
Impact of Graft Size Matching on the Early Post-Transplant Complications and Patients Survival in Children after Living Donor Liver Transplantations

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Donors
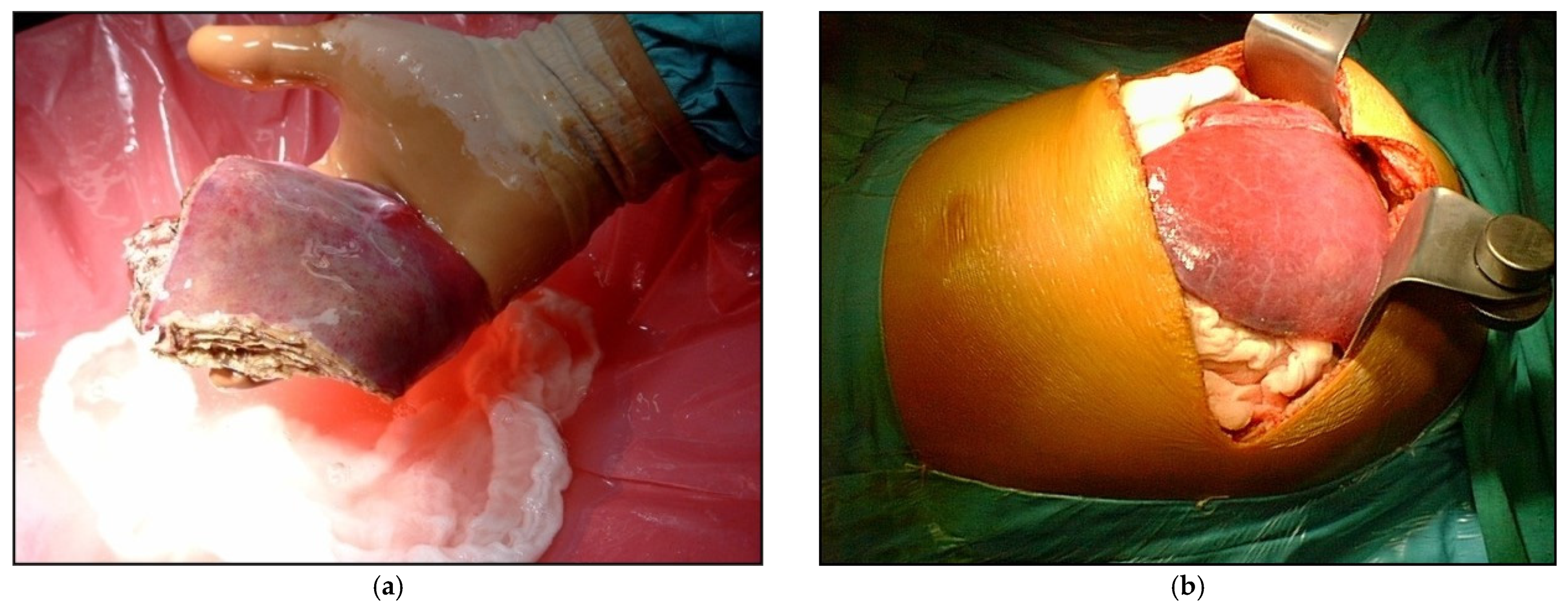
2.2. Recipient Surgery
2.3. Immunosuppressive Regimens
2.4. Statistical Analysis
3. Results
3.1. Recipients, Donors and Grafts
3.2. Postoperative Complications
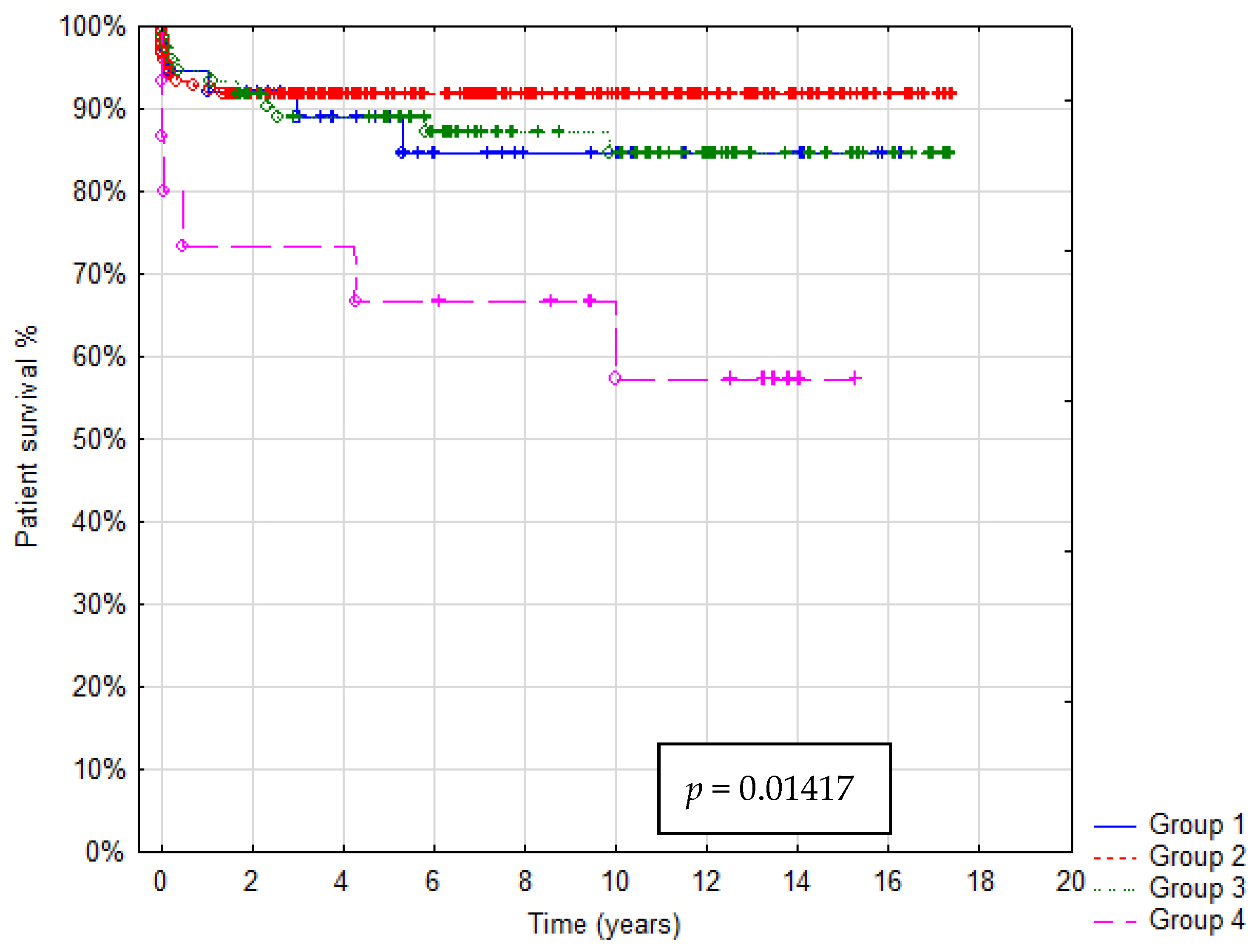
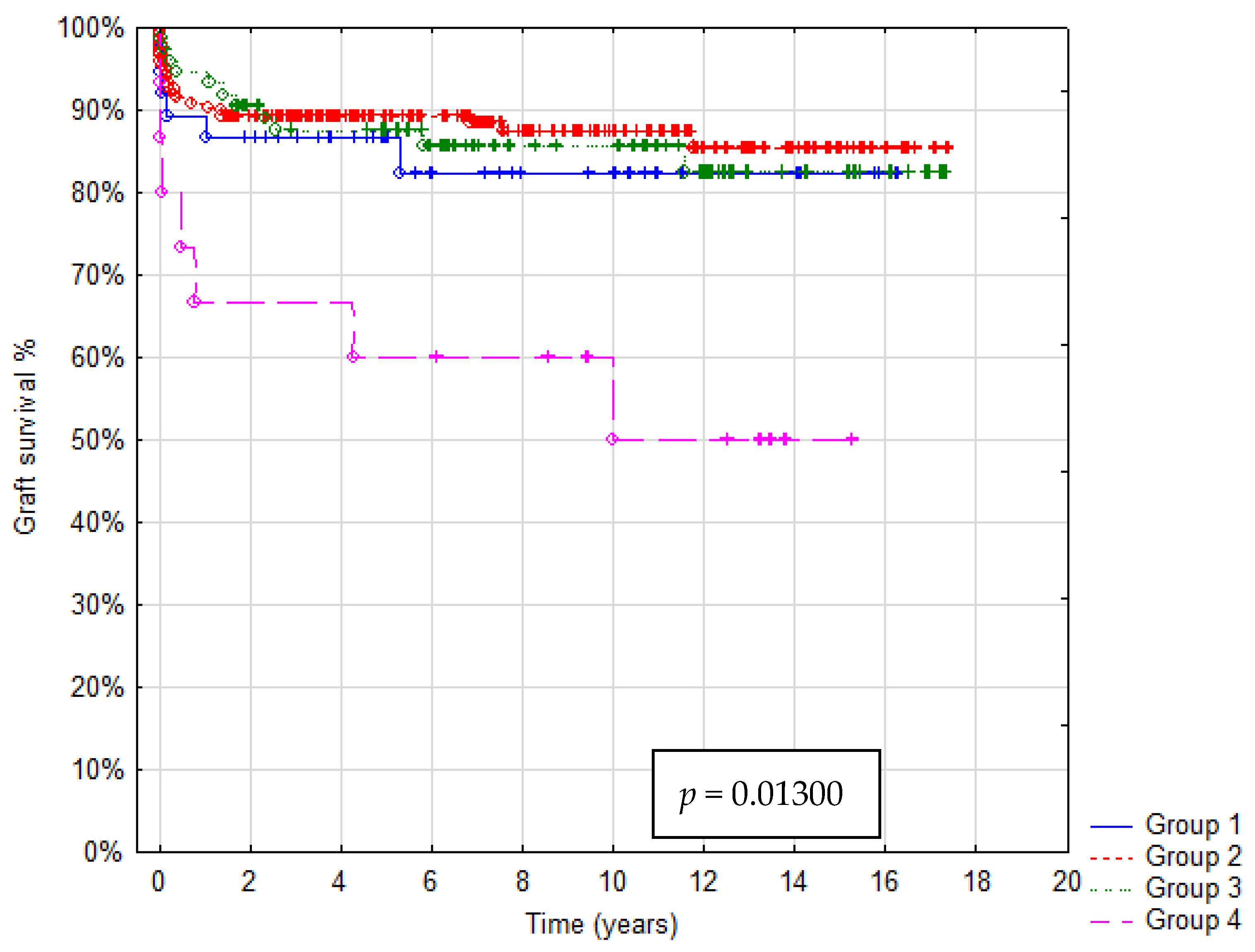
3.3. Patient and Graft Survival
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strong, R.W.; Lynch, S.V.; Ong, T.H.; Matsunami, H.; Koido, Y.; Balderson, G.A. Successful liver transplantation from a living donor to her son. N. Engl. J. Med. 1990, 322, 1505–1507. [Google Scholar] [CrossRef]
- Dahm, F.; Georgiev, P.; Clavien, P.A. Small-for-size syndrome after partial liver transplantation: Definition, mechanisms of disease and clinical implications. Am. J. Transplant. 2005, 5, 2605–2610. [Google Scholar] [CrossRef]
- Kiuchi, T.; Kasahara, M.; Uryuhara, K.; Inomata, Y.; Uemoto, S.; Asonuma, K.; Egawa, H.; Fujita, S.; Hayashi, M.; Tanaka, K. Impact of graft size mismatching on graft prognosis in liver transplantation from living donors. Transplantation 1999, 67, 321–327. [Google Scholar] [CrossRef]
- Moon, J.I.; Kwon, C.H.; Joh, J.W.; Jung, G.O.; Choi, G.S.; Park, J.B.; Kim, J.M.; Shin, M.; Kim, S.J.; Lee, S.K. Safety of small-for-size grafts in adult-to-adult living donor liver transplantation using the right lobe. Liver Transplant. 2010, 16, 864–869. [Google Scholar] [CrossRef]
- Urata, K.; Kawasaki, S.; Matsunami, H.; Hashikura, Y.; Ikegami, T.; Ishizone, S.; Momose, Y.; Komiyama, A.; Makuuchi, M. Calculation of child and adult standard liver volume for liver transplantation. Hepatology 1995, 21, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.F.; Chen, C.L.; Huang, T.L.; Chen, T.Y.; Chen, Y.S.; Takatsuki, M.; Wang, C.C.; Chiu, K.W.; Tsang, L.L.; Sun, P.L.; et al. Risk factors for intraoperative portal vein thrombosis in pediatric living donor liver transplantation. Clin. Transplant. 2004, 18, 390–394. [Google Scholar] [CrossRef]
- Kitajima, T.; Sakamoto, S.; Sasaki, K.; Narumoto, S.; Kazemi, K.; Hirata, Y.; Fukuda, A.; Imai, R.; Miyazaki, O.; Irie, R.; et al. Impact of graft thickness reduction of left lateral segment on outcomes following pediatric living donor liver transplantation. Am. J. Transplant. 2018, 18, 2208–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.J.; Zu, C.H.; Li, S.P.; Gao, W.; Shen, Z.Y.; Cai, J.Z. Effect of graft size matching on pediatric living-donor liver transplantation at a single center. Clin. Transplant. 2018, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehar, M.; Parekh, R.S.; Stunguris, J.; De Angelis, M.; Van Roestel, K.; Ghanekar, A.; Cattral, M.; Fecteau, A.; Ling, S.; Kamath, B.M.; et al. Superior Outcomes and Reduced Wait Times in Pediatric Recipients of Living Donor Liver Transplantation. Transplant. Direct 2019, 5, e430. [Google Scholar] [CrossRef]
- Goldaracena, N.; Echeverri, J.; Kehar, M.; DeAngelis, M.; Jones, N.; Ling, S.; Kamath, B.M.; Avitzur, Y.; Ng, V.L.; Cattral, M.S.; et al. Pediatric living donor liver transplantation with large-for-size left lateral segment grafts. Am. J. Transplant. 2020, 20, 504–512. [Google Scholar] [CrossRef]
- Wan, P.; Li, Q.; Zhang, J.; Shen, C.; Luo, Y.; Chen, Q.; Chen, X.; Zhang, M.; Han, L.; Xia, Q. Influence of graft size matching on outcomes of infantile living donor liver transplantation. Pediatr. Transplant. 2015, 19, 880–887. [Google Scholar] [CrossRef]
- Bonatti, H.; Muiesan, P.; Connelly, S.; Baker, A.; Mieli-Vergani, G.; Gibbs, P.; Heaton, N.; Rela, M. Hepatic transplantation in children under 3 months of age: A single centre’s experience. J. Pediatr. Surg. 1997, 32, 486–488. [Google Scholar] [CrossRef]
- Shirouzu, Y.; Kasahara, M.; Morioka, D.; Sakamoto, S.; Taira, K.; Uryuhara, K.; Ogawa, K.; Takada, Y.; Egawa, H.; Tanaka, K. Vascular reconstruction and complications in living donor liver transplantation in infants weighing less than 6 kg: The Kyoto experience. Liver Transplant. 2006, 12, 1224–1232. [Google Scholar] [CrossRef]
- Uchida, Y.; Sakamoto, S.; Egawa, H.; Ogawa, K.; Ogura, Y.; Taira, K.; Kasahara, M.; Uryuhara, K.; Takada, Y.; Kamiyama, Y.; et al. The impact of meticulous management for hepatic artery thrombosis on long-term outcome after pediatric living donor liver transplantation. Clin. Transplant. 2009, 23, 392–399. [Google Scholar] [CrossRef]
- Moon, J.I.; Jung, G.O.; Choi, G.S.; Kim, J.M.; Shin, M.; Kim, E.Y.; Kwon, C.H.; Kim, S.J.; Joh, J.W.; Lee, S.K. Risk factors for portal vein complications after pediatric living donor liver transplantation with left-sided grafts. Transplant. Proc. 2010, 42, 871–875. [Google Scholar] [CrossRef]
- Neto, J.S.; Fonseca, E.A.; Feier, F.H.; Pugliese, R.; Candido, H.L.; Benavides, M.R.; Porta, G.; Miura, I.K.; Danesi, V.B.; Guimaraes, T.; et al. Analysis of factors associated with portal vein thrombosis in pediatric living donor liver transplant recipients. Liver Transplant. 2014, 20, 1157–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutluturk, K.; Sahin, T.T.; Karakas, S.; Unal, B.; Gozukara Bag, H.G.; Akbulut, S.; Aydin, C.; Yilmaz, S. Early Hepatic Artery Thrombosis After Pediatric Living Donor Liver Transplantation. Transplant. Proc. 2019, 51, 1162–1168. [Google Scholar] [CrossRef]
- Ueda, M.; Oike, F.; Kasahara, M.; Ogura, Y.; Ogawa, K.; Haga, H.; Takada, Y.; Egawa, H.; Tanaka, K.; Uemoto, S. Portal vein complications in pediatric living donor liver transplantation using left-side grafts. Am. J. Transplant. 2008, 8, 2097–2105. [Google Scholar] [CrossRef]
- Jung, D.H.; Ikegami, T.; Balci, D.; Bhangui, P. Biliary reconstruction and complications in living donor liver transplantation. Int. J. Surg. 2020, 82S, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Karam, V.; Cailliez, V.; JG, O.G.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)—50-year evolution of liver transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, N.; Sanada, Y.; Onishi, Y.; Urahashi, T.; Ihara, Y.; Yamada, N.; Hirata, Y.; Katano, T.; Imai, T.; Ushijima, K.; et al. The Causes and Outcomes of Early Relaparotomy Following Pediatric Living Donor Liver Transplantation. Liver Transplant. 2019, 25, 1066–1073. [Google Scholar] [CrossRef]
- Bourdeaux, C.; Brunati, A.; Janssen, M.; de Magnee, C.; Otte, J.B.; Sokal, E.; Reding, R. Liver retransplantation in children. A 21-year single-center experience. Transpl. Int. 2009, 22, 416–422. [Google Scholar] [CrossRef]
- Dreyzin, A.; Lunz, J.; Venkat, V.; Martin, L.; Bond, G.J.; Soltys, K.A.; Sindhi, R.; Mazariegos, G.V. Long-term outcomes and predictors in pediatric liver retransplantation. Pediatr. Transplant. 2015, 19, 866–874. [Google Scholar] [CrossRef]
- Kanazawa, H.; Sakamoto, S.; Fukuda, A.; Uchida, H.; Hamano, I.; Shigeta, T.; Kobayashi, M.; Karaki, C.; Tanaka, H.; Kasahara, M. Living-donor liver transplantation with hyperreduced left lateral segment grafts: A single-center experience. Transplantation 2013, 95, 750–754. [Google Scholar] [CrossRef]
- Masuda, Y.; Yoshizawa, K.; Ohno, Y.; Mita, A.; Shimizu, A.; Soejima, Y. Small-for-size syndrome in liver transplantation: Definition, pathophysiology and management. Hepatobiliary Pancreat. Dis. Int. 2020, 19, 334–341. [Google Scholar] [CrossRef]
- Linares, I.; Goldaracena, N.; Rosales, R.; Maza, L.; Kaths, M.; Kollmann, D.; Echeverri, J.; Selzner, N.; McCluskey, S.A.; Sapisochin, G.; et al. Splenectomy as Flow Modulation Strategy and Risk Factors of De Novo Portal Vein Thrombosis in Adult-to-Adult Living Donor Liver Transplantation. Liver Transplant. 2018, 24, 1209–1220. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| GRWR Cutoff Value | Number of Patients | Overall Survival (%) | χ2 | Log-Rank Test p-Value |
|---|---|---|---|---|
| <1 vs. ≥ 1 | 3 vs. 317 | 100 vs. 88.33 | 0.00013588 | 0.54246 |
| <1.5 vs. ≥ 1.5 | 37 vs. 283 | 86.11 vs. 88.73 | 0.20301664 | 0.65271 |
| <2 vs. ≥ 2 | 93 vs. 227 | 89.25 vs. 88.11 | 0.06631477 | 0.79707 |
| <2.5 vs. ≥ 2.5 | 143 vs. 177 | 90.21 vs. 87.01 | 0.64005114 | 0.42278 |
| <3 vs. ≥ 3 | 184 vs. 136 | 91.30 vs. 84.56 | 3.03766444 | 0.07729 |
| <3.5 vs. ≥ 3.5 | 232 vs. 88 | 90.95 vs. 81.82 | 4.18125661 * | 0.03652 |
| <4 vs. ≥ 4 | 271 vs. 49 | 89.30 vs. 83.67 | 0.97788367 | 0.31531 |
| <4.5 vs. ≥ 4.5 | 293 vs. 27 | 89.42 vs. 77.78 | 2.74998956 | 0.08962 |
| <5 vs. ≥ 5 | 305 vs. 15 | 89.84 vs. 60.00 | 11.0518162 * | 0.00055 |
| Diagnosis | Group A (n = 37) GRWR ≤ 1.5% | Group B (n = 196) >1.5% GRWR ≤ 3.5% | Group C (n = 73) >3.5% GRWR < 5% | Group D (n = 15) GRWR ≥ 5% | Total (n = 321) |
|---|---|---|---|---|---|
| Cholestatic disease Biliary atresia | 15 (40.6%) | 120 (61.2%) | 56 (76.7%) | 12 (80%) | 203 (63.2%) |
| 13 (35.1%) | 104 (53.1%) | 55 (75.3%) | 11 (73.3%) | 184 (57.3%) | |
| Liver tumors | 4 (10.8%) | 33 (16.8%) | 6 (8.3%) | 1 (6.7%) | 44 (13.7%) |
| Acute liver failure | 4 (10.8%) | 21 (10.7%) | 0 | 2 (13.3%) | 27 (8.4%) |
| Metabolic disorders | 2 (5.4%) | 6 (3.1%) | 2 (2.7%) | 0 | 10 (3.2%) |
| Others | 12 (32.4%) | 16 (8.2%) | 9 (12.3%) | 0 | 37 (11.5%) |
| Characteristics | Group A (n = 37) GRWR ≤ 1.5% | Group B (n = 196) >1.5% GRWR ≤ 3.5% | Group C (n = 73) >3.5% GRWR < 5% | Group D (n = 15) GRWR ≥ 5% | p-Value |
|---|---|---|---|---|---|
| Recipients | |||||
| Age (months), median (range) <1 year | 78 (5–184) | 17 (5–176) | 8 (3–29) | 6 (0.5–11) | p < 0.001 |
| 1 (2.7%) | 62 (31.6%) | 61 (83.6%) | 15 (100%) | ||
| Body mass (kg); median (range) | 22.5 (12.8–45) | 10 (4–47) | 7 (4.5–12.3) | 5.6 (3.1–7.8) | p < 0.001 |
| PELD score median (range) | 7 (−9–38) | 13 (−11–41) | 21 (−9–38) | 20 (4–42) | p < 0.0001 |
| AB0i LDLT | 4 (10.8%) | 29 (14.8%) | 16 (21.9%) | 4 (26.7%) | 0.226 |
| Urgent LDLT | 6 (16.2%) | 24 (12.2%) | 1 (1.4%) | 3 (20%) | p < 0.021 |
| Donors | |||||
| Age (year); median (range) | 33 (21–57) | 31 (19– 54) | 31 (18–56) | 32 (21–44) | p < 0.05 |
| Body mass (kg); median (range) | 67.5 (50–106) | 65 (45–110) | 68 (46–106) | 67 (54–90) | p = 0.2849 |
| Graft weight (g); median (range) | 280 (158–615) | 252 (131–919) | 275 (198–506) | 320 (212–507) | p < 0.0001 |
| GRWR (%); median (range) | 1.35 (0.86–1.5) | 2.42 (1.51–3.49) | 3.98 (3.52–4.94) | 5.54 (5–10.68) | p < 0.05 |
| Operation | Group A (n = 37) GRWR ≤ 1.5% | Group B (n = 196) >1.5% GRWR ≤ 3.5% | Group C (n = 73) >3.5% GRWR < 5% | Group D (n = 15) GRWR ≥ 5% | Total (n = 321) |
|---|---|---|---|---|---|
| Graft type | |||||
| Monosegment | 0 | 4 | 5 | 1 | 10 (3.1%) |
| Left lateral segment | 17 | 178 | 68 | 14 | 277 (86.3%) |
| Left lobe | 19 | 13 | 0 | 0 | 32 (10%) |
| Right lobe | 1 | 1 | 0 | 0 | 2 (0.6%) |
| Biliary anastomosis | |||||
| Roux-en-Y hepaticojejunostomy | 28 | 164 | 70 | 14 | 276 (86%) |
| Duct to duct anastomosis | 9 | 32 | 3 | 1 | 45 (14%) |
| Cold ischemic time (min); median (range) | 296 (210–450) | 265 (183–485) | 270 (200–383) | 287 (240–315) |
| Group A (37) GRWR ≤ 1.5% | Group B (196) >1.5% GRWR ≤ 3.5% | Group C (73) >3.5% GRWR < 5% | Group D (15) GRWR ≥ 5% | Total | p-Value | |
|---|---|---|---|---|---|---|
| Hepatic artery thrombosis | ||||||
| Early (%) | 1 (2.7%) | 13 (6.6%) | 2 (2.7%) | 0 | 16 (5.0%) | p = 0.338 |
| Rethrombosis after trombectomy (%) | 0 | 2 (1%) | 1 (1.4%) | 0 | 3 (0.9%) | |
| Portal vein thrombosis | ||||||
| Early (%) | 4 (10.8%) | 12 (6.1%) | 10 (13.7%) | 1 (6.7%) | 27 (8.4%) | p = 0.229 |
| Rethrombosis after trombectomy (%) | 1 (2.7%) | 3 (1.5%) | 2 (2.7%) | 0 | 5 (1.6%) | |
| Biliary leaks | ||||||
| Biliary anastomosis | 6 (16.2%) | 19 (9.7%) | 8 (11%) | 0 | 33 (10.3%) | p = 0.502 |
| Cut surface of liver | 1 (2.7%) | 5 (2.6%) | 3 (4.1%) | 2 (13.3%) | 11 (3.4%) | p = 0.167 |
| Postoperative bleeding | 6 (16.2%) | 34 (17.3%) | 14 (19.2%) | 1 (6.7%) | 55 (17.1%) | p = 0.705 |
| Gastrointestinal perforations | 0 | 6 (3.1%) | 5 (6.8%) | 0 | 11 (3.4%) | p = 0.163 |
| Acute rejections | 14 (37.8%) | 77 (39.5%) | 31 (42.5%) | 5 (33.3%) | 127 (39.6%) | p = 0.907 |
| Abdominal wound closure * | ||||||
| Primary | 20 (58.8%) | 86 (48.0%) | 22 (30.6) | 2 (15.4%) | 130 (43.6%) | |
| Delayed Time to closure (days) | 14 (41.2%) 6 (2–9) | 93 (52.0%) 5 (2–65) | 50 (69.4%) 7 (1–63) | 11 (84.6%) 5 (4–123) | 168 (56.4%) | p < 0.005 |
| ICU stay (days) *; median (range) | 3 (2–27) | 4(2–62) | 5 (2–40) | 10 (3–48) | p < 0.001 | |
| Hospital stay (days) *; median (range) | 48.5 (17–324) | 35 (13–136) | 40 (12–167) | 37 (24–189) | p < 0.01 | |
| Re-Tx (%) | 2 (5.4%) | 9 (4.6%) | 2 (2.7%) | 2 (13.3%) | 15 (4.7%) | p = 0.364 |
| Cause of Retransplantation | Group A (n = 37) GRWR ≤ 1.5% | Group B (n = 196) >1.5% GRWR ≤ 3.5% | Group C (n = 73) >3.5% GRWR < 5% | Group D (n = 15) GRWR ≥ 5% | Total (n = 15) |
|---|---|---|---|---|---|
| HAT | 0 | 2 (2.4 months) | 0 | 0 | 2 (13.3%) |
| PVT | 1 (10 days) | 0 | 0 | 0 | 1 (6.7%) |
| Biliary complications | 0 | 2 (83.131 months) | 1 (17 months) | 1 (10 months) | 4 (26.7%) |
| Hyperacute rejection | 1 (2 days) | 1 (3 days) | 0 | 0 | 2 (13.3%) |
| Chronic rejection | 0 | 2 (5.16 months) | 0 | 1 (48 months) | 3 (20%) |
| Other causes | 0 | 2 (2.91 months) | 1 (139 months) | 0 | 3 (20%) |
| Variables | Adjusted OR (95% CI) | p-Value |
|---|---|---|
| Urgent LDLT | 1.23 (0.36–4.18) | 0.744 |
| Recipient age at LDLT | 1.00 (0.97–1.04) | 0.860 |
| Recipient body mass at LDLT | 1.02 (0.86–1.20) | 0.859 |
| GRWR | 1.39 (1.02–1.89) | 0.036 |
| GRWR ≥ 5 | 5.81 (1.77–19-07) | 0.004 |
| PELD/MELD | 1.01 (0.98–1.03) | 0.507 |
| Postoperative bleeding | 1.74 (0.75–4.03) | 0.196 |
| PVT | 1.85 (0.63–5.40) | 0.264 |
| HAT | 1.05 (0.21–5.19) | 0.953 |
| Biliary anastomosis leak | 0.9 (0.25–3.19) | 0.868 |
| Cause of Death | Group A (37) GRWR ≤ 1.5% | Group B (196) >1.5% GRWR ≤ 3.5% | Group C (73) >3.5% GRWR < 5% | Group D (15) GRWR ≥ 5% |
|---|---|---|---|---|
| Infections | 0 | 2 (10.15 days) | 7 (8,30 days, 3,9,13,28,31,70 months) | 2 (22 days, 6 months) |
| MODS | 1 (13 months) | 5 (4.11 * days, 2.2 *,8 months) | 0 | 3 (3.4 days, 51 * months) |
| Malignancy/tumor recurrence | 0 | 4 (30 days, 2,4,17 months) | 1 (5 months) | 0 |
| Acute rejection | 0 | 1 (30 days) | 0 | 0 |
| GVHD | 0 | 1 (3 months) | 0 | 0 |
| HAT | 0 | 1 (6 days) | 0 | 0 |
| Central nervous system complications | 2 (30 days, 36 months) | 2 (4.7 days) | 0 | 0 |
| Gastrointestinal bleeding | 0 | 0 | 0 | 1 (120 months) |
| Allograft dysfunction | 1 (75 months) | 0 | 0 | 0 |
| Autoimmune thrombocytopenia | 0 | 0 | 1 (120 * months) | 0 |
| Non-medical | 0 | 0 | 1 (3 months) | |
| Total (%) | 4 (10.8) | 16 (8.2) | 10 (13.7) | 6 (40.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanowicz, M.; Kowalewski, G.; Szymczak, M.; Patkowski, W.; Zieniewicz, K.; Grzelak, I.; Kowalski, A.; Ismail, H.; Kamińska, D.; Kaliciński, P. Impact of Graft Size Matching on the Early Post-Transplant Complications and Patients Survival in Children after Living Donor Liver Transplantations. Children 2021, 8, 579. https://doi.org/10.3390/children8070579
Stefanowicz M, Kowalewski G, Szymczak M, Patkowski W, Zieniewicz K, Grzelak I, Kowalski A, Ismail H, Kamińska D, Kaliciński P. Impact of Graft Size Matching on the Early Post-Transplant Complications and Patients Survival in Children after Living Donor Liver Transplantations. Children. 2021; 8(7):579. https://doi.org/10.3390/children8070579
Chicago/Turabian StyleStefanowicz, Marek, Grzegorz Kowalewski, Marek Szymczak, Waldemar Patkowski, Krzysztof Zieniewicz, Ireneusz Grzelak, Adam Kowalski, Hor Ismail, Diana Kamińska, and Piotr Kaliciński. 2021. "Impact of Graft Size Matching on the Early Post-Transplant Complications and Patients Survival in Children after Living Donor Liver Transplantations" Children 8, no. 7: 579. https://doi.org/10.3390/children8070579
APA StyleStefanowicz, M., Kowalewski, G., Szymczak, M., Patkowski, W., Zieniewicz, K., Grzelak, I., Kowalski, A., Ismail, H., Kamińska, D., & Kaliciński, P. (2021). Impact of Graft Size Matching on the Early Post-Transplant Complications and Patients Survival in Children after Living Donor Liver Transplantations. Children, 8(7), 579. https://doi.org/10.3390/children8070579