
Segmental Assessment of Trunk Control in Moderate-to-Late Preterm Infants Related to Sitting Development

 ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement Instruments
2.2.1. Segmental Assessment of Trunk Control (SATCo)
2.2.2. Alberta Infant Motor Scale (AIMS)
2.3. Ethical Clearance
2.4. Procedure
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO Multicentre Growth Reference Study Group. WHO Motor Development Study: Windows of achievement for six gross motor development milestones. Acta Paediatr. 2006, 95, 86–95. [Google Scholar] [CrossRef]
- Karasik, L.B.; Tamis-LeMonda, C.S.; Adolph, K.E.; Bornstein, M.H. Places and postures: A cross-cultural comparison of sitting in 5-month-olds. J. Cross-Cult Psychol. 2015, 46, 1023–1038. [Google Scholar] [CrossRef] [Green Version]
- De Groot, L.; Hopkins, B.; Touwen, B. Muscle power, sitting unsupported and trunk rotation in pre-term infants. Early Hum. Dev. 1995, 43, 37–46. [Google Scholar] [CrossRef]
- Wang, T.-N.; Howe, T.-H.; Hinojosa, J.; Hsu, Y.-W. Postural control of pre-term infants at 6 and 12 months corrected age. Early Hum. Dev. 2010, 86, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.T.; Tudella, E. Influence of sitting positions and level of trunk control during reaching movements in late preterm and full-term infants. Front. Pediatr. 2018, 6, 185. [Google Scholar] [CrossRef]
- Saavedra, S.L.; van Donkelaar, P.; Woollacott, M.H. Learning about gravity: Segmental assessment of upright control as infants develop independent sitting. J. Neurophysiol. 2012, 108, 2215–2229. [Google Scholar] [CrossRef]
- Duncan, K.; Goodworth, A.; Da Costa, C.S.N.; Wininger, M.; Saavedra, S. Parent handling of typical infants varies segmentally across development of postural control. Exp. Brain Res. 2018, 236, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.; Saavedra, M.S.; Sofranac, M.M.; Jarvis, M.S.; Woollacott, M. Refinement, reliability and validity of the segmental assessment of trunk control (SATCo). Pediatr. Phys. Ther. 2010, 22, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, A.L.R.; da Costa, C.S.N.; Tudella, E. Identifying the level of trunk control of healthy term infants aged from 6 to 9 months. Infant Behav. Dev. 2018, 50, 207–212. [Google Scholar] [CrossRef]
- Pin, T.W.; Butler, P.B.; Cheung, H.-M.; Shum, S.L.-F. Longitudinal Development of Segmental Trunk Control in Full Term and Preterm Infants- a Pilot Study: Part I. Dev. Neurorehabil. 2020, 23, 185–192. [Google Scholar] [CrossRef]
- Pin, T.W.; Butler, P.B.; Cheung, H.-M.; Shum, S.L.-F. Longitudinal Development of Segmental Trunk Control in Full Term and Preterm Infants-a Pilot Study: Part II. Dev. Neurorehabil. 2020, 23, 193–200. [Google Scholar] [CrossRef]
- Greco, A.L.R.; Sato, N.T.d.S.; Cazotti, A.M.; Tudella, E. Is Segmental Trunk Control Related to Gross Motor Performance in Healthy Preterm and Full-Term Infants? J. Mot. Behav. 2020, 52, 666–675. [Google Scholar] [CrossRef]
- De Vries, L.S.; Eken, P.; Dubowitz, L.M. The spectrum of leukomalacia using cranial ultrasound. Behav. Brain Res. 1992, 49, 1–6. [Google Scholar] [CrossRef]
- Papile, L.-A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatrics 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Pin, T.W.; Butler, P.B.; Cheung, H.M.; Shum, S.L. Segmental Assessment of Trunk Control in infants from 4 to 9 months of age- a psychometric study. BMC Pediatr. 2018, 18, 182. [Google Scholar] [CrossRef]
- Piper, M.; Darrah, J. Motor Assessment of the Developing Infant. Phila. WB Saunders 1994, 74, 110. [Google Scholar]
- Aimsamrarn, P.; Janyachareon, T.; Rattanathanthong, K.; Emasithi, A.; Siritaratiwat, W. Cultural translation and adaptation of the Alberta Infant Motor Scale Thai version. Early Hum. Dev. 2019, 130, 65–70. [Google Scholar] [CrossRef]
- Wijnhoven, T.M.A.; de Onis, M.; Onyango, A.W.; Wang, T.; Bjoerneboe, G.-E.A.; Bhandari, N.; Lartey, A.; Rashidi, B.A. Assessment of Gross Motor Development in the WHO Multicentre Growth Reference Study. Food Nutr. Bull. 2004, 25, S37–S45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009; Volume 892. [Google Scholar]
- Darrah, J.; Redfern, L.; Maguire, T.O.; Beaulne, A.P.; Watt, J. Intra-individual stability of rate of gross motor development in full-term infants. Early Hum. Dev. 1998, 52, 169–179. [Google Scholar] [CrossRef]
- Darrah, J.; Hodge, M.; Magill-Evans, J.; Kembhavi, G. Stability of serial assessments of motor and communication abilities in typically developing infants—implications for screening. Early Hum. Dev. 2003, 72, 97–110. [Google Scholar] [CrossRef]
- Darrah, J.; Senthilselvan, A.; Magill-Evans, J. Trajectories of serial motor scores of typically developing children: Implications for clinical decision making. Infant Behav. Dev. 2009, 32, 72–78. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Demographic Data | Mean (SD) | Range |
|---|---|---|
| Birth weight (g) | 2139.5 (406.7) | 1330–3092 |
| Birth length (cm) | 47.5 (1.7) | 44–50 |
| Birth head circumference (cm) | 30.4 (1.5) | 29–34 |
| Apgar Score at 5 min | 9.3 (0.5) | 8–10 |
| Average gestational age | 34.5 (1.5) | 32–36 |
| Corrected Age of Prematurity | SATCo Conditions | Level of Trunk Segment | Median | Range |
|---|---|---|---|---|
| 4 months | Static | Midthoracic | 3 | 2 to 5 |
| Active | Upper thoracic | 2 | 1 to 4 | |
| Reactive | Upper thoracic | 2 | 1 to 4 | |
| 5 months | Static | Lower thoracic | 4 | 3 to 6 |
| Active | Mid thoracic | 3 | 2 to 5 | |
| Reactive | Mid thoracic | 3 | 2 to 4 | |
| At age of independent sitting | Static | Full trunk | 7 | 5 to 7 |
| Active | Upper lumbar | 5 | 4 to 7 | |
| Reactive | Upper lumbar | 5 | 4 to 6 |
| AIMS | 4 Months | 5 Months | Age of Independent Sitting |
|---|---|---|---|
| Prone | 5.1 (1.2) | 7.6 (1.8) | 12.9 (2.2) |
| Supine | 5.9 (1.8) | 7.6 (1.2) | 9.0 (0.2) |
| Sitting | 2.4 (0.6) | 3.7 (1.0) | 7.3 (0.7) |
| Standing | 1.9 (0.3) | 2.0 (0.0) | 2.6 (1.4) |
| Total | 15.3 (2.8) | 21.0 (3.4) | 31.7 (3.6) |
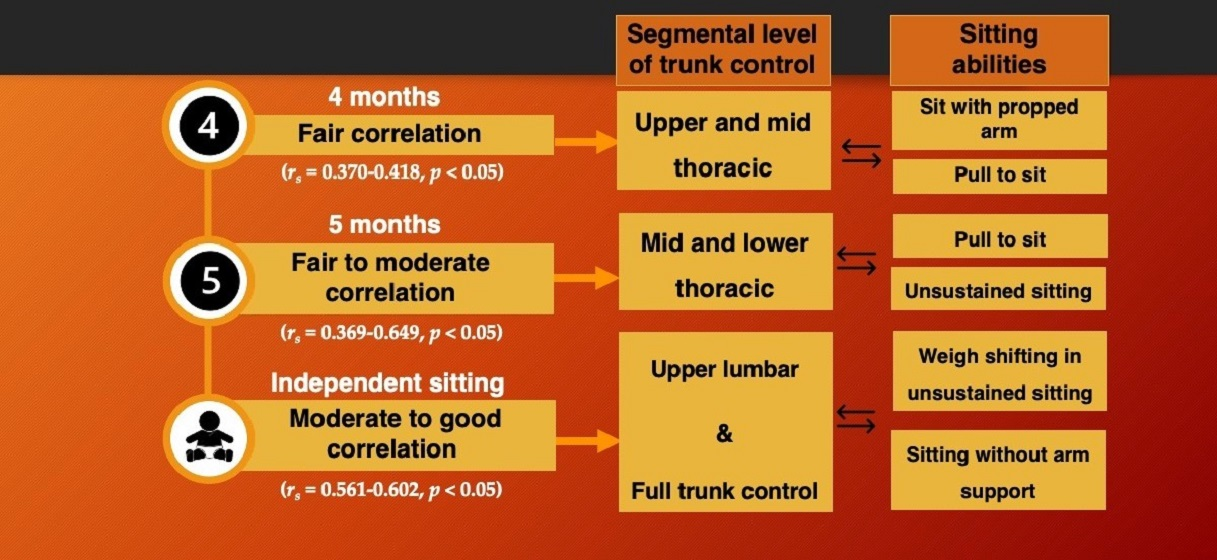
| SATCo | Correlation Coefficients (rs) | ||
|---|---|---|---|
| Conditions | 4-Month Corrected Age | 5-Month Corrected Age | Age of Independent Sitting |
| Static d (effect size) | 0.370 * | 0.369 * | 0.561 ** |
| 0.780 | 0.830 | 1.590 | |
| Active d (effect size) | 0.420 * | 0.400 * | 0.561 ** |
| 0.800 | 0.920 | 1.590 | |
| Reactive d (effect size) | 0.418 * | 0.649 ** | 0.602 ** |
| 0.980 | 2.180 | 1.830 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sangkarit, N.; Keeratisiroj, O.; Yonglitthipagon, P.; Bennett, S.; Siritaratiwat, W. Segmental Assessment of Trunk Control in Moderate-to-Late Preterm Infants Related to Sitting Development. Children 2021, 8, 722. https://doi.org/10.3390/children8090722
Sangkarit N, Keeratisiroj O, Yonglitthipagon P, Bennett S, Siritaratiwat W. Segmental Assessment of Trunk Control in Moderate-to-Late Preterm Infants Related to Sitting Development. Children. 2021; 8(9):722. https://doi.org/10.3390/children8090722
Chicago/Turabian StyleSangkarit, Noppharath, Orawan Keeratisiroj, Ponlapat Yonglitthipagon, Surussawadi Bennett, and Wantana Siritaratiwat. 2021. "Segmental Assessment of Trunk Control in Moderate-to-Late Preterm Infants Related to Sitting Development" Children 8, no. 9: 722. https://doi.org/10.3390/children8090722
APA StyleSangkarit, N., Keeratisiroj, O., Yonglitthipagon, P., Bennett, S., & Siritaratiwat, W. (2021). Segmental Assessment of Trunk Control in Moderate-to-Late Preterm Infants Related to Sitting Development. Children, 8(9), 722. https://doi.org/10.3390/children8090722