Abstract
Kawasaki disease (KD) is a systemic vasculitis with an unknown etiology affecting young children. Although intravenous immunoglobulin (IVIG) plus acetylsalicylic acid is effective in most cases, approximately 10–20% of patients do not respond to this therapy. An 8-month-old boy was admitted to a local hospital with the presumptive diagnosis of KD. He received IVIG twice and four series of methylprednisolone pulse therapy from the third to the tenth day of illness. Despite these treatments, his fever persisted with the development of moderate dilatations of the coronary arteries. A diagnosis of refractory KD was made, and infliximab with oral prednisolone was administered without success. Defervescence was finally achieved by cyclosporine A, an inhibitor of the signaling pathway of the calcineurin/nuclear factor of activated T cells (NFAT). Whole-genome sequencing of his deoxyribonucleic acid samples disclosed two single nucleotide variants (SNVs) in disease-susceptibility genes in Japanese KD patients, ORAI1 (rs3741596) and BLK (rs2254546). In summary, the refractory nature of the present case could be explained by the presence of combined SNVs in susceptibility genes associated with upregulation of the calcineurin/NFAT signaling pathway. It may provide insights for stratifying KD patients based on the SNVs in their susceptibility genes.
1. Introduction
Kawasaki disease (KD) is a systemic vasculitis affecting young children between 6 months and 4 years old. Although the therapeutic efficacy of intravenous immunoglobulin (IVIG) plus acetylsalicylic acid has been established for KD, approximately 10–20% of patients do not respond to IVIG [1]. As the patients resistant to IVIG have an increased risk of developing coronary artery abnormalities, additional therapeutic strategies such as IVIG retreatment, corticosteroids, or infliximab (IFX, an anti-tumor necrosis factor (TNF)-specific antibody) must be employed.
Recent studies have shown that some refractory KD cases had genetic backgrounds characterized by single nucleotide variants (SNVs) in disease-susceptibility genes [2,3,4].
Here, an infant with refractory KD who did not respond to repeated IVIG, corticosteroids, and IFX, but responded to cyclosporine A (CsA), an inhibitor of the calcineurin/nuclear factor of activated T cells (NFAT) signaling pathway, is presented. Whole-genome sequencing (WGS) revealed that he had combined SNVs in susceptibility genes reported in Japanese KD patients. We also discuss an association of the refractory nature of KD with SNVs.
2. Case Presentation
The patient’s clinical course during admission is shown in Figure 1 and Table 1. An 8-month-old boy presented with a 3-day history of persistent fever, conjunctival infection, changes in the oral mucosa and tongue, skin rash, and redness of the palms and the soles of the feet without identification of the causative infectious agents. A blood investigation showed leukocytosis and an increased level of serum C-reactive protein (CRP). Based on the presumptive diagnosis of KD, he received IVIG (2 g/kg/dose) twice and methylprednisolone pulse therapy (30 mg/kg/day) for four days at a local hospital between the third and the tenth day of illness, without defervescence. He was then transferred to us for further treatment on the tenth day of illness. On admission, the laboratory tests revealed leukocytosis and an elevated CRP level. An echocardiogram revealed moderate dilatations of the left anterior descending artery of the left coronary artery (LAD, Z-score 6.0) and right coronary artery (RCA, Z-score 8.2). The ethics committee approved this study of Kansai Medical University (no. 2019069).
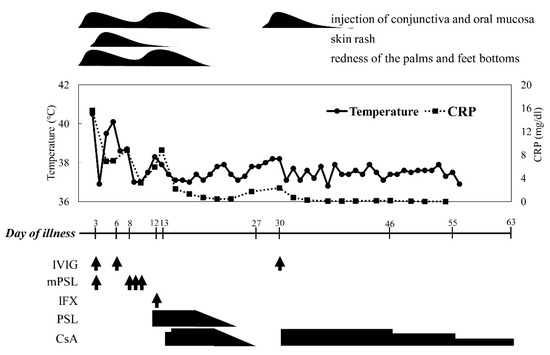
Figure 1.
The clinical course of the present case. Abbreviations and administered dose of the therapeutic agents: CRP, C-reactive protein; IVIG, intravenous immunoglobulin (2 g/kg/day); m-PSL, methylprednisolone (30 mg/kg/day); IFX, infliximab (5 mg/kg/day); PSL, prednisolone (1 mg/kg/day per os); CsA, cyclosporine A (6 mg/kg/day per os with a target trough level between 100–150 ng/mL); arrows indicate the intravenous administrations of therapeutic agents.

Table 1.
Laboratory and Echocardiogram Data in the Clinical Course.
From these findings, a diagnosis of refractory KD complicated by moderate coronary arterial lesions (CALs) was made, and IFX (5 mg/kg) with oral prednisolone (1 mg/kg/day) was administered intravenously on the 12th day of illness without success. Then, according to previous observations of efficacy for refractory KD [5], CsA was initiated orally (6 mg/kg/day) with a target trough level between 100–150 ng/mL from the 13th day of illness. In response to CsA, defervescence was observed on the 14th day of illness, and the dose of CsA was tapered off by two weeks. However, the re-development of fever with increased serum CRP soon after its cessation prompted us to recommence the CsA from the 30th day of illness, which controlled the disease activity well. After that, CsA was gradually tapered off by the 63rd day of illness. He developed CALs at the LAD (Z-score 21.8) and RCA (28.2).
At the outpatient clinic, at 1 year of age, echocardiographic examination demonstrated moderate CALs, necessitating the administration of warfarin, dipyridamole, and aspirin.
The patient’s parents provided informed consent and agreed with the submission of the case report to the journal.
3. Genetic Analysis
To determine the mechanism by which CsA was effective in this patient, WGS was performed to search for SNVs in the susceptibility genes in Japanese KD patients using NovaSeq6000 and the TruSeqDNA PCR-free library (Illumina Inc.; San Diego, CA, USA). The primary data from WGS were automatically processed for assembly and mapping. The obtained whole-genome data were subjected to structural annotation.
First, the susceptibility genes of Japanese KD were listed by a literature search as the following [2,3,4,6]: ORAI1 (calcium release-activated calcium modulator), FCGR2A (Fc fragment of IgG, low-affinity IIa, receptor), BLK (B lymphoid tyrosine kinase), CD40 (CD40), ITPKC (inositol 1,4,5-triphosphate 3-kinase C), CASP3 (caspase-3), and HLA (human leukocyte antigen) (gene products were shown in parentheses). The present case had a total of 17,707 SNVs in these susceptibility genes. Among them, 17,692 SNVs were excluded from further analysis as they were not listed in Table 2, in which the reported SNVs associated with the susceptibility to KD were filled. As a result, 15 SNVs, including 4 SNVs in ORAI1, 4 in CD40, and 7 in BLK, were targeted for the next stage. After leaving out 12 SNVs of synonymous amino acid substitution, 3 SNVs, ORAI1 (rs3741596), CD40 (rs4813003), and BLK (rs2254546), remained as candidate SNVs associated with KD in the case. Among them, the SNV of CD40 was determined to be neutral polymorphism based on the previous reports demonstrating that CD40 (rs4813003) neither promoted nor inhibited the calcineurin/NFAT signaling pathway, preserving the function of CD40L-mediated signaling between B and T cells [7,8].
Table 2.
Studied single-nucleotide variants in the candidate genes in Japanese Kawasaki disease.
Thus, ORAI1 (rs3741596) and BLK (rs2254546) were finally identified as significant SNVs in the case.
4. Discussion
Despite extensive research, the underlying mechanisms of KD remain unknown [1]. The current paradigm on this enigmatic vasculitis pathogenesis is that the disease results from an exaggerated immune response towards infectious agent(s) in a genetically and environmentally susceptible child [9,10]. Genetically determined susceptibility includes polymorphisms in the genes encoding cytokines, chemokines, and enzymes involved in signal transduction. Pathologically, KD is characterized by a marked immune activation associated with endothelial cell injury, which could be due to abnormal cytokine production. The clinical symptoms and laboratory findings also result from abnormally high inflammatory cytokines such as TNF-α, interleukin (IL)-1β, or IL-6 [11,12].
The therapeutic efficacy of IVIG has been established for KD, as IVIG reduces inflammation (fever, clinical signs, acute phase reactant levels) and prevents the development of CAL. IVIG appears to have a generalized anti-inflammatory effect, and possible mechanisms include the enhancement of regulatory T cell activity, the neutralization of bacterial super-antigens or other unknown pathogenic agents, the regulation of cytokine production, the suppression of antibody synthesis and inflammatory markers, the provision of anti-idiotypic antibodies, the Fc-gamma receptor and IL-1β, and balancing the T helper (Th) Th1/Th2 immune responses [13]. However, approximately 10–20% of patients do not respond to IVIG [1,11]. As IVIG-resistant patients have a higher probability for CAL formation [14,15,16], it is important to treat them aggressively. Mounting evidence has identified several epidemiological and laboratory characteristics as predictors of IVIG resistance [13]. These include age [16], illness day, platelet count, erythrocyte sedimentation rate, hemoglobin concentration, CRP [15,16], eosinophils, lactate dehydrogenase, albumin, alanine aminotransferase, concomitant infection [10,15], and granulocyte-colony stimulating factor [14]. Several treatments are available for combination with the second administration of IVIG for patients who do not respond to the initial IVIG treatment, such as IFX, corticosteroids, cytotoxic drugs (cyclophosphamide, methotrexate, CsA), plasmapheresis, and plasma exchange [13].
Though the pathogenesis is poorly understood, recent advances in genome-wide association studies (GWAS) and linkage analyses of KD have identified the SNVs in several disease-susceptibility genes. Candidate genes can be classified into four groups: enhanced T cell activation (ITPKC, ORAI1, STIM1), dysregulated leukocyte signaling (CD40, BLK, FCGR2A), decreased apoptosis (CASP3), and altered transforming growth factor-beta signaling (TGFB2, TGFBR2, MMP, SMAD) [3]. Among them, eight SNVs in seven genes are reported to be representative in Japanese KD patients. These genes (SNVs) are ITPKC (rs28493229), ORAI1 (rs3741596, rs141919534), FCGR2A (rs1801274), CD40 (rs4813003), BLK (rs2254546), CASP3 (rs113420705), and HLA (rs2857151) [2,3,4,6]. Interestingly, most molecules encoded by these genes play important roles in the calcineurin/NFAT signaling pathway (Figure 2). Therefore, it is reasonable to speculate that SNVs in these susceptibility genes could also be related to the refractory nature in the present case via functional changes, with an upregulation of the signaling pathway. SNVs in ITPKC and CASP3 are reported to be associated with resistance to IVIG [17]. Furthermore, recent observations have revealed that one SNV in ORAI1 in a refractory patient caused a gain of function, leading to constitutive Ca2+ entry into immune cells, which upregulated the calcineurin/NFAT signaling pathway [18]. Therefore, the SNV in ORAI1 (rs3741596) detected in the present case might be associated with its refractory nature.
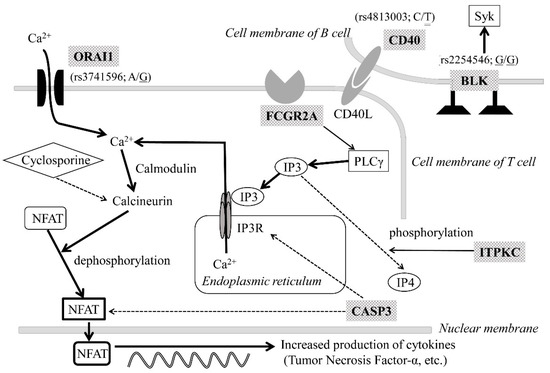
Figure 2.
Susceptibility genes in Kawasaki disease in Japanese patients encoding molecules associated with T-cell activation. The present case had three significant single nucleotide variants (SNVs): ORAI1 (rs3741596), CD40 (rs4813003), or BLK (rs2254546). The types of SNVs, base substitutions, and genotypic patterns of the case are shown in parentheses. The single underline shows an alternative allele with risk for KD, and the double line means a neutral polymorphism. Shaded molecular names are encoded by the representative disease susceptibility genes in Japanese KD patients. Solid lines with arrows indicate activation, while dashed lines with arrows denote the suppression of the calcineurin/NFAT signaling pathway. Abbreviations: BLK, B lymphoid tyrosine kinase; CASP3, caspase-3; FCGR2A, Fc fragment of IgG low-affinity IIa receptor; He, heterozygous genotype; Ho, homozygous genotype; ITPKC, inositol 1, 4, 5-triphosphate 3 kinase C; IP3: inositol 1,4,5-triphosphate; IP3R, inositol 1,4,5-triphosphate receptor; KD: Kawasaki disease, NFAT, nuclear factor of activated T cells; ORAI1, calcium release-activated calcium modulator 1; PLC, phospholipase C; Syk, spleen tyrosine kinase.
Meanwhile, another SNV in BLK (rs2254546) found in the case may also be associated with the activation of the calcineurin/NFAT signaling pathway via cross-interaction between T cells and B cells [19,20]. In this regard, Simpfendorfer et al. revealed that patients with rheumatoid arthritis having SNVs in BLK, including rs2254546, demonstrated a decreased expression of BLK on B cells with reduced B cell receptor signaling activity, leading to the activation of T cells via the CD86 molecule [21]. This report supports the concept that the SNV in BLK detected in the present case (rs2254546) could amplify the upregulation of the calcineurin/NFAT signaling pathway.
Recent observation confirmed the involvement of this pathway in KD, demonstrating that the serum levels of calcineurin and NFAT increased significantly in the acute stage and decreased progressively in the afebrile and subacute stage, reducing the CRP, white blood cell, and neutrophil counts [22]. Furthermore, an in vitro study using cultured endothelial cells of the coronary artery also suggested that the activation of the calcineurin/NFAT signaling pathway plays a vital role in causing the inflammation of the endothelial cells; Wang et al. demonstrated that the serum of KD patients promoted the proliferation of coronary artery endothelial cells not only morphologically but also by increasing the expression of proteins involved in cell proliferation and proteins constituting the calcineurin/NFAT signaling pathway. Furthermore, they reported that the expression of these proteins was suppressed by adding CsA to KD patients’ serum [23]. In other words, the calcineurin/NFAT signaling pathway activated by some extracellular inflammatory molecules is involved in CAL formation, and CsA was shown to be effective in preventing CAL formation in vitro.
From these findings, CsA, a calcineurin inhibitor, is expected to suppress the upregulation of the calcineurin/NFAT signaling pathway in refractory Japanese KD patients. The recent clinical trial from Japan revealed the efficacy of CsA in KD; an open-label, randomized, multicenter study of 173 patients with KD showed that IVIG plus CsA resulted in earlier fever resolution, lower CRP, and a lower CAL formation rate than IVIG alone. There was no difference in adverse events between the two groups, confirming that CsA is helpful in clinical practice for calming inflammation and preventing CAL formation in KD [24].
Based on these findings, the following mechanisms might be involved in the efficacy of CsA in the present case: the calcineurin/NFAT signaling pathway was constitutively upregulated because of an elevated cytosolic Ca2+ concentration due to functional changes in ORAI1 due to SNV in ORAI1 (rs3741596); another SNV in BLK (rs2254546) might indirectly aggravate the calcineurin/NFAT signaling pathway, with an increase in T cell–B cell collaboration; as a result, upregulated calcineurin/NFAT signaling pathway caused an enhanced proinflammatory cytokine production leading to multidrug resistance including IVIG, corticosteroids, and IFX; CsA effectively suppressed the upregulated calcineurin/NFAT signaling pathway resulting in remission, which could not be obtained by other therapeutic agents including repeated IVIG or IFX.
Our present case study has two limitations. First, our concept concerning the relationship between multidrug resistance and the susceptibility genes in KD is based on only a single case. To verify this, further studies with more cases are necessary. Second, the genetic examination was performed using the targeted analysis for the annotation. Thus, several SNVs of other candidate genes have not been considered for their association with KD.
5. Conclusions
The refractory nature of KD patients who did not respond to conventional therapies could be explained by the presence of combined SNVs in susceptibility genes associated with the upregulation of the calcineurin/NFAT signaling pathway. Our findings may provide insights for stratifying KD patients based on the SNVs in their susceptibility genes.
Author Contributions
S.K. and Y.F. prepared the manuscript. S.K., S.-i.H., and K.Y. managed the case. T.O. and K.H. supported and provided advice for the evaluation of the WGS results. K.K. critically reviewed and revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The ethics committee approved this study of Kansai Medical University (no. 2019069).
Informed Consent Statement
A written informed consent as the attached file was obtained from the patients to publish this paper.
Data Availability Statement
It is not applicable in this section.
Acknowledgments
We thank Yoshihiro Onouchi from the Department of Public Health of the Graduate School of Medicine at Chiba University for their expertise in genetics.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 2017, 135, 927–999. [Google Scholar] [CrossRef]
- Onouchi, Y. Genetics of Kawasaki disease: What we know and don’t know. Circ. J. 2012, 76, 1581–1586. [Google Scholar] [CrossRef]
- Kumrah, R.; Vignesh, P.; Rawat, A.; Singh, S. Immunogenetics of Kawasaki disease. Clin. Rev. Allergy Immunol. 2020, 59, 122–139. [Google Scholar] [CrossRef]
- Onouchi, Y.; Fukazawa, R.; Yamamura, K.; Suzuki, H.; Kakimoto, N.; Suenaga, T.; Takeuchi, T.; Hamada, H.; Honda, T.; Yasukawa, K.; et al. Variations in ORAI1 gene associated with Kawasaki disease. PLoS ONE 2016, 11, e0145486. [Google Scholar] [CrossRef]
- Higashigawa, M.; Nakamura, T.; Hattori, T.; Yoshino, A.; Ito, M.; Ichimi, R. Combination of prednisolone and cyclosporin A as third-line therapy for refractory Kawasaki disease: A case study. Minerva Pediatr. 2019. [Google Scholar] [CrossRef]
- Lee, Y.C.; Kuo, H.C.; Chang, J.S.; Chang, L.Y.; Huang, L.M.; Chen, M.R.; Liang, C.D.; Chi, H.; Huang, F.Y.; Lee, M.L.; et al. Two new susceptibility loci for Kawasaki disease identified through genome-wide association analysis. Nat. Genet. 2012, 44, 522–526. [Google Scholar] [CrossRef]
- Lou, J.; Zhong, R.; Shen, N.; Lu, X.Z.; Ke, J.T.; Duan, J.Y.; Qi, Y.Q.; Wang, Y.J.; Zhang, Q.; Wang, W.; et al. Systematic confirmation study of GWAS-identified genetic variants for Kawasaki disease in a Chinese population. Sci. Rep. 2015, 5, 8194. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.R.; Chang, T.Y.; Chiu, N.C.; Chi, H.; Yang, K.D.; Chang, L.; Huang, D.T.N.; Huang, F.Y.; Lien, Y.P.; Lin, W.S.; et al. Validation of genome-wide associated variants for Kawasaki disease in a Taiwanese case-control sample. Sci. Rep. 2020, 10, 11756. [Google Scholar] [CrossRef]
- Kaneko, K.; Akagawa, S.; Akagawa, Y.; Kimata, T.; Tsuji, S. Our evolving understanding of Kawasaki disease pathogenesis: Role of the gut microbiota. Front Immunol. 2020, 11, 1616. [Google Scholar] [CrossRef]
- Dionne, A.; Le, C.K.; Poupart, S.; Autmizguine, J.; Meloche-Dumas, L.; Turgeon, J.; Fournier, A.; Dahdah, N. Profile of resistance to IVIG treatment in patients with Kawasaki disease and concomitant infection. PLoS ONE 2018, 13, e0206001. [Google Scholar] [CrossRef] [PubMed]
- Galeotti, C.; Kaveri, S.V.; Cimaz, R.; Koné-Paut, I.; Bayry, J. Predisposing factors, pathogenesis and therapeutic intervention of Kawasaki disease. Drug Discov. Today 2016, 13, 1850–1857. [Google Scholar] [CrossRef]
- Lee, C.P.; Huang, Y.S.; Hsu, Y.W.; Yang, K.D.; Chien, H.C.; Yu, H.R.; Yang, Y.L.; Wang, C.L.; Chang, W.C.; Kuo, H.C. TARC/CCL17 gene polymorphisms and expression associated with susceptibility and coronary artery aneurysm formation in Kawasaki disease. Pediatr. Res. 2013, 74, 545–551. [Google Scholar] [CrossRef][Green Version]
- Kuo, H.C.; Hsu, Y.W.; Wu, M.S.; Chien, S.C.; Liu, S.F.; Chang, W.C. Intravenous immunoglobulin, pharmacogenomics, and Kawasaki disease. J. Microbiol. Immunol. Infect. 2016, 49, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abe, J.; Ebata, R.; Jibiki, T.; Yasukawa, K.; Saito, H.; Terai, M. Elevated granulocyte colony-stimulating factor levels predict treatment failure in patients with Kawasaki disease. J. Allergy Clin. Immunol. 2008, 122, 1008–1013. [Google Scholar] [CrossRef] [PubMed]
- Downie, M.L.; Manlhiot, C.; Latino, G.A.; Collins, T.H.; Chahal, N.; Yeung, R.S.M.; McCrindle, B.W. Variability in response to intravenous immunoglobulin in the treatment of Kawasaki disease. J. Pediatr. 2016, 179, 124–130. [Google Scholar] [CrossRef]
- Rigante, D.; Valentini, P.; Rizzo, D.; Leo, A.; Rosa, G.D.; Onesimo, R.; Nisco, A.D.; Angelone, D.F.; Compagnone, A.; Delogu, A.B. Responsiveness to intravenous immunoglobulins and occurrence of coronary artery abnormalities in a single-center cohort of Italian patients with Kawasaki syndrome. Rheumatol. Int. 2010, 30, 841–846. [Google Scholar] [CrossRef]
- Kuo, H.C.; Hsu, Y.W.; Wu, C.M.; Chen, S.H.; Hung, K.S.; Chang, W.P.; Yang, K.D.; Hsieh, K.S.; Chen, W.C.; Onouchi, Y.; et al. A replication study for association of ITPKC and CASP3 two-locus analysis in IVIGSimunresponsiveness and coronary artery lesion in Kawasaki disease. PLoS ONE 2013, 8, e69685. [Google Scholar] [CrossRef]
- Thiha, K.; Mashimo, Y.; Suzuki, H.; Hamada, H.; Hata, A.; Hara, T.; Tanaka, T.; Ito, K.; Onouchi, Y. Japan Kawasaki Disease Genome Consortium. Investigation of novel variations of ORAI1 gene and their association with Kawasaki disease. J. Hum. Genet. 2019, 64, 511–519. [Google Scholar] [CrossRef]
- Laird, R.M.; Laky, K.; Hayes, S.M. Unexpected role for the B cell-specific Src family kinase B lymphoid kinase in the development of IL-17-producing γδ T cells. J. Immunol. 2010, 185, 6518–6527. [Google Scholar] [CrossRef]
- Compeer, E.B.; Janssen, W.; van Royen-Kerkhof, A.; van Gijn, M.; van Montfrans, J.M.; Boes, M. Dysfunctional BLK in common variable immunodeficiency perturbs B-cell proliferation and ability to elicit antigen-specific CD4+ T-cell help. Oncotarget 2015, 6, 10759–10771. [Google Scholar] [CrossRef][Green Version]
- Simpfendorfer, K.R.; Armstead, B.E.; Shih, A.; Li, W.; Curran, M.; Manjarrez-Orduño, N.; Lee, A.T.; Diamond, B.; Gregersen, P.K. Autoimmune disease-associated haplotypes of BLK exhibit lowered thresholds for B cell activation and expansion of Ig class-switched B cells. Arthritis Rheumatol. 2015, 67, 2866–2876. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Liu, J.; Geng, Z.; Tao, Y.; Zheng, F.; Wang, Y.; Fu, S.; Wang, W.; Xie, C.; Zhang, Y.; et al. The elevated serum levels of calcineurin and nuclear factor of activated T-cells 1 in children with Kawasaki disease. Pediatr Rheumatol Online J. 2020, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, J.; Liu, J.; Geng, Z.; Tao, Y.; Zheng, F.; Wang, Y.; Fu, S.; Wang, W.; Xie, C.; et al. The role of Ca2+/NFAT in dysfunction and inflammation of human coronary endothelial cells induced by sera from patients with Kawasaki disease. Sci. Rep. 2020, 10, 4706. [Google Scholar] [CrossRef] [PubMed]
- Hamada, H.; Suzuki, H.; Onouchi, Y.; Ebata, R.; Terai, M.; Fuse, S.; Okajima, Y.; Kurotobi, S.; Hirai, K.; Soga, T.; et al. Efficacy of primary treatment with immunoglobulin plus ciclosporin for prevention of coronary artery abnormalities in patients with Kawasaki disease predicted to be at increased risk of non-response to intravenous immunoglobulin (KAICA): A randomised controlled, open-label, blinded-endpoints, phase 3 trial. Lancet 2019, 393, 1128–1137. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).