMC Public Health 2017, 17 (Suppl. 5), 857. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.M.B.; Atatoa Carr, P.E.; Grant, C.C.; Berry, S.D.; Bandara, D.K.; Mohal, J.; Tricker, P.J.; Ivory, V.C.; Kingi, T.R.; Liang, R.; et al. Growing Up in New Zealand: A Longitudinal Study of New Zealand Children and Their Families. Now We Are Two: Describing our First 1000 Days. 2014. Available online: https://www.growingup.co.nz/sites/growingup.co.nz/files/2019-10/report03.pdf (accessed on 7 June 2021).
- Ministry of Health. Sit Less, Move More, Sleep Well: Active Play Guidelines for Under-Fives; Ministry of Health: Wellington, New Zealand, 2017.
- Andersen, E.; Ovreas, S.; Jorgensen, K.A.; Borch-Jenssen, J.; Moser, T. Children’s physical activity level and sedentary behaviour in Norwegian early childhood education and care: Effects of a staff-led cluster-randomised controlled trial. BMC Public Health 2020, 20, 1651. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P. The physical activity levels of preschool-aged children: A systematic review. Early Child. Res. Q. 2008, 23, 547–558. [Google Scholar] [CrossRef]
- Brown, W.H.; Pfeiffer, K.A.; McIver, K.L.; Dowda, M.; Addy, C.L.; Pate, R.R. Social and environmental factors associated with preschoolers’ nonsedentary physical activity. Child. Dev. 2009, 80, 45–58. [Google Scholar] [CrossRef]
- Hannon, J.C.; Brown, B.B. Increasing preschoolers’ physical activity intensities: An activity-friendly preschool playground intervention. Prev. Med. 2008, 46, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Pigou, D.; Clarke, L.; McLachlan, C. Literature review on motor skill and physical activity in preschool children in New Zealand. Adv. Phys. Educ. 2017, 07, 10–26. [Google Scholar] [CrossRef]
- Campbell, K.J.; Hesketh, K.D. Strategies which aim to positively impact on weight, physical activity, diet and sedentary behaviours in children from zero to five years. A systematic review of the literature. Obes. Rev. 2007, 8, 327–338. [Google Scholar] [CrossRef]
- Oliver, M.; Duncan, S.; Kuch, C.; McPhee, J.; Schofield, G. Prevalence of New Zealand children and adolescents achieving current physical activity and television watching recommendations. J. Phys. Act. Health 2012, 9, 173–187. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Jones, R.A.; Hinkley, T.; Crawford, D.; Okely, A.D. Patterns of physical activity and sedentary behaviour in preschool children. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 138. [Google Scholar] [CrossRef]
- Ministry of Education. Participation in Early Learning: 2020 ECE Census Results; Education Counts: Wellington, New Zealand, 2021. Available online: https://www.educationcounts.govt.nz/__data/assets/pdf_file/0008/205847/Participation-in-Early-Learning.pdf (accessed on 1 April 2021).
- McLachlan, C.; Smith, J.; McLaughlin, T.; Ali, A.; Conlon, C.; Mugridge, O.; Foster, S. Development of teachers’ knowledge and skills in implementing a physical education curriculum: A New Zealand early childhood intervention study. Int. J. Early Child. 2017, 49, 211–228. [Google Scholar] [CrossRef]
- UNICEF Innocenti. Worlds of Influence: Understanding What Shapes Child Well-Being in Rich Countries; UNICEF Office of Research–Innocenti: Florence, Italy, 2020. [Google Scholar]
- Ministry of Health. Understanding Excess Body Weight: New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2015.
- Wrotniak, B.H.; Epstein, L.H.; Dorn, J.M.; Jones, K.E.; Kondilis, V.A. The relationship between motor proficiency and physical activity in children. Pediatrics 2006, 118, e1758–e1765. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A. Obesity prevention: The role of policies, laws and regulations. Aust. N. Z. Health Policy 2008, 5, 12. [Google Scholar] [CrossRef]
- Wolfenden, L.; Jones, J.; Williams, C.M.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Wiggers, J.; Williams, A.J.; Seward, K.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2016, 10, CD011779. [Google Scholar] [CrossRef] [PubMed]
- Gunner, K.B.; Atkinson, P.M.; Nichols, J.; Eissa, M.A. Health promotion strategies to encourage physical activity in infants, toddlers, and preschoolers. J. Pediatr. Health Care 2005, 19, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Annual Data Explorer 2019/2020; Ministry of Health: Wellington, New Zealand, 2020. Available online: Minhealthnz.shinyapps.io/nz-health-survey-2019-20-annual-data-explorer/_w_9efb10e8/#!/key-indicators (accessed on 1 April 2021).
- Coleman, B.; Dyment, J.E. Factors that limit and enable preschool-aged children’s physical activity on child care centre playgrounds. J. Early Child. Res. 2013, 11, 203–221. [Google Scholar] [CrossRef]
- Dyment, J.E.; Coleman, B. The intersection of physical activity opportunities and the role of early childhood educators during outdoor play: Perceptions and reality. Aust. J. Early Child. 2012, 37, 90–98. [Google Scholar] [CrossRef]
- Tandon, P.; Hassairi, N.; Soderberg, J.; Joseph, G. The relationship of gross motor and physical activity environments in child care settings with early learning outcomes. Early Child. Dev. Care 2020, 190, 570–579. [Google Scholar] [CrossRef]
- Little, H.; Wyver, S.; Gibson, F. The influence of play context and adult attitudes on young children’s physical risk-taking during outdoor play. Eur. Early Child. Educ. Res. J. 2011, 19, 113–131. [Google Scholar] [CrossRef]
- Kolt, G.S.; Schofield, G.M.; McLachlan, C.J.; Oliver, M.; Lucas, P.; Maddison, R.; Walters, S. Active Movement: Scoping Exercise and Programme Evaluation; Centre for Physical Activity and Nutrition Research, Auckland University of Technology: Auckland, New Zealand, 2005. [Google Scholar]
- Oliver, M.; Schofield, G.M.; Kolt, G.S. Physical activity in preschoolers: Understanding prevalence and measurement issues. Sports Med. 2007, 37, 1045–1070. [Google Scholar] [CrossRef]
- Oliver, M.; McLachlan, C. Physical activity: An overview of policy and practice in early childhood education and care. Early Edu. 2006, 40, 15–19. [Google Scholar]
- Kane, R. Initial Teacher Education: Policy and Practice. Final Report; Ministry of Education: Wellington, New Zealand, 2005. [Google Scholar]
- McLachlan, C.; Fleer, M.; Edwards, S. Early Childhood Curriculum: Planning, Assessment and Implementation, 2nd ed.; Cambridge University Press: Port Melbourne, VIC, Australia, 2013. [Google Scholar]
- Van Der Horst, K.; Paw, M.J.; Twisk, J.W.; Van Mechelen, W. A brief review on correlates of physical activity and sedentariness in youth. Med. Sci. Sports Exerc. 2007, 39, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents: Review of associated health benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef]
- Barnett, L.M.; Van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Does childhood motor skill proficiency predict adolescent fitness? Med. Sci. Sports Exerc. 2008, 40, 2137. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood motor skill proficiency as a predictor of adolescent physical activity. J. Adolesc. Health 2009, 44, 252–259. [Google Scholar] [CrossRef]
- Piek, J.P.; Baynam, G.B.; Barrett, N.C. The relationship between fine and gross motor ability, self-perceptions and self-worth in children and adolescents. Hum. Mov. Sci. 2006, 25, 65–75. [Google Scholar] [CrossRef]
- Barnett, L.M.; Morgan, P.J.; van Beurden, E.; Beard, J.R. Perceived sports competence mediates the relationship between childhood motor skill proficiency and adolescent physical activity and fitness: A longitudinal assessment. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 40. [Google Scholar] [CrossRef]
- Alhassan, S.; St. Laurent, C.W.; Burkart, S.; Greever, C.J.; Ahmadi, M.N. Feasibility of integrating physical activity into early education learning standards on preschooler’s physical activity levels. J. Phys. Act. Health 2019, 16, 101–107. [Google Scholar] [CrossRef]
- Matvienko, O.; Ahrabi-Fard, I. The effects of a 4-week after-school program on motor skills and fitness of kindergarten and first-grade students. Am. J. Health Promot. 2010, 24, 299–303. [Google Scholar] [CrossRef]
- Reilly, J.J.; Kelly, L.; Montgomery, C.; Williamson, A.; Fisher, A.; McColl, J.H.; Lo Conte, R.; Paton, J.Y.; Grant, S. Physical activity to prevent obesity in young children: Cluster randomised controlled trial. BMJ 2006, 333, 1041. [Google Scholar] [CrossRef]
- Altunsöz, I.H. Motor skills interventions for young children. Niğde Univ. J. Phys. Educ. Sport Sci. 2015, 9, 133–148. [Google Scholar]
- Brian, A.; Taunton, S. Effectiveness of motor skill intervention varies based on implementation strategy. Phys. Educ. Sport Pedagog. 2017, 23, 222–233. [Google Scholar] [CrossRef]
- Ulrich, D.A. Test of Gross Motor Development 2: Examiner’s Manual, 2nd ed.; Pro-ED Inc.: Austin, TX, USA, 2000. [Google Scholar]
- Rey, E.; Carballo-Fazanes, A.; Varela-Casal, C.; Abelairas-Gomez, C.; Collaborators A-MP. Reliability of the test of gross motor development: A systematic review. PLoS ONE 2020, 15, e0236070. [Google Scholar] [CrossRef]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Wong, W.W.; Lee, J.S.; Adolph, A.L.; Puyau, M.R.; Zakeri, I.F. Prediction of energy expenditure and physical activity in preschoolers. Med. Sci. Sports Exerc. 2014, 46, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- Kordi, R.; Nourian, R.; Ghayour, M.; Kordi, M.; Younesian, A. Development and evaluation of a basic physical and sports activity program for preschool children in nursery schools in Iran: An interventional study. Iran. J. Pediatr. 2012, 22, 357–363. [Google Scholar] [PubMed]
- Aye, T.; Oo, K.S.; Khin, M.T.; Kuramoto-Ahuja, T.; Maruyama, H. Gross motor skill development of 5-year-old Kindergarten children in Myanmar. J. Phys. Ther. Sci. 2017, 29, 1772–1778. [Google Scholar] [CrossRef][Green Version]
- Tomaz, S.A.; Jones, R.A.; Hinkley, T.; Bernstein, S.L.; Twine, R.; Kahn, K.; Norris, S.A.; Draper, C.E. Gross motor skills of South African preschool-aged children across different income settings. J. Sci. Med. Sport 2019, 22, 689–694. [Google Scholar] [CrossRef]
- Goodway, J.D.; Rudisill, M.E. Perceived physical competence and actual motor skill competence of African American preschool children. Adapt. Phys. Activ. Q. 1997, 14, 314–326. [Google Scholar] [CrossRef]
- Apache, R.R. Activity-based intervention in motor skill development. Percept. Mot. Skills 2005, 100 (Suppl. 3), 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Leis, A.; Ward, S.; Vatanparast, H.; Humbert, M.L.; Chow, A.F.; Muhajarine, N.; Engler-Stringer, R.; Belanger, M. Effectiveness of the Healthy Start-Depart Sante approach on physical activity, healthy eating and fundamental movement skills of preschoolers attending childcare centres: A randomized controlled trial. BMC Public Health 2020, 20, 523. [Google Scholar] [CrossRef] [PubMed]
- Vučić, A.; Bilić-Kirin, V. Impact of physical activity and sports on academic achievement of students in primary and secondary schools in Osijek-Baranja County, Croatia. Southeast. Eur. Med. J. 2020, 4, 97–107. [Google Scholar] [CrossRef]
- Chomitz, V.R.; Slining, M.M.; McGowan, R.J.; Mitchell, S.E.; Dawson, G.F.; Hacker, K.A. Is there a relationship between physical fitness and academic achievement? Positive results from public school children in the northeastern United States. J. Sch. Health 2009, 79, 30–37. [Google Scholar] [CrossRef]
- Castelli, D.M.; Hillman, C.H.; Buck, S.M.; Erwin, H.E. Physical fitness and academic achievement in third- and fifth-grade students. J. Sport Exerc. Psychol. 2007, 29, 239–252. [Google Scholar] [CrossRef]
- Chaddock-Heyman, L.; Erickson, K.I.; Kienzler, C.; King, M.; Pontifex, M.B.; Raine, L.B.; Hillman, C.H.; Kramer, A.F. The role of aerobic fitness in cortical thickness and mathematics achievement in preadolescent children. PLoS ONE 2015, 10, e0134115. [Google Scholar] [CrossRef]
- Voss, M.W.; Chaddock, L.; Kim, J.S.; Vanpatter, M.; Pontifex, M.B.; Raine, L.B.; Cohen, N.J.; Hillman, C.H.; Kramer, A.F. Aerobic fitness is associated with greater efficiency of the network underlying cognitive control in preadolescent children. Neuroscience 2011, 199, 166–176. [Google Scholar] [CrossRef]
- de Waal, E. Fundamental movement skills and academic performance of 5- to 6-year-old preschoolers. Early Child. Educ. J. 2019, 47, 455–464. [Google Scholar] [CrossRef]
- Lai, N.K.; Ang, T.F.; Por, L.Y.; Liew, C.S. The impact of play on child development-A literature review. Eur. Early Child. Educ. Res. J. 2018, 26, 625–643. [Google Scholar] [CrossRef]
- De Bruijn, A.G.M.; Kostons, D.D.N.M.; Van Der Fels, I.M.J.; Visscher, C.; Oosterlaan, J.; Hartman, E.; Bosker, R.J. Effects of aerobic and cognitively-engaging physical activity on academic skills: A cluster randomized controlled trial. J. Sports Sci. 2020, 38, 1806–1817. [Google Scholar] [CrossRef]
- Bardid, F.; Lenoir, M.; Huyben, F.; De Martelaer, K.; Seghers, J.; Goodway, J.D.; Deconinck, F.J.A. The effectiveness of a community-based fundamental motor skill intervention in children aged 3–8 years: Results of the “Multimove for Kids” project. J. Sci. Med. Sport 2017, 20, 184–189. [Google Scholar] [CrossRef]
- Ali, A.; McLachlan, C.; Mugridge, O.; McLaughlin, T.; Conlon, C.; Clarke, L. The effect of a 10-week physical activity programme on fundamental movement skills in 3–4-year-old children within early childhood education centres. Children 2021, 8, 440. [Google Scholar] [CrossRef]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the fundamentals of movement: A meta-analysis of the effectiveness of motor skill interventions in children. Child. Care Health Dev. 2012, 38, 305–315. [Google Scholar] [CrossRef]
- Hardy, L.L.; King, L.; Kelly, B.; Farrell, L.; Howlett, S. Munch and Move: Evaluation of a preschool healthy eating and movement skill program. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 80. [Google Scholar] [CrossRef] [PubMed]
- Maiano, C.; Hue, O.; April, L. Effects of motor skill interventions on fundamental movement skills in children and adolescents with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2019, 63, 1163–1179. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Stanley, R.M.; Jones, R.A.; Cliff, D.P.; Trost, S.G.; Berthelsen, D.; Salmon, J.; Batterham, M.; Eckermann, S.; Reilly, J.J.; et al. ‘Jump start’ childcare-based intervention to promote physical activity in pre-schoolers: Six-month findings from a cluster randomised trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; McNeill, J.; Vella, S.; Howard, S.J.; Kelly, M.A.; Angus, D.J.; Wright, I.M.; Santos, R.; Batterham, M.; Melhuish, E.; et al. The Preschool Activity, Technology, Health, Adiposity, Behaviour and Cognition (PATH-ABC) cohort study: Rationale and design. BMC Pediatr. 2017, 17, 95. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Male | Female | |
|---|---|---|---|
| Total Participants | 84 | 47 (56%) | 37 (44%) |
| Age (y) | 4.02 ± 0.57 | 3.98 ± 0.62 | 4.08 ± 0.50 |
| Height (cm) | 104.14 ± 5.77 | 103.20 ± 5.39 | 105.60 ± 6.26 |
| Weight (kg) | 18.74 ± 3.42 | 18.41 ± 3.45 | 19.25 ± 3.45 |
| Participated in TGMD-2 | 81 | 45 (56%) | 36 (44%) |
| Age (y) | 4.00 ± 0.56 | 3.94 ± 0.60 | 4.07 ± 0.51 |
| Height (cm) | 104.14 ± 5.77 | 103.20 ± 5.39 | 105.60 ± 6.26 |
| Weight (kg) | 18.74 ± 3.42 | 18.41 ± 3.45 | 19.25 ± 3.45 |
| Participated in accelerometry | 53 | 33 (62%) | 20 (38%) |
| Age (y) | 4.00 ± 0.56 | 3.88 ± 0.62 | 4.21 ± 0.39 |
| Height (cm) | 103.68 ± 5.64 | 102.09 ± 5.28 | 107.82 ± 4.67 |
| Weight (kg) | 18.01 ± 2.29 | 17.23 ± 1.57 | 20.04 ± 2.78 |
| Participated in TGMD-2 and accelerometry | 50 | 31 (62%) | 19 (38%) |
| Age (y) | 3.97 ± 0.55 | 3.82 ± 0.58 | 4.21 ± 0.41 |
| Height (cm) | 103.68 ± 5.64 | 102.09 ± 5.28 | 107.82 ± 4.67 |
| Weight (kg) | 18.01 ± 2.29 | 17.23 ± 1.57 | 20.04 ± 2.78 |
| Total (n = 81) | Male (n = 45) | Female (n = 36) | p Value * | |
|---|---|---|---|---|
| Gross Motor Quotient | 104.04 ± 14.53 | 104.33 ± 14.59 | 103.67 ± 14.65 | 0.839 |
| TGMD-2 Locomotor | 27.47 ± 10.02 | 26.73 ± 8.76 | 28.39 ± 11.45 | 0.463 |
| Locomotor Standard Score | 10.93 ± 3.26 | 10.76 ± 2.94 | 11.14 ± 3.66 | 0.602 |
| Locomotor Percentile | 63.00 (37.00, 91.00) | 50.00 (37.00, 84.00) | 63.00 (37.00, 91.00) | 0.509 |
| Locomotor Age Equivalent | 4.60 (3.30, 6.00) | 4.50 (3.25, 5.50) | 4.68 (3.63, 6.25) | 0.344 |
| TGMD-2 Object Control Skill | 23.46 ± 8.36 | 25.29 ± 8.74 | 21.17 ± 7.35 | 0.026 a |
| Object Control Standard Score | 10.00 (9.00, 12.00) | 10.00 (9.00, 13.00) | 10.00 (9.00, 12.00) | 0.293 |
| Object Control Percentile | 50.00 (37.00, 75.00) | 50.00 (37.00, 84.00) | 50.00 (37.00, 75.00) | 0.323 |
| Object Control Age Equivalent | 4.25 (3.25, 5.00) | 4.75 (3.00, 5.25) | 4.25 (3.25, 5.00) | 0.588 |
| Total (n = 53) | Male (n = 33) | Female (n = 20) | p Value * | |
|---|---|---|---|---|
| Average kCal per hour | 8.65 ± 4.30 | 8.15 ± 4.10 | 9.47 ± 4.60 | 0.468 |
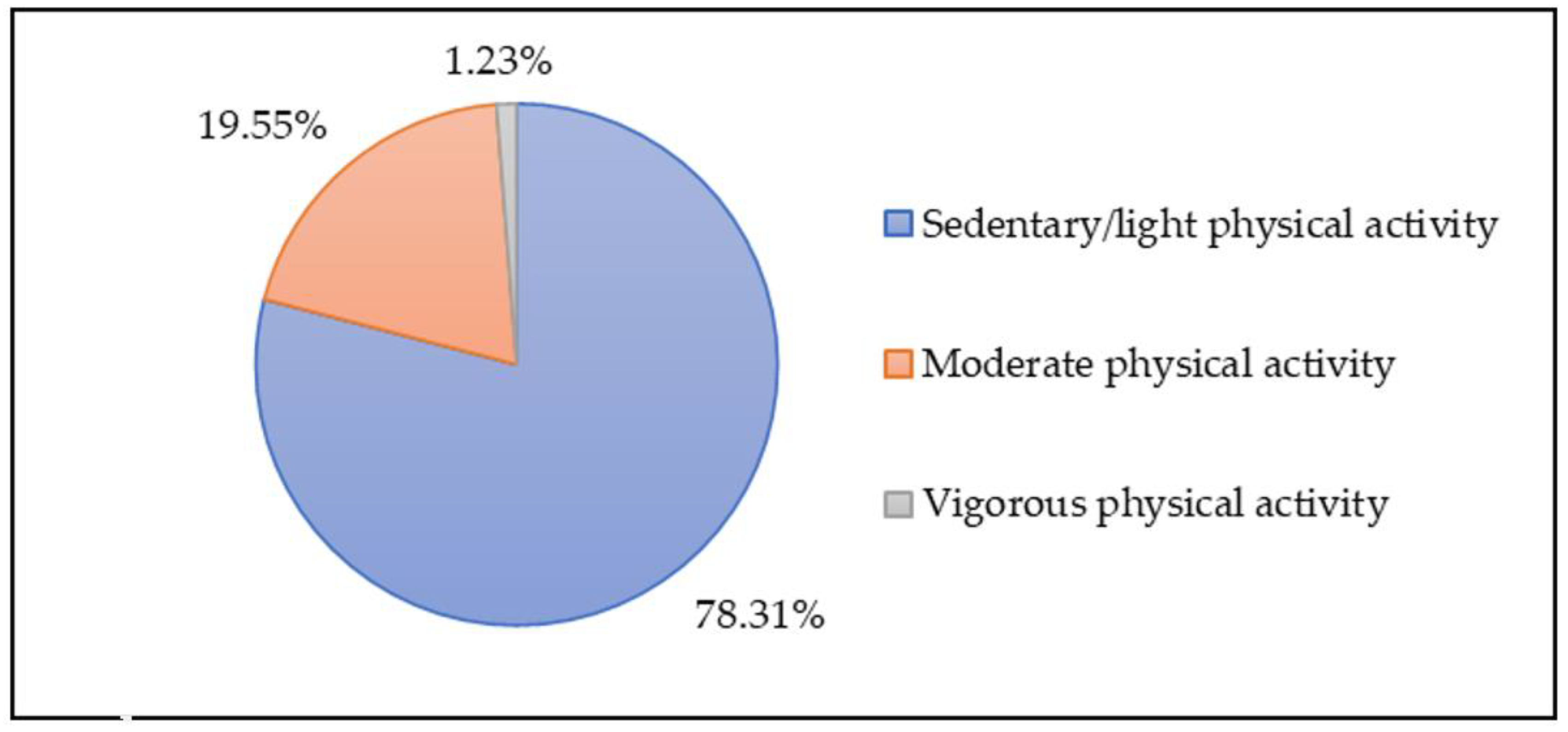
| % of sedentary/light activity | 78.31 ± 9.63 | 77.97 ± 9.57 | 78.88 ± 9.96 | 0.984 |
| % of moderate activity | 19.55 ± 8.87 | 19.92 ± 8.90 | 18.94 ± 9.01 | 0.827 |
| % of vigorous activity | 1.23 (0.83, 2.39) | 1.23 (0.78, 2.16) | 1.27 (0.90, 2.43) | 0.819 |
| Descriptive Rating of Gross Motor Quotient, n (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Group b | Age, Years | Locomotor Standard Scores | Object Control Skills Standard Scores | Gross Motor Quotient | Very Superior (>130) | Superior (121–130) | Above Average (111–120) | Average (90–110) | Below Average (80–89) | Poor (70–79) | Very Poor (<70) |
| Present study | Total (n = 81) | 3–4-year-old preschool children, New Zealand | 10.93 ± 3.26 | 10.00 (9.00, 12.00) | 104.04 ± 14.53 | 1 (1.2) | 14 (17.3) | 11 (13.6) | 42 (51.9) | 9 (11.1) | 4 (4.9) | 0 (0) |
| Male (n = 45) | 10.76 ± 2.94 | 10.00 (9.00, 13.00) | 104.33 ± 14.59 | 1 (2.2) | 9 (20.0) | 7 (15.6) | 20 (44.4) | 7 (15.6) | 1 (2.2) | 0 (0) | ||
| Female (n = 36) | 11.14 ± 3.66 | 10.00 (9.00, 12.00) | 103.67 ± 14.65 | 0 (0) | 5 (13.9) | 4 (11.1) | 22 (61.1) | 2 (5.6) | 3 (8.3) | 0 (0) | ||
| Aye, Oo [48] | Total (n = 472) | 5-year-old, kindergarten children, Myanmar | 12.8 ± 3.61 | 10.1 ± 2.81 | 108.3 ± 16.0 | 32 (6. 8) | 83 (17.6) | 95 (20.1) | 218 (46.2) | 29 (6.1) | 12 (2.5) | 3 (0.6) |
| Male (n = 237) | 12.9 ± 3.74 | 10.0 ± 2.65 | 108.3 ± 16.3 | NA | NA | NA | NA | NA | NA | NA | ||
| Female (n = 235) | 12.6 ± 3.48 | 10.2 ± 2.95 | 108.4 ± 15.8 | NA | NA | NA | NA | NA | NA | NA | ||
| Goodway, Rudisill [50] | Male (n = 30) | 4-year-old, preschool children, African American | 10.43 ± 2.5 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Female (n = 29) | 11.38 ± 2.69 | NA | NA | NA | NA | NA | NA | NA | NA | NA | ||
| Kordi, Nourian [47] | Baseline (n = 147) | 3–6-year-old, preschool children, Iran | 9 ± 4 | 9 ± 3 | 93.3 ± 18.9 | 3 (2) | 14 (9.5) | 8 (5.4) | 61 (41.5) | 22 (15) | 27 (18.4) | 12 (8.2) |
| Male (n = 75) | NA | NA | 91.2 ± 17.3 | NA | NA | NA | NA | NA | NA | NA | ||
| Female (n = 72) | NA | NA | 95.5 ± 20.3 | NA | NA | NA | NA | NA | NA | NA | ||
| Tomaz, Bernstein [49] | Total (n = 259) | 3–6-year-old, preschool children, South African | 11.3 ± 2.5 | 10.6 ± 2.3 | 105.5 ± 12.0 | 4 (1.5) | 20 (7.7) | 61 (23.6) | 156 (60.2) | 13 (5.0) | 3 (1.2) | 2 (0.8) |
| Male (n = 130) | 11.4 ± 2.3 | 10.4 ± 1.9 | 105.1 ± 10.2 | 1 (0.8) | 7 (5.4) | 31 (23.9) | 85 (65.4) | 4 (3.1) | 2 (1.5) | 0 (0) | ||
| Female (n = 129) | 11.3 ± 2.7 | 10.8 ± 2.5 | 105.8 ± 13.6 | 3 (2.3) | 13 (10.1) | 30 (23.3) | 71 (55.0) | 9 (7.0) | 1 (0.8) | 2 (1.6) | ||
| Apache [51] | Baseline 1 (n = 28) | 3–6-year-old, preschool children with disabilities, Las Vegas | 10.2 ± 3.3 | 8.6 ± 1.7 | NA | NA | NA | NA | NA | NA | NA | NA |
| Baseline 2 (n = 28) | 10.9 ± 3.6 | 9.7 ± 2.8 | NA | NA | NA | NA | NA | NA | NA | NA | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, A.; McLachlan, C.; McLaughlin, T.; Mugridge, O.; Conlon, C.; Mumme, K.; Knightbridge-Eager, T. Fundamental Movement Skills and Physical Activity of 3–4-Year-Old Children within Early Childhood Centers in New Zealand. Children 2021, 8, 742. https://doi.org/10.3390/children8090742
Ali A, McLachlan C, McLaughlin T, Mugridge O, Conlon C, Mumme K, Knightbridge-Eager T. Fundamental Movement Skills and Physical Activity of 3–4-Year-Old Children within Early Childhood Centers in New Zealand. Children. 2021; 8(9):742. https://doi.org/10.3390/children8090742
Chicago/Turabian StyleAli, Ajmol, Claire McLachlan, Tara McLaughlin, Owen Mugridge, Cathryn Conlon, Karen Mumme, and Tayla Knightbridge-Eager. 2021. "Fundamental Movement Skills and Physical Activity of 3–4-Year-Old Children within Early Childhood Centers in New Zealand" Children 8, no. 9: 742. https://doi.org/10.3390/children8090742
APA StyleAli, A., McLachlan, C., McLaughlin, T., Mugridge, O., Conlon, C., Mumme, K., & Knightbridge-Eager, T. (2021). Fundamental Movement Skills and Physical Activity of 3–4-Year-Old Children within Early Childhood Centers in New Zealand. Children, 8(9), 742. https://doi.org/10.3390/children8090742