
The Role of Sleep in the Transition from Acute to Chronic Musculoskeletal Pain in Youth—A Narrative Review

 ,
, 
Abstract
1. Introduction
2. Methods
3. The Transition from Acute to Chronic Pain
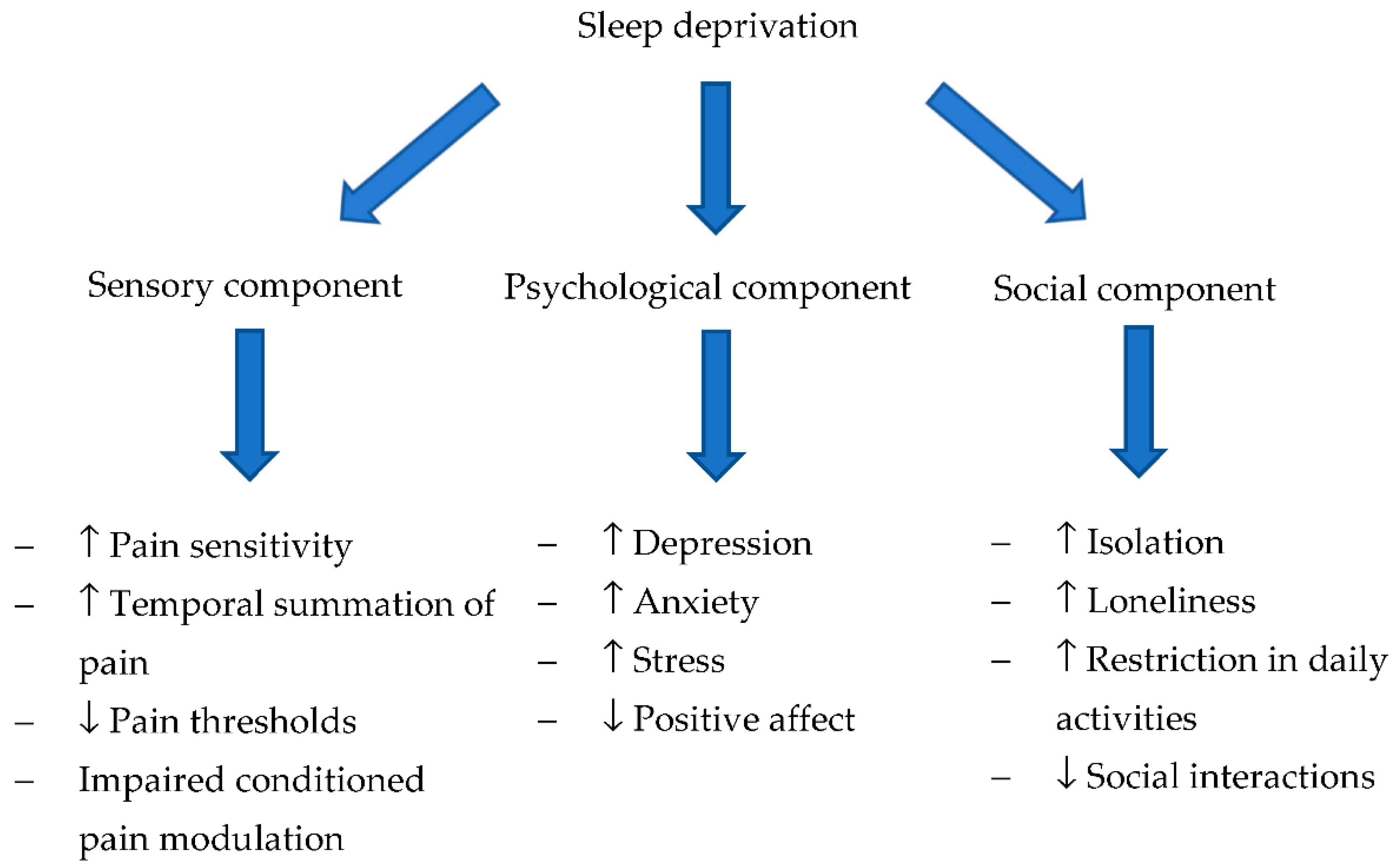
4. The Potential Role of Sleep in the Transition from Acute to Chronic Pain
4.1. Sleep and the Sensory Component of Pain
4.1.1. Evidence on the Effect of Sleep on the Sensory Component of Pain
4.1.2. Mechanisms to Explain the Effect of Sleep on the Sensory Component of Pain
4.2. Sleep and Psychological Factors
4.2.1. Evidence on the Effect of Sleep on the Psychological Component of Pain
4.2.2. Mechanisms to Explain the Effect of Sleep on the Psychological Component of Pain
4.3. Sleep and Social Factors
4.3.1. Evidence on the Effect of Sleep on the Social Component of Pain
4.3.2. Mechanisms to Explain the Effect of Sleep on the Social Component of Pain
5. The Role of Sleep Treatments
5.1. Cognitive-Behavioral Interventions
5.2. Pharmacotherapy
6. Limitations
7. Research Agenda for Future Investigations
- Longitudinal or experimental studies are needed to understand the mediational role of modifiable social and psychological factors on the effect of sleep in the transition from acute to chronic musculoskeletal pain. The evidence for social and psychological factors in children and adolescents is based on only a few cross-sectional studies [53,55] and longitudinal studies [54,56]. Additional longitudinal studies are needed to evaluate the temporal and causal relationships between sleep, social and psychological factors, and subsequent acute to chronic pain transition. This knowledge would allow for a better understanding of the temporal sequence of mechanisms underlying the sleep-pain association, and identify mediators that may be targeted by interventions in order to prevent the development of chronic pain (e.g., reducing social isolation). Investigations of youth following musculoskeletal injury may provide the ideal means to prospectively study these factors over the course of the evolving pain experience.
- Further research is needed to clarify the role of biological factors by means of experimental studies that assess the change in inflammatory mediators (e.g., prostaglandins, cytokines), other substances and neurotransmitters (serotonin, norepinephrine, adenosine, orexin), and HPA axis functioning and their association with pain in children with sleep deficiency. This would allow for a better understanding of the role of biological mechanisms in the transition to chronic pain and their specific intersection with sleep.
- There is also an urgent need for research evaluating whether existing treatments aimed at improving sleep in youth may extend to the context of preventing acute to chronic pain transition. For example, CBT-I has shown efficacy for sleep improvement in multiple pain populations [16], but its role in preventing acute to chronic pain transition remains unexplored.
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; MacDonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef] [PubMed]
- Borsook, D.; Youssef, A.M.; Simons, L.; Elman, I.; Eccleston, C. When pain gets stuck: The evolution of pain chronification and treatment resistance. Pain 2018, 159, 2421–2436. [Google Scholar] [CrossRef] [PubMed]
- Rathleff, M.S.; Holden, S.; Straszek, C.L.; Olesen, J.L.; Jensen, M.B.; Roos, E.M. 5- Year Prognosis and Impact of Adolescent Knee Pain: A Prospective Population-Based Cohort Study in 504 Adolescents. BMJ Open 2019, 9, e024113. [Google Scholar] [CrossRef]
- Nahin, R.L.; Sayer, B.; Stussman, B.J.; Feinberg, T.M. Eighteen-Year Trends in the Prevalence of, and Health Care Use for, Noncancer Pain in the United States: Data from the Medical Expenditure Panel Survey. J. Pain 2019, 20, 796–809. [Google Scholar] [CrossRef] [PubMed]
- Henschke, N.; Kamper, S.J.; Maher, C.G. The Epidemiology and Economic Consequences of Pain. Mayo Clin. Proc. 2015, 90, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Forouzanfar, M.H.; Daoud, F.; Mokdad, A.A.; El Bcheraoui, C.; Moradi-Lakeh, M.; Kyu, H.H.; Barber, R.M.; Wagner, J.; Cercy, K.; et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 2383–2401. [Google Scholar] [CrossRef]
- Rathleff, M.S.; Graven-Nielsen, T. Transition from acute to chronic pain in children: Novel pieces of the puzzle. Pain 2017, 158, 767–768. [Google Scholar] [CrossRef] [PubMed]
- Huguet, A.; Tougas, M.E.; Hayden, J.; McGrath, P.J.; Stinson, J.N.; Chambers, C.T. A Systematic Review with Meta-analysis of Childhood and Adolescent Risk and Prognostic Factors for Musculoskeletal Pain. Pain 2016, 157, 2640–2656. [Google Scholar] [CrossRef]
- Pate, J.W.; Hancock, M.J.; Hush, J.M.; Gray, K.; Pounder, M.; Pacey, V. Prognostic factors for pain and functional disability in children and adolescents with persisting pain: A systematic review and meta-analysis. Eur. J. Pain 2020, 24, 722–741. [Google Scholar] [CrossRef]
- Elman, I.; Borsook, D. Common Brain Mechanisms of Chronic Pain and Addiction. Neuron Perspect. 2016, 89, 11–36. [Google Scholar] [CrossRef]
- Rabbitts, J.A.; Zhou, C.; Narayananf, A.; Palermo, T.M. Longitudinal and temporal associations between daily pain and sleep patterns after major pediatric surgery. Physiol. Behav. 2017, 18, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Maski, K.; Owens, J.A. Insomnia, parasomnias, and narcolepsy in children: Clinical features, diagnosis, and management. Lancet Neurol. 2016, 15, 1170–1181. [Google Scholar] [CrossRef]
- Kansagra, S. Sleep disorders in adolescents. Pediatrics 2020, 145, S204–S209. [Google Scholar] [CrossRef] [PubMed]
- Matricciani, L.; Olds, T.; Petkov, J. In search of lost sleep: Secular trends in the sleep time of school-aged children and adolescents. Sleep Med. Rev. 2012, 16, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.; Noel, M.; Mychasiuk, R. Neurobiological mechanisms underlying the sleep-pain relationship in adolescence: A review. Neurosci. Biobehav. Rev. 2019, 96, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Badawy, S.M.; Law, E.F.; Palermo, T.M. The interrelationship between sleep and chronic pain in adolescents. Curr. Opin. Physiol. 2019, 11, 25–28. [Google Scholar] [CrossRef]
- Valrie, C.R.; Bromberg, M.H.; Palermo, T.; Schanberg, L.E. A systematic review of sleep in pediatric pain populations. J. Dev. Behav. Pediatr. 2013, 34, 120–128. [Google Scholar] [CrossRef]
- Mckillop, H.N.; Banez, G.A. A Broad Consideration of Risk Factors in Pediatric Chronic Pain: Where to Go from Here? Children 2016, 3, 38. [Google Scholar] [CrossRef]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The association of sleep and pain: An update and a path forward. J. Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef]
- Andreucci, A.; Campbell, P.; Mundy, L.K.; Sawyer, S.M.; Kosola, S.; Patton, G.C.; Dunn, K.M. Sleep problems increase the risk of musculoskeletal pain in boys but not girls: A prospective cohort study. Eur. J. Pediatr. 2020, 179, 1711–1719. [Google Scholar] [CrossRef]
- Andreucci, A.; Campbell, P.; Richardson, E.; Chen, Y.; Dunn, K.M. Sleep problems and psychological symptoms as predictors of musculoskeletal conditions in children and adolescents. Eur. J. Pain 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Nassikas, N.J.; Clauw, D.J. The role of the central nervous system in the generation and maintenance of chronic pain in rheumatoid arthritis, osteoarthritis and fibromyalgia. Arthritis Res. Ther. 2011, 13. [Google Scholar] [CrossRef] [PubMed]
- Voscopoulos, C.; Lema, M. When does acute pain become chronic? Br. J. Anaesth. 2010, 105, i69–i85. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.H.S. The role of sleep in pain and fibromyalgia. Nat. Rev. Rheumatol. 2015, 11, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Schrimpf, M.; Liegl, G.; Boeckle, M.; Leitner, A.; Geisler, P.; Pieh, C. The effect of sleep deprivation on pain perception in healthy subjects: A meta-analysis. Sleep Med. 2015, 16, 1313–1320. [Google Scholar] [CrossRef]
- Staffe, A.T.; Bech, M.W.; Clemmensen, S.L.K.; Nielsen, H.T.; Larsen, D.B.; Petersen, K.K. Total sleep deprivation increases pain sensitivity, impairs conditioned pain modulation and facilitates temporal summation of pain in healthy participants. PLoS ONE 2019, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Krietsch, K.N.; King, C.D.; Beebe, D.W. Experimental sleep restriction increases somatic complaints in healthy adolescents. Sleep Med. 2020, 73, 213–216. [Google Scholar] [CrossRef]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Eacret, D.; Veasey, S.C.; Blendy, J.A. Bidirectional relationship between opioids and disrupted sleep: Putative mechanisms. Mol. Pharmacol. 2020, 98, 445–453. [Google Scholar] [CrossRef]
- Boakye, P.A.; Olechowski, C.; Rashiq, S.; Verrier, M.J.; Kerr, B.; Witmans, M.; Baker, G.; Joyce, A.; Dick, B.D. A critical review of neurobiological factors involved in the interactions between chronic pain, depression, and sleep disruption. Clin. J. Pain 2016, 32, 327–336. [Google Scholar] [CrossRef]
- Hannibal, K.E.; Bishop, M.D. Chronic Stress, Cortisol Dysfunction, and Pain: A Psychoneuroendocrine Rationale for Stress Management in Pain Rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Goodin, B.R.; Smith, M.T.; Quinn, N.B.; King, C.D.; McGuire, L. Poor sleep quality and exaggerated salivary cortisol reactivity to the cold pressor task predict greater acute pain severity in a non-clinical sample. Biol. Psychol 2012, 91, 36–41. [Google Scholar] [CrossRef]
- Whibley, D.; Alkandari, N.; Kristensen, K.; Barnish, M.; Rzewuska, M.; Druce, K.L.; Tang, N.K.Y. Sleep and Pain: A Systematic Review of Studies of Mediation. Clin. J. Pain 2019, 35, 544–558. [Google Scholar] [CrossRef] [PubMed]
- Krause, A.J.; Simon, E.B.; Mander, B.A.; Greer, S.M.; Saletin, J.M.; Goldstein-Piekarski, A.N.; Walker, M.P. The sleep-deprived human brain. Nat. Rev. Neurosci. 2017, 18, 404–418. [Google Scholar] [CrossRef] [PubMed]
- Finan, P.H.; Smith, M.T. The Comorbidity of Insomnia, Chronic Pain, and Depression: Dopamine as a Putative Mechanism. Sleep Med. Rev. 2014, 17, 173–183. [Google Scholar] [CrossRef]
- Herrero Babiloni, A.; De Koninck, B.P.; Beetz, G.; De Beaumont, L.; Martel, M.O.; Lavigne, G.J. Sleep and pain: Recent insights, mechanisms, and future directions in the investigation of this relationship. J. Neural Transm. 2020, 127, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Fadda, P.; Tortorella, A.; Fratta, W. Sleep deprivation decreases μ and δ opioid receptor binding in the rat limbic system. Neurosci. Lett. 1991, 129, 315–317. [Google Scholar] [CrossRef]
- Przewłocka, B.; Mogilnicka, E.; Lasón, W.; van Luijtelaar, E.L.J.M.; Coenen, A.M.L. Deprivation of REM sleep in the rat and the opioid peptides β-endorphin and dynorphin. Neurosci. Lett. 1986, 70, 138–142. [Google Scholar] [CrossRef]
- Smith, M.T.; Edwards, R.R.; McCann, U.D.; Haythomthwaite, J.A. The effects of sleep deprivation on pain inhibition and spontaneous pain in women. Sleep 2007, 30, 494–505. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.M.; Bounds, S.C.; Kuwabara, H.; Edwards, R.R.; Campbell, J.N.; Haythornthwaite, J.A.; Smith, M.T. Individual Variation in Sleep Quality and Duration Is Related to Cerebral Mu Opioid Receptor Binding Potential during Tonic Laboratory Pain in Healthy Subjects. Pain Med. 2013, 14, 1882–1892. [Google Scholar] [CrossRef]
- Ukponmwan, O.E.; Rupreht, J.; Dzoljic, M.R. REM sleep deprivation decreases the antinociceptive property of enkephalinase-inhibition, morphine and cold-water-swim. Gen. Pharmacol. 1984, 15, 255–258. [Google Scholar] [CrossRef]
- Nascimento, D.C.; Andersen, M.L.; Hipólide, D.C.; Nobrega, J.N.; Tufik, S. Pain hypersensitivity induced by paradoxical sleep deprivation is not due to altered binding to brain μ-opioid receptors. Behav. Brain Res. 2007, 178, 216–220. [Google Scholar] [CrossRef]
- Raymond, I.; Nielsen, T.A.; Lavigne, G.; Manzini, C.; Choinière, M. Quality of sleep and its daily relationship to pain intensity in hospitalized adult burn patients. Pain 2001, 92, 381–388. [Google Scholar] [CrossRef]
- Raymond, I.; Ancoli-Israel, S.; Choinière, M. Sleep disturbances, pain and analgesia in adults hospitalized for burn injuries. Sleep Med. 2004, 5, 551–559. [Google Scholar] [CrossRef]
- Dimsdale, J.E.; Norman, D.; Dejardin, D.; Wallace, M.S. The Effect of Opioids on Sleep Architecture. J. Clin. Sleep Med. 2007, 3, 33–36. [Google Scholar] [PubMed]
- Shaw, I.R.; Lavigne, G.; Mayer, P.; Choinière, M. Acute Intravenous Administration of Morphine Perturbs Sleep Architecture in Healthy Pain-Free Young Adults: A Preliminary Study. Sleep 2005, 28, 677–682. [Google Scholar] [CrossRef]
- Xiao, L.; Tang, Y.-L.; Smith, A.K.; Xiang, Y.-T.; Sheng, L.-X.; Chi, Y.; Du, W.-J.; Guo, S.; Jiang, Z.-N.; Zhang, G.-F.; et al. Nocturnal sleep architecture disturbances in early methadone treatment patients. Psychiatry Res. 2010, 179, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Burke, C.K.; Peirce, J.M.; Kidorf, M.S.; Neubauer, D.; Punjabi, N.M.; Stoller, K.B.; Hursh, S.; Brooner, R.K. Sleep problems reported by patients entering opioid agonist treatment. J. Subst. Abuse Treat. 2008, 35, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, K.M.; Kurth, M.E.; Anderson, B.J.; Corso, R.P.; Millman, R.P.; Stein, M.D. Assessing Sleep in Opioid Dependence: A Comparison of Subjective Ratings, Sleep Diaries, and Home Polysomnography in Methadone Maintenance. Patients 2011, 113, 245–248. [Google Scholar] [CrossRef]
- Mu, P.; Huang, Y.H. Cholinergic system in sleep regulation of emotion and motivation. Pharmacol. Res. 2019, 143, 113–118. [Google Scholar] [CrossRef]
- Baum, K.T.; Desai, A.; Field, J.; Miller, L.E.; Rausch, J.; Beebe, D.W. Sleep restriction worsens mood and emotion regulation in adolescents. J. Child Psychol. Psychiatry 2014, 55, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.; Palmer, C.A.; Jackson, C.; Farris, S.G.; Alfano, C.A. Impact of sleep restriction versus idealized sleep on emotional experience, reactivity and regulation in healthy adolescents. J. Sleep Res. 2017, 26, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Djilas, V.; Seidman, L.C.; Zeltzer, L.K.; Tsao, J.C.I. Sleep quality, affect, pain and disability in children with chronic pain: Is affect a mediator or moderator? J. Pain 2017, 18, 1087–1095. [Google Scholar] [CrossRef]
- Valrie, C.R.; Gil, K.M.; Redding-Lallinger, R.; Daeschner, C. Brief report: Daily mood as a mediator or moderator of the pain-sleep relationship in children with sickle cell disease. J. Pediatr. Psychol. 2008, 33, 317–322. [Google Scholar] [CrossRef]
- Pavlova, M.; Ference, J.; Hancock, M.; Noel, M. Disentangling the Sleep-Pain Relationship in Pediatric Chronic Pain: The Mediating Role of Internalizing Mental Health Symptoms. Pain Res. Manag. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Bromberg, M.H.; Gil, K.M.; Schanberg, L.E. Daily Sleep Quality and Mood as Predictors of Pain in Children with Juvenile Polyarticular Arthritis. Health Psychol. 2012, 31, 202–209. [Google Scholar] [CrossRef]
- Beattie, L.; Kyle, S.D.; Espie, C.A.; Biello, S.M. Social interactions, emotion and sleep: A systematic review and research agenda. Sleep Med. Rev. 2015, 24, 83–100. [Google Scholar] [CrossRef] [PubMed]
- Tavernier, R.; Willoughby, T. A Longitudinal Examination of the Bidirectional Association Between Sleep Problems and Social Ties at University: The Mediating Role of Emotion Regulation. J. Youth Adolesc. 2015, 44, 317–330. [Google Scholar] [CrossRef]
- Palermo, T.M.; Kiska, R. Subjective sleep disturbances in adolescents with chronic pain: Relationship to daily functioning and quality of life. J. Pain 2005, 6, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Dunster, G.P.; de la Iglesia, L.; Ben-Hamo, M.; Nave, C.; Fleischer, J.G.; Panda, S.; de la Iglesia, H.O. Sleepmore in Seattle: Later school start times are associated with more sleep and better performance in high school students. Sci. Adv. 2018, 4, eaau6200. [Google Scholar] [CrossRef]
- Minges, K.E.; Redeker, N.S. Delayed school start times and adolescent sleep: A systematic review of the experimental evidence. Sleep Med. Rev. 2016, 28, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.L.; Bruni, O. IInsomnia in childhood and adolescence: Clinical aspects, diagnosis, and therapeutic approach. J. Pediatr. 2015, 91, S26–S35. [Google Scholar] [CrossRef] [PubMed]
- Clinch, J.; Eccleston, C. Chronic musculoskeletal pain in children: Assessment and management. Rheumatology 2009, 48, 466–474. [Google Scholar] [CrossRef]
- Forgeron, P.A.; King, S.; Stinson, J.N.; McGrath, P.J.; MacDonald, A.J.; Chambers, C.T. Social functioning and peer relationships in children and adolescents with chronic pain: A systematic review. Pain Res. Manag. 2010, 15, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Åslund, C.; Starrin, B.; Nilsson, K.W. Social capital in relation to depression, musculoskeletal pain, and psychosomatic symptoms: A cross-sectional study of a large population-based cohort of Swedish adolescents. BMC Public Health 2010, 10, 1–10. [Google Scholar] [CrossRef]
- Batley, S.; Aartun, E.; Boyle, E.; Hartvigsen, J.; Stern, P.J.; Hestbæk, L. The association between psychological and social factors and spinal pain in adolescents. Eur. J. Pediatr. 2019, 178, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Fonareva, I.; Janosy, N.R. Sleep Quality and Efficiency in Adolescents with Chronic Pain: Relationship with Activity Limitations and Health Related Quality of Life. Behav. Sleep Med. 2008, 6, 234–250. [Google Scholar] [CrossRef]
- Lewandowski Holley, A.; Wilson, A.C.; Cho, E.; Palermo, T.M. Clinical Phenotyping of Youth With New-Onset Musculoskeletal Pain. Clin. J. Pain 2017, 33, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Harrison, L.; Wilson, S.; Munafò, M.R. Pain-related and Psychological Symptoms in Adolescents With Musculoskeletal and Sleep Problems. Clin. J. Pain 2016, 32, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Keefe, F.J.; Rumble, M.E.; Scipio, C.D.; Giordano, L.A.; Perri, L.M. Psychological aspects of persistent pain: Current state of the science. J. Pain 2004, 5, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Felt, B.T.; Chervin, R.D. Medications for sleep disturbances in children. Neurol. Clin. Pract. 2014, 4, 82–87. [Google Scholar] [CrossRef]
- de Zambotti, M.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Insomnia disorder in adolescence: Diagnosis, impact, and treatment. Sleep Med. Rev. 2018, 39, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Blake, M.J.; Sheeber, L.B.; Youssef, G.J.; Raniti, M.B.; Allen, N.B. Systematic Review and Meta-analysis of Adolescent Cognitive–Behavioral Sleep Interventions. Clin. Child Fam. Psychol. Rev. 2017, 20, 227–249. [Google Scholar] [CrossRef]
- Palermo, T.M.; Beals-Erickson, S.; Bromberg, M.; Law, E.; Chen, M. A single arm pilot trial of brief cognitive behavioral therapy for insomnia in adolescents with physical and psychiatric comorbidities. J. Clin. Sleep Med. 2017, 13, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Law, E.F.; Wan Tham, S.; Aaron, R.V.; Dudeney, J.; Palermo, T.M. Hybrid Cognitive-Behavioral Therapy Intervention for Adolescents With Co-Occurring Migraine and Insomnia: A Single-Arm Pilot Trial. Headache 2018, 58, 1060–1073. [Google Scholar] [CrossRef]
- Tang, N.K.Y. Cognitive behavioural therapy in pain and psychological disorders: Towards a hybrid future. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 87, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J.; Buysse, D.J.; Krystal, A.D.; Neubauer, D.N.; Heald, J.L. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 307–349. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Proposed Mechanism | Relationship with Sleep | Relationship with Pain |
|---|---|---|
| ↑ Inflammatory mediators (prostaglandins, cytokines) | ↑ Prostaglandins, cytokines after SD | ↑ Prostaglandins, cytokines in pain conditions |
| Altered serotonergic system | ↑ Serotonin (acute SD) ↓ Serotonin 1A receptor sensitivity (chronic SD) | Impaired serotonergic descending inhibitory system ↓ Pain threshold |
| ↑ Norepinephrine | ↑ Norepinephrine after SD | Not clear yet |
| ↑ Adenosine | ↑ Adenosine after SD | ↑ Adenosine associated with hyperalgesia |
| ↑ Activity orexinergic system | ↑ Activity orexinergic system after SD | Pain modulation |
| HPA axis | ↑ HPA axis reactivity after SD | ↑ HPA axis reactivity in chronic pain |
| Dopaminergic signaling | ↓ Dopamine after SD | ↓ Dopamine in chronic pain |
| Opioidergic system | ↓ Endogenous opioids after SD ↓ µ and δ opioid receptors | Impaired opioidergic descending inhibitory system |
| Proposed Mechanism | Relationship with Sleep | Relationship with Pain |
|---|---|---|
| Emotional component of pain | Negative mood after SD affects the emotional component of pain | ↓ Pain threshold due to high negative mood |
| Coping strategies | Maladaptive coping after SD | ↑ Pain perception due to maladaptive coping strategies |
| Engagement in daily activities | ↓ Engagement in daily activities after SD | ↓ Engagement in daily activities linked to pain |
| Catastrophizing | ↑ Catastrophizing after SD | ↑ Focus on pain due to catastrophizing |
| Reward | ↑ Motivation after acute SD ↑ or ↓ motivation after chronic SD | Dysfunctional reward associated with chronic pain |
| 5-HT neuromodulators | ↓ 5-HT both in depression and after SD | ↓ 5-HT in chronic pain |
| Dopaminergic signaling | ↓ Dopamine both in depression and after SD | ↓ Dopamine in chronic pain |
| Amygdala | ↑ Amygdala activity in negative emotional states and after SD ↓ Amygdala activity in positive emotional states | ↑ Amygdala activity - increased pain ↓ Amygdala activity - decreased pain |
| Proposed Mechanism | Relationship with Sleep | Relationship with Pain |
|---|---|---|
| Maladaptive coping | Maladaptive coping after SD in socially isolated children | ↑ Pain perception |
| ↓ Engagement in daily activities | ↓ Engagement in daily activities after SD and social isolation | ↑ Disability and chronic pain |
| Fatigue | ↑ Fatigue after SD | ↑ Disability and chronic pain |
| Fear-avoidant behaviors | ↑ Fear-avoidant behaviors after SD | ↑ Disability and chronic pain |
| Amygdala | ↑ Amygdala activity after SD in socially isolated children | ↑ Attention to pain due to: ↑ emotional sensitivity ↓ regulatory control |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreucci, A.; Groenewald, C.B.; Rathleff, M.S.; Palermo, T.M. The Role of Sleep in the Transition from Acute to Chronic Musculoskeletal Pain in Youth—A Narrative Review. Children 2021, 8, 241. https://doi.org/10.3390/children8030241
Andreucci A, Groenewald CB, Rathleff MS, Palermo TM. The Role of Sleep in the Transition from Acute to Chronic Musculoskeletal Pain in Youth—A Narrative Review. Children. 2021; 8(3):241. https://doi.org/10.3390/children8030241
Chicago/Turabian StyleAndreucci, Alessandro, Cornelius B. Groenewald, Michael Skovdal Rathleff, and Tonya M. Palermo. 2021. "The Role of Sleep in the Transition from Acute to Chronic Musculoskeletal Pain in Youth—A Narrative Review" Children 8, no. 3: 241. https://doi.org/10.3390/children8030241
APA StyleAndreucci, A., Groenewald, C. B., Rathleff, M. S., & Palermo, T. M. (2021). The Role of Sleep in the Transition from Acute to Chronic Musculoskeletal Pain in Youth—A Narrative Review. Children, 8(3), 241. https://doi.org/10.3390/children8030241