Abstract
Background: The COVID-19 pandemic is a global issue which affects the entire population’s mental health. This study evaluates how restrictions to curtail this pandemic change parenting self-efficacy, depressive symptoms, couple satisfaction and health-related quality of life in parents after delivery of a newborn. Methods: In this prospective single center evaluation of parental self-efficacy and quality of life, four validated questionnaires were used to repeatedly assess parenting self-efficacy (Tool to measure Parental Self-Efficacy, TOPSE), depressive symptoms (Edinburgh Postnatal Depression Scale, EPDS), couple satisfaction (Couple Satisfaction Index, CSI) and health-related quality of life (short form 12, SF12). Fifty-three parents of 50 infants answered a total number of 63 questionnaires during the lockdown period to limit the spread of COVID-19. These questionnaires were matched with 63 questionnaires of 58 other parents that had answered them before or after strong pandemic related measures. Results: Parents experienced lower parenting self-efficacy during the strict pandemic measures as compared to before and after (p = 0.04). In terms of age, socioeconomic, marital status and duration of hospitalization we detected no significant difference between both groups. On univariate linear regression, TOPSE scores were associated with gestational age (p = 0.044, parameter estimate: 1.67, 95% CI: 0.048 to 3.301), birth weight (p = 0.035, parameter estimate: 0.008, 95% CI: 0.001 to 0.015), number of newborns’ siblings (p = 0.0554, parameter estimate: 7.49, 95% CI: −0.174 to 15.145) and distance of home from hospital (p = 0.043, parameter estimate: −0.38, 95% CI: −0.745 to −0.011). Interestingly, there was a positive correlation between quality of life and TOPSE scores, suggesting that those who experience a higher self-efficacy also have a higher quality of life. Conclusions: When implementing a lock-down period psychological effects such as lower experience of parental self-efficacy have to be considered.
1. Introduction
The COVID-19 pandemic due to infection with SARS-CoV-2, a coronavirus first described in 2019, affects the world in many different ways. On March 11th 2020 the World Health Organization declared the state of a global pandemic [1]. In Switzerland, the government reacted and took pandemic measures starting from March 17th on by advising people to stay at home, recommending home-office and calling up military service in case of need for more employees in the health system [2]. Correspondingly, since 12 March, no visitors were allowed during the hospital stay at the University Hospital Zurich with the exception that fathers were tolerated in the delivery room during the immediate delivery of their child [3]. We named these social restrictions “pandemic lockdown period”. From 27 March on, some COVID-19 measures were eased [4] and the visiting ban at the University Hospital of Zurich was lifted on 30 May (according to internal communication, USZ). Recent studies showed that the pandemic and the associated social measures had an impact on mental health in the entire population [5,6,7]. It is known from previous pandemics, such as SARS-CoV-1 in 2003, that the population suffers from psychological distress afterwards [8]. In earlier pandemics new parents experienced symptoms of depression and anxiety, as well as stress, due to lots of uncertainties involving perinatal care of their child [9]. Self-efficacy describes the people’s belief in their own abilities to complete a given task [10]. Studies suggest that a higher self-efficacy may correlate with a better task performance [11,12] and lower psychological distress [13]. However, family well-being is influenced by many factors, some external such as social disruption by COVID-19 measures but also altered couple relationships changed due to home-office and home-schooling. Data show that in previous pandemics the couple relationships in families can also improve in some cases as both partners were able to support each other [9,14,15]. A recent study from China has already shown that parents of children hospitalized due to the pandemic had more serious mental health problems than parents of children hospitalized due to medical issues unassociated with the pandemic [16]. In this study, we aim to determine the effect of COVID-19 measures on parents’ self-efficacy, depressive symptoms, couple satisfaction and quality of life.
2. Materials and Methods
2.1. Study Subjects
During the recruiting period starting in December 2018, parents of term and preterm born newborn infants delivered at the University Hospital Zurich were approached at the maternity ward and neonatology unit. Parents who were able to complete the questionnaire in German or English and willing to participate, were included in the study. Exclusion criteria were parents of children with genetic abnormalities or severe morbidities detected before or after birth (such as congenital heart disease, trisomy 21, 18 and 13).
2.2. Procedure
This research project is part of an ongoing single-center prospective study evaluating parental self-efficacy, quality of life, postpartum depressive symptoms and couple relationship in parents of newborn infants at the University Hospital of Zurich since December 2018. During the COVID-19 pandemic the project was allowed to be continued in a restricted way. Consequently, parents were invited to participate, but only if the contact between the physician and parents was needed for clinical reasons. Whenever possible, mother and father were recruited, but it was also possible that one parent participated separately. The analysis took place after the measures that were taken due to COVID-19 pandemic were eased. In this study, we distinguished between strong pandemic measures from 17 March 2020 to 30 May 2020 (lockdown period), characterized by governmental recommendation to stay at home, to work from home, to keep social distancing, and, specific visiting ban at University Hospital of Zurich), and the time before the measures were put in place or after those measures were eased. During the lockdown period 53 parents (43 mothers and 10 fathers) completed 63 questionnaires. These questionnaires were statistically matched by survey point and gestational age of the infant with 63 questionnaires of 58 parents (40 mothers and 18 fathers) that had participated in the study before or after the pandemic measures according to the consort diagram (Figure 1). Mothers and fathers responded to the questionnaires independently and repeatedly at three measuring times: 1) during the first week postpartum, 2) after six weeks postpartum and 3) after three months postpartum. If the baby was born preterm, parents filled in the questionnaire 1) in the first week postpartum, 2) at term equivalent 3) three months postpartum. Some infants were treated in the maternity ward and some were hospitalized at a neonatology unit.
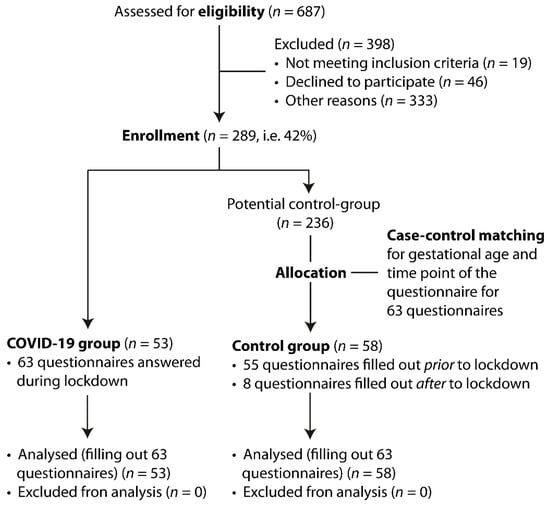
Figure 1.
CONSORT diagram for enrollment and study allocation.
2.3. Questionnaire
The entire questionnaire consisted of the tool to measure parenting self-efficacy (TOPSE score), the Edinburgh Postnatal Depression Scale (EPDS), the Couple Satisfaction Index (CSI) and the Short Form 12 (SF-12).
TOPSE is a validated tool to assess parenting self-efficacy [17]. Parents are asked to rate the extent to which they agree to a total of 30 statements regarding parenting self-efficacy on a scale from one to ten. It covers different topics of parenting including both emotions, affection and pressures they feel as a parent as well as self-acceptance and confidence. Parenting self-efficacy is defined as the parents’ own perception about their ability to successfully care for their newborn child. A higher score indicates a better parenting self-efficacy.
The EPDS is a screening tool for symptoms of depression and anxiety. The questionnaire is composed of ten questions about feelings parents experience postpartum. The answers are scored with 0 to 3 points and summed together for the score values. Higher scores indicate higher depressive symptomatology [18]. Although it was originally created to screen for depressive symptoms in mothers, the EPDS has also been validated for fathers [19].
The CSI consists of four questions which evaluate relationship satisfaction in couples [20]. Each question has six answer choices, which are rated with 0 to 5 points and summed together. Higher scores indicate more couple satisfaction.
The SF-12 is a questionnaire validated to measure health-related quality of life [21]. It consists of twelve questions divided in eight dimensions: physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role and mental health. For each dimension a score from 0–100 points is calculated. SF-12 total score is the mean value of the eight dimensions. Sub-scores for physical and mental health can be analyzed separately. A higher SF-12 score indicates a better health-related quality of life. CSI, SF-12 and TOPSE questionnaires were not specifically validated for women only and can be applied for both women and men [17,21,22].
2.4. Primary and Secondary Outcomes
The primary endpoint was the investigation for parental self-efficacy (TOPSE score) and the influence of the lockdown period. Secondary outcomes were the investigation for health-related quality of life (total scores of SF-12), the evaluation of EPDS and of the CSI questionnaires and investigation of variables that might have an impact on parental self-efficacy (TOPSE score) such as gestational age, birth weight, gender, proxy filling in the questionnaire (mother vs. father), family socioeconomic status, age and health status of parents, parental self-estimation of quality of life, number of the newborns’ siblings and distance from hospital to home.
2.5. Statistics
The questionnaires completed during the lockdown period were statistically matched to controls before or after the lockdown period by survey times (1 week after birth, 6 weeks after birth (at term for preterm birth), and 3 months after birth) and by gestational age of the participants’ infants. The data were processed and analyzed using GraphPad Prism version 8.0 (GraphPad Software, San Diego, California USA), SAS, version 9.3 (SAS Institute, Cary, NC, USA), and scistat (MedCalc Software Ltd., Ostend, Belgium) and JASP (JASP Team, v. 0.11.1). Visualization of the results was performed with R (version 4.0.2). The data was tested for normal distribution. All statistical tests were two-sided. p values < 0.05 were considered statistically significant for all analyses. Wilcoxon rank sum test (Mann Whitney U test) was used to analyze the influence of strong pandemic measures on univariate analysis. Additionally, a linear multivariable regression model with the TOPSE Score as outcome variable and strong pandemic measures as principal exposure variable was carried out, including variables with a significance on univariate analysis at ≤0.02 or clinical importance.
2.6. Ethics
The responsible local ethics committee approved the research plan on 29.11.2018 (Nr: 2018-01796). Participating parents signed an Informed Consent.
3. Results
3.1. Characteristics of the Study Population
From December 2018 until June 2020, 289 parents of 160 term and 66 preterm children were included in the research project. The response rate was 42%. 63 questionnaires, completed by 53 participants during the lockdown period were statistically matched with 63 questionnaires, completed by 58 participants prior or post the lockdown period (55 questionnaires filled in prior and eight questionnaires filled in after the lockdown period). 36 parents answered one questionnaire during the lockdown period, 10 parents answered two questionnaires during the lock-down period and seven parents answered questionnaires both during and before or after the lockdown period. We had 11 couples participating which means mother and father answered the questionnaires separately. Eight of these couples participated during lockdown period, one couple before lockdown period and of two couples mother and father answered the questionnaire with a time difference of a few days, which caused them to be in both periods (before/after and during lockdown period). Altogether, 64 questionnaires were evaluated for the first point of time of the survey (1 week after birth), 42 questionnaires for the second point of time (at predicted term or 6 weeks after birth) and 20 questionnaires at the third point of time (3 months after birth). During the time before the strong pandemic measures three parents answered more than one questionnaire, during “lockdown” measures ten answered two questionnaires. The characteristics of the study population are shown in Table 1. Timeline of filling in the questionnaires is depicted in Figure 2.

Table 1.
Baseline characteristics of 104 parents and 103 children.
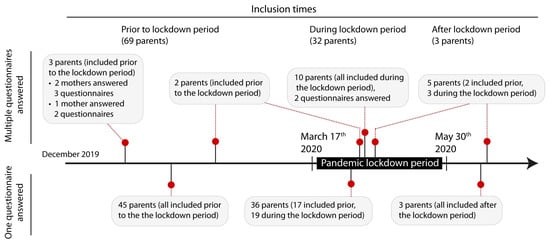
Figure 2.
The lockdown period interfered unexpectedly with the study evaluation of parental self-efficacy, that is why the questionnaires filled in during the lockdown period were statistically matched with questionnaires of parents with children of the same gestational age and the same time after delivery.
3.2. Primary Outcome During COVID-19 Lockdown Period
On univariate analysis, when comparing the questionnaires completed during the strong COVID-19 pandemic measures to those completed before or after the lockdown situation, parenting self-efficacy (TOPSE score) was significantly lower (p = 0.041, effect size: 0.215) (shown in Table 2 and Figure 3. When performing a subanalysis of the matched data, excluding questionnaires of the seven parents that answered prior/after and during lockdown period and their matched questionnaires, TOPSE is also significantly lower (p = 0.008, 95% CI: −0.752 to 0.058, effect size: −0.347). When performing the same subanalysis on the matched data excluding questionnaire of the eleven fathers of the participating couples and their matched questionnaires, TOPSE is still significantly lower (p = 0.048, effect size −0.309). A combined subanalysis without individuals filling out several questionnaires in both groups and excluding fathers when couples filled out questionnaires and all of their matching questionnaires, TOPSE during lockdown period is significantly lower (p = 0.011, effect size: −0.479). Overall matched questionnaires when comparing all TOPSE scores of mothers and fathers in a univariate analysis there was no significant difference found (p = 0.183, effect size: 0.262).
Table 2.
Characteristics of standardized evaluation of tendency to depression (EPDS), couple satisfaction (CSI), quality of life (SF-12) and self-efficacy (TOPSE). A p-value of <0.05 is considered significant meaning that parental self-efficacy has been reduced during the lockdown period (marked in bold). Values given as mean (95% CI).
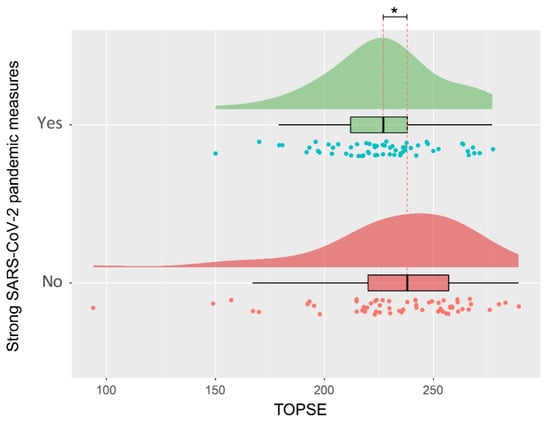
Figure 3.
Visualization of the distribution of parental self-efficacy during the lock-down period or before and after. * Significant difference p < 0.05.
3.3. Secondary Outcomes during COVID-19 Lockdown Period
EPDS, CSI as well as SF-12 total and subscores did not show any difference in the two groups before or after and during the COVID-19 pandemic lockdown situation (Table 2). No significant differences between questionnaires filled in by mothers compared to fathers were observed.
Predictors of parenting self-efficacy (TOPSE score) were analyzed using linear regression analysis. On simple linear regression, a significant association between TOPSE score and gestational age (p = 0.044, parameter estimate: 1.67, 95% CI: 0.048 to 3.301), birth weight (p = 0.035, coefficient: 0.008, 95% CI: 0.001 to 0.015), number of newborns’ siblings (p = 0.055, parameter estimate: 7.49, 95% CI: −0.174 to 15.145) and distance of home from hospital (p = 0.043, parameter estimate: −0.38, 95% CI: −0.745 to −0.011) was found. The linear multivariable regression analysis with TOPSE scores as outcome variable and strong pandemic measure (lockdown period) as principal exposure variable, adjusted for gestational age, birth weight, gender and including clinical relevant variables and/or significance at ≤ 0.2 results in univariate analysis (parental filling in the questionnaire (mother vs. father), age of parent at time of filling in the questionnaire, presence of physical or psychological parental problems, number of siblings, parental self-estimation of quality of life and socioeconomic status) was performed. The lockdown period was negatively associated with TOPSE scores, indicating that parents reported lower self-efficacy during strong pandemic measures (p = 0.0497, parameter estimate: −11.5, 95% CI: −23.04 to −0.014). Assessing the raw data, we found one significant outlier with a TOPSE score below 100 in the group of parents filling in the questionnaire before the lockdown period. Statistically, due to the difference of more than 2 standard-deviations to the mean, it might be appropriate to exclude this value which then would result in even more significant results with a significant reduction of TOPSE during the lockdown period (p = 0.013). In order to not overestimate the effects, we cautiously kept the value within the dataset. Parental self-assessment of quality of life was positively associated with higher TOPSE scores (p = 0.0297, parameter estimate: 4.549, 95% CI: 0.457 to 8.641).
4. Discussion
The objective of this research was to evaluate the influence of the lockdown period on parental self-efficacy after delivery of a child at the University Hospital Zurich. It became clear that parents who cared for an infant younger than 3 months during the lockdown period because of the COVID-19 pandemic exhibited less parenting self-efficacy compared to those parents, who were in the same situation before or after pandemic measures. This result was shown to be robust, no matter whether we kept or excluded serial questionnaires or both questionnaires filled out separately by fathers or mothers belonging to the same couple and child/children. On a professional level, increased self-efficacy is correlated with a higher level of job-satisfaction and job-performance, especially concerning tasks of a lower complexity [23]. Increasing evidence suggests that parental self-efficacy may also improve parental competences as reviewed by Jones [24]. These findings are in line with the study of Leahy-Warren and Mc Carthy who found that maternal self-efficacy decreases with stress, anxiety and depression while it increases with social support and parenting satisfaction [25]. To our opinion, the lockdown period was a completely new situation with new uncertainties for parents and the caring personnel which made personnel interaction and social support more difficult. These facts may have contributed to the reduction of self-effectiveness. Additional studies suggest that pandemic measures may be associated with increased levels of depression and anxiety [26] and may even correlate with long-term psychological consequences such as posttraumatic stress disorder [27,28]. In Switzerland the “Swiss Corona Stress Study” demonstrates that about 40% of responders felt more stressed during the pandemic compared to the time before [29] and in Italy, anxiety, perceived stress and adjustment disorder affected about every 5th person who filled in the questionnaire during the Italian lockdown period [30]. Interventions which strengthen parental self-efficacy such as family centered or family integrated care [31,32] should therefore be promoted during times of insecurity such as a pandemic. Interestingly, our secondary analysis demonstrated a positive correlation between self-assessment of quality of life and TOPSE scores, suggesting that those with higher self-efficacy also experience a better quality of life. According to Banduras theory main sources of self-efficacy are the observation of role models, the opportunity to practice, receiving feedback and the affective state [33]. During the lockdown period the social contacts have been reduced, which may have led to a reduction of potential role models, a reduction of opportunities to practice with respective feedbacks of peers and/or personnel. Interestingly, parents with preterm children and those with children at a lower birth weight also showed a reduced self-efficacy compared to parents with term children of higher weight. This result may be partially due to the reduced emotional feedback of preterm children and possibly increased concerns and uncertainty due to prematurity and reduced weight [34].
However, in contrast to previous studies in this study population of new parents’ the self-reported quality of life as well as symptoms of depression and anxiety did not differ due to pandemic measures [5,6,16,35]. It may be that the low self-efficacy we detected using the TOPSE score may later on predispose for depression or adjustment problems as suggested by the cognitive vulnerability hypothesis [36,37]. Perhaps the assessment time in our setting was too early to detect these problems. The fact that fathers were allowed to stay in the hospital for deliveries only and could not visit their child and partner afterwards could be one reason for lower self-efficacy of both fathers and mothers in our study. In their responses, mothers reported about uncertainties before delivery being frightened how the delivery would take place and if their partner could arrive on time. Also, the psychological well-being of the health care team might have been affected by the COVID-19 measures because of a different interaction with their patients [38,39,40,41]. The design of the study restricts the cases to the time of the “lockdown period”, not taking into account that a certain fear and anxiety concerning the spreading pandemic may both already occur before the implementation of strong measures and may persist after lockdown release. In Zurich, unlike in other cities, there has not been a relevant pandemic related shortage of medical resources, and the medical support after delivery by both nurses and midwifes has always been available. Studies describing the association of depression following quarantine mainly involve people who were advised to completely stay at home [42] and were assessed years later [43], while in Zurich it was still allowed to go outside and meet in groups ≤ 5 persons. Additionally, it is possible that some parents could enjoy more family time at home due to parental working in home office which may have helped to prevent mental health issues. Another possible reason could be that pandemic measures in Switzerland were not as strict as compared to China or Denmark. The Danish study of Sønderskov et al. found that the general population was negatively affected by the pandemic, with women being more affected than men [6]. However, our study could not confirm this difference in our population investigated. Parenting self-efficacy is important because it affects children’s upbringing [44,45].
This study has several limitations. It was not assessed how much time fathers could spend with their family after the delivery of the newborn. In Switzerland, fathers officially get one day off at work after the birth of their child, but some companies offer more days of paternity leave or some fathers take their holidays to be with their family. The control group consists of individuals filling in the questionnaire before OR after the lockdown period and some individuals filled in a questionnaire at several times, couples participating, resulting in a heterogenous group with overlaps, which could influence the results. However, to control for this potential bias, we matched the questionnaires with controls by survey point and gestational age. Subanalyses showed that couples or individuals filling out questionnaires at several times did not influence the significant result for lower TOPSE scores during lockdown period. Furthermore, we controlled the potential bias factors by performing the regression analysis on the matched data, including the same parameters to double check for any influence on the primary outcome TOPSE Score.
5. Conclusions
This study demonstrates a significant lower parental self-efficacy during the phase when the COVID-19 pandemic measures in Switzerland were active, compared to the situation before or after. Health care teams should consider intervention programs to support parenting self-efficacy, especially during situations of global uncertainty.
Author Contributions
A.X. and T.R. conceptualized and designed the study, collected and analyzed data and drafted the initial manuscript; V.O. collected data and helped to write the manuscript; P.L.M.-G. helped to design the study and revised the manuscript; F.S. performed statistical analysis, revised the manuscript and drafted the statistical figures. F.R.-G. performed statistical analysis and revised the manuscript; G.N., T.K. and D.B. gave input to the conceptualization, helped to acquire funding and revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This project was funded by the Hartmann Müller Foundation ID2343.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Zurich 29.11.2018 (protocol code: 2018-01796 and date of approval: 29.11.2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We thank all the parents and the clinical team at the Department of Neonatology for their valuable contributions. We thank Barbara Dinten-Schmid for her advice during the conceptualization period. We thank Felicia Gray for medical writing support.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
References
- Virtual Press Conference on COVID-19—11 March 2020 [Press Release]. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-emergencies-coronavirus-press-conference-full-and-final-11mar2020.pdf?sfvrsn=cb432bb3_2 (accessed on 11 March 2020).
- Admin.ch. Coronavirus: Bundesrat erklärt die “ausserordentliche Lage” und verschärft die Massnahmen 2020. Available online: https://www.admin.ch/gov/de/start/dokumentation/medienmitteilungen.msg-id-78454.html (accessed on 17 March 2020).
- Zürich, U. USZ erlässt Zutrittsverbot für Besucherinnen und Besucher 2020. Available online: http://www.usz.ch/news/medienmitteilungen/Seiten/Zutrittsverbot.aspx (accessed on 12 March 2020).
- Admin.ch. Bundesrat lockert schrittweise Massnahmen zum Schutz vor dem neuen Coronavirus 2020. Available online: https://www.admin.ch/gov/de/start/dokumentation/medienmitteilungen/bundesrat.msg-id-78818.html (accessed on 27 April 2020).
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Sønderskov, K.M.; Dinesen, P.T.; Santini, Z.I.; Østergaard, S.D. The depressive state of Denmark during the COVID-19 pandemic. Acta Neuropsychiatr. 2020, 32, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Peng, E.Y.; Lee, M.B.; Tsai, S.T.; Yang, C.C.; Morisky, D.E.; Tsai, L.T.; Weng, Y.L.; Lyu, S.Y. Population-based post-crisis psychological distress: An example from the SARS outbreak in Taiwan. J. Formos. Med. Assoc. 2010, 109, 524–532. [Google Scholar] [CrossRef]
- Farewell, C.V.; Jewell, J.; Walls, J.; Leiferman, J.A. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience during COVID-19. J. Prim. Care Community Health 2020, 11, 2150132720944074. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. The assessment and predictive generality of self-percepts of efficacy. J. Behav. Ther. Exp. Psychiatry 1982, 13, 195–199. [Google Scholar] [CrossRef]
- Ouweneel, E.; Schaufeli, W.B.; Le Blanc, P.M. Believe, and you will achieve: Changes over time in self-efficacy, engagement, and performance. Appl. Psychol. Health Well Being 2013, 5, 225–247. [Google Scholar] [CrossRef]
- Howard, M.C. Task performance influences general self-efficacy, even without increases in the skills required to achieve success. J. Soc. Psychol. 2019, 159, 642–647. [Google Scholar] [CrossRef]
- Morelli, M.; Cattelino, E.; Baiocco, R.; Trumello, C.; Babore, A.; Candelori, C.; Chirumbolo, A. Parents and Children During the COVID-19 Lockdown: The Influence of Parenting Distress and Parenting Self-Efficacy on Children’s Emotional Well-Being. Front. Psychol. 2020, 11, 584645. [Google Scholar] [CrossRef]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef]
- Günther-Bel, C.; Anna, V.; Eduard, C.; Sonia, T.-G.; Carles, P.-T. A Mixed-method Study of Individual, Couple, and Parental Functioning During the State-regulated COVID-19 Lockdown in Spain. Fam Process. 2020, 59, 1060–1079. [Google Scholar] [CrossRef] [PubMed]
- Yuan, R.; Xu, Q.H.; Xia, C.C.; Lou, C.Y.; Xie, Z.; Ge, Q.M.; Shao, Y. Psychological status of parents of hospitalized children during the COVID-19 epidemic in China. Psychiatry Res. 2020, 288, 112953. [Google Scholar] [CrossRef]
- Kendall, S.; Bloomfield, L. Developing and validating a tool to measure parenting self-efficacy. J. Adv. Nurs. 2005, 51, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Matthey, S.; Barnett, B.; Kavanagh, D.J.; Howie, P. Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. J. Affect. Disord. 2001, 64, 175–184. [Google Scholar] [CrossRef]
- Funk, J.L.; Rogge, R.D. Testing the ruler with item response theory: Increasing precision of measurement for relationship satisfaction with the Couples Satisfaction Index. J. Fam. Psychol. 2007, 21, 572–583. [Google Scholar] [CrossRef]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Galenkamp, H.; Stronks, K.; Mokkink, L.B.; Derks, E.M. Measurement invariance of the SF-12 among different demographic groups: The HELIUS study. PLoS ONE 2018, 13, e0203483. [Google Scholar] [CrossRef]
- Judge, T.A.; Bono, J.E. Relationship of core self-evaluations traits--self-esteem, generalized self-efficacy, locus of control, and emotional stability--with job satisfaction and job performance: A meta-analysis. J. Appl. Psychol. 2001, 86, 80–92. [Google Scholar] [CrossRef]
- Jones, T.L.; Prinz, R.J. Potential roles of parental self-efficacy in parent and child adjustment: A review. Clin. Psychol. Rev. 2005, 25, 341–363. [Google Scholar] [CrossRef]
- Leahy-Warren, P.; McCarthy, G. Maternal parental self-efficacy in the postpartum period. Midwifery 2011, 27, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Sprang, G.; Silman, M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med. Public Health Prep. 2013, 7, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- de Quervain, D.; Aerni, A.; Amini, E.; Bentz, D.; Coynel, D.; Freytag, V.; Gerhards, C.; Papassotiropoulos, A.; Schicktanz, N.; Schilitt, T.; et al. The Swiss Corona Stress Study: Second Pandemic Wave, November 2020. OSF Prepr. 2020. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Salvador, Á.; Crespo, C.; Barros, L. The Benefits of Family-Centered Care for Parental Self-Efficacy and Psychological Well-being in Parents of Children with Cancer. J. Child Fam. Stud. 2019, 28, 1926–1936. [Google Scholar] [CrossRef]
- O’Brien, K.; Robson, K.; Bracht, M.; Cruz, M.; Lui, K.; Alvaro, R.; da Silva, O.; Monterrosa, L.; Narvey, M.; Ng, E.; et al. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: A multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc. Health 2018, 2, 245–254. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman, W.H., Ed.; Henry Holt and Company: Equitable Building, NY, USA, 1997; 604p. [Google Scholar]
- Ionio, C.; Colombo, C.; Brazzoduro, V.; Mascheroni, E.; Confalonieri, E.; Castoldi, F.; Lista, G. Mothers and Fathers in NICU: The Impact of Preterm Birth on Parental Distress. Eur. J. Psychol. 2016, 12, 604–621. [Google Scholar] [CrossRef]
- Otu, A.; Charles, C.H.; Yaya, S. Mental health and psychosocial well-being during the COVID-19 pandemic: The invisible elephant in the room. Int. J. Ment. Health Syst. 2020, 14, 38. [Google Scholar] [CrossRef]
- Beck, A. Depression: Clinical, Experimental, and Theoretical Aspects; Harper & Row: Manhattan, NY, USA, 1967. [Google Scholar]
- Reilly, L.C.; Ciesla, J.A.; Felton, J.W.; Weitlauf, A.S.; Anderson, N.L. Cognitive vulnerability to depression: A comparison of the weakest link, keystone and additive models. Cogn. Emot. 2012, 26, 521–533. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Lian, B.; Song, X.; Hou, T.; Deng, G.; Li, H. A cross-sectional study on mental health among health care workers during the outbreak of Corona Virus Disease 2019. Asian J. Psychiatry 2020, 51, 102111. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef] [PubMed]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef]
- Ruiz-Zaldibar, C.; Serrano-Monzó, I.; Mujika, A. Parental competence programs to promote positive parenting and healthy lifestyles in children: A systematic review. J. Pediatr. (Rio J.) 2018, 94, 238–250. [Google Scholar] [CrossRef]
- Weaver, C.M.; Shaw, D.S.; Dishion, T.J.; Wilson, M.N. Parenting self-efficacy and problem behavior in children at high risk for early conduct problems: The mediating role of maternal depression. Infant Behav. Dev. 2008, 31, 594–605. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).