
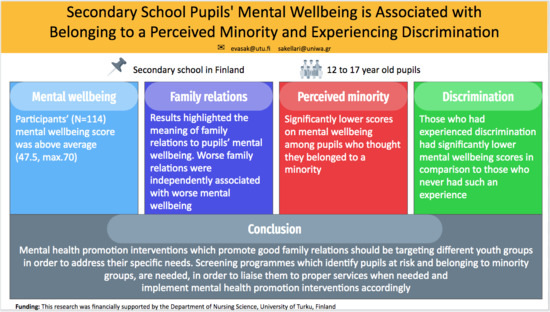
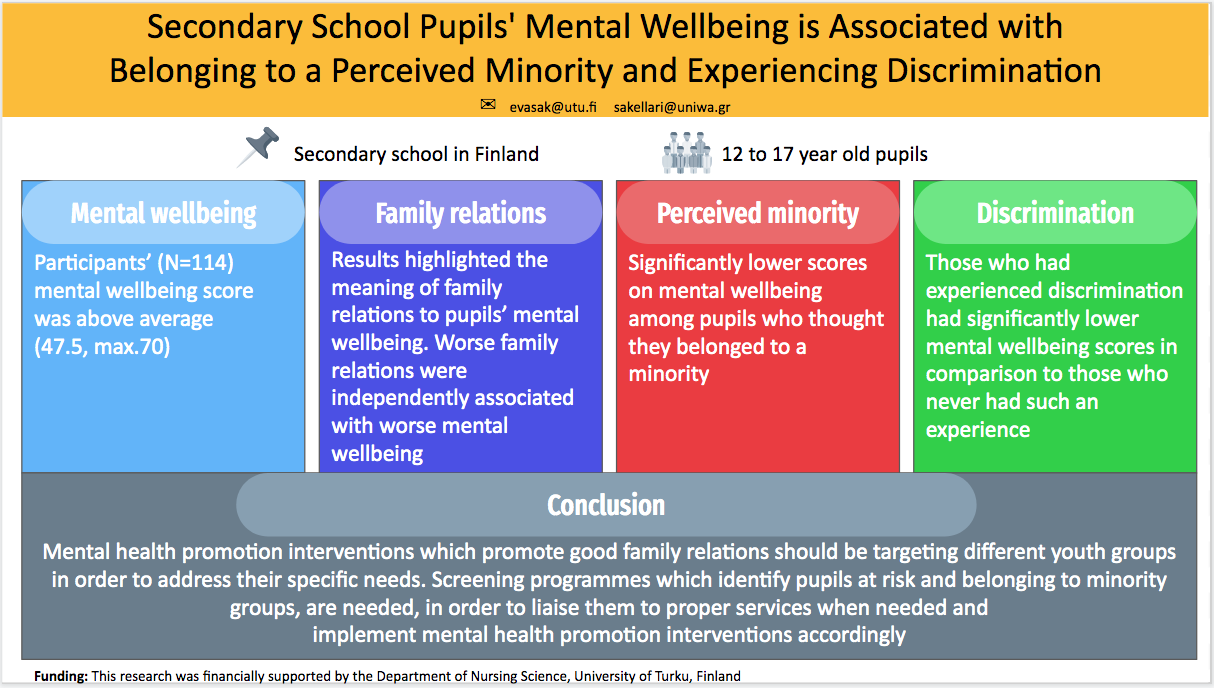
Secondary School Pupils’ Mental Wellbeing Is Associated with Belonging to a Perceived Minority and Experiencing Discrimination

 ,
,
Abstract
1. Introduction
- What is the adolescents’ level of mental wellbeing?
- Are socioeconomic factors associated with the adolescents’ level of mental wellbeing?
- Is the perception of belonging in a minority a factor associated with the adolescents’ level of mental wellbeing?
- Is the perception of experiencing discrimination a factor associated with the adolescents’ level of mental wellbeing?
2. Materials and Methods
2.1. Participants and Setting
2.2. Data Collection and Measures
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Adolescents Mental Well-Being. Fact Sheet. 2016. Available online: https://www.euro.who.int/__data/assets/pdf_file/0020/303482/HBSC-No.7_factsheet_Well-being.pdf?ua=1 (accessed on 4 January 2021).
- O’Reilly, M.; Adams, S.; Whiteman, N.; Hughes, J.; Reilly, P.; Dogra, N. Whose Responsibility is Adolescent’s Mental Health in the UK? Perspectives of Key Stakeholders. School Ment. Health. 2018, 10, 450–461. [Google Scholar] [CrossRef]
- World Health Organization. Giving Adolescents a Voice: Conducting a Rapid Assessment of Adolescent Health Needs: A Manual for Health Planners and Researchers. 2001. Available online: https://iris.wpro.who.int/handle/10665.1/5494 (accessed on 20 January 2021).
- Savolainen, O.; Turunen, H.; Sormunen, M. Municipal strategies and meeting minutes’ descriptions of the promotion of children’s mental health: A document analysis. Scand. J. Public Health 2020. [Google Scholar] [CrossRef]
- Rees, G.; Goswami, H.; Pople, L.; Bradshaw, J.; Keung, A.; Main, G. The Good Childhood Report; The Children’s Society: London, UK, 2013. [Google Scholar]
- Lin, N.; Dean, A.; Ensel, W.M. Social Support, Life Events, and Depression; Academic Press: New York, NY, USA, 1986. [Google Scholar]
- Bal, S.; Crombez, G.; Van Oost, P.; Debourdeaudhuij, I. The role of social support in well-being and coping with self-reported stressful events in adolescents. Child Abuse Negl. 2003, 27, 1377–1395. [Google Scholar] [CrossRef]
- Camara, M.; Bacigalupe, G.; Padilla, P. The role of social support in adolescents: Are you helping me or stressing me out? Int. J. Adolesc. Youth 2017, 22, 123–136. [Google Scholar] [CrossRef]
- Patalay, P.; Fitzsimmons, E. Correlates of mental illness and wellbeing in children: Are they the same? Results from the UK millennium cohort study. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Rees, G.; Bradshaw, J.; Goswami, H.; Keung, A. Understanding Children’s Well-Being: A National Survey of Young People’s Well-Being; The Children’s Society: London, UK, 2009. [Google Scholar]
- Vukojević, M.; Zovko, A.; Talić, I.; Tanović, M.; Rešić, B.; Vrdoljak, I.; Splavski, B. Parental Socioeconomic Status as a Predictor of Physical and Mental Health Outcomes in Children—Literature Review. Acta Clin. Croat. 2017, 56, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Ge, T. Effect of socioeconomic status on children’s psychological well-being in China: The mediating role of family social capital. J. Health Psychol. 2020, 25, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, C.J. Parents’ Employment and Children’s Wellbeing. Future Child. 2014, 24, 121–146. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. 2016. Available online: www.euro.who.int/en/publications/abstracts/growing-up-unequal.-hbsc-2016-study-20132014-survey (accessed on 4 January 2021).
- Moksnes, U.K.; Løhre, A.; Lillefjell, M.; Byrne, D.G.; Haugan, G. The Association between School Stress, Life Satisfaction and Depressive Symptoms in Adolescents: Life Satisfaction as a Potential Mediator. Soc. Indic. Res. 2016, 125, 339–357. [Google Scholar] [CrossRef]
- Pascoe, E.A.; Smart Richman, L. Perceived discrimination and health: A meta-analytic review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. Discrimination: What It Is, and How to Cope. 2019. Available online: https://www.apa.org/helpcenter/discrimination (accessed on 4 January 2021).
- Andriessen, I.; Fernee, H.; Wittebrood, K. Perceived Discrimination in the Netherlands; Institute for Social Research: Hague, The Netherlands, 2014. [Google Scholar]
- Straiton, M.L.; Aambø, A.K.; Johansen, R. Perceived discrimination, health and mental health among immigrants in Norway: The role of moderating factors. BMC Public Health 2019, 19, 325. [Google Scholar] [CrossRef] [PubMed]
- Stone, D.M.; Luo, F.; Ouyang, L.; Lippy, C.; Hertz, M.F.; Crosby, A.E. Sexual orientation and suicide ideation, plans, attempts, and medically serious attempts: Evidence from local Youth Risk Behavior Surveys 2001–2009. Am. J. Public Health. 2014, 104, 262–271. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, A.B.; Gould, M.S. Global trends in teenage suicide: 2003–2014. QJM Int. J. Med. 2015, 108, 765–780. [Google Scholar] [CrossRef] [PubMed]
- Kouider, E.B.; Koglin, U.; Petermann, F. Emotional and behavioral problems in migrant children and adolescents in Europe: A systematic review. Eur. Child Adolesc. Psychiatry 2014, 24, 373–391. [Google Scholar] [CrossRef]
- National Research Council (US) and Institute of Medicine (US). Committee on the Prevention of Mental Disorders and Substance Abuse among Children, Youth, and Young Adults: Research Advances and Promising Interventions; Preventing Mental, Emotional, and Behavioral Disorders among Young People: Progress and Possibilities; O’Connell, M.E., Boat, T., Warner, K.E., Eds.; National Academies Press: Washington, DC, USA, 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK32775/ (accessed on 4 January 2021). [CrossRef]
- Lippman, L.H.; Ryberg, R.; Terzian, M.; Moore, K.A.; Humble, J.; McIntosh, H. Positive and Protective Factors in Adolescent Well-Being. In Handbook of Child Well-Being; Ben-Arieh, A., Casas, F., Frønes, I., Korbin, J., Eds.; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar] [CrossRef]
- Public Health England. Measuring Mental Wellbeing in Children and Young People. 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/768983/Measuring_mental_wellbeing_in_children_and_young_people.pdf (accessed on 4 January 2021).
- Nishida, A.; Richards, M.; Stafford, M. Prospective associations between adolescent mental health problems and positive mental wellbeing in early old age. Child Adolesc. Psychiatry Ment. Health 2016, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health for the World’s Adolescents. A Second Chance in the Second Decade. 2014. Available online: https://www.who.int/maternal_child_adolescent/documents/second-decade/en/ (accessed on 4 January 2021).
- Eurydice (2020) Finland. Single Structure Education (Integrated Primary and Lower Secondary Education). Available online: https://eacea.ec.europa.eu/national-policies/eurydice/finland/single-structure-education-integrated-primary-and-lower-secondary-education_en (accessed on 4 January 2021).
- City of Turku. Determination of the School. 2020. Available online: https://www.turku.fi/en/daycare-and-education/basic-education/determination-school (accessed on 4 January 2021).
- Appelqvist-Schmidlechner, K.; Tuisku, K.; Tamminen, N.; Nordling, E.; Solin, P. Mitä positiivinen mielenterveys on ja kuinka sitä mitataan? [What is positive mental health and how to measure it]. Suom. Lääkärilehti [Doctors’ J.] 2016, 24, 1759–1764. [Google Scholar]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Myllyniemi, S. Ihmisarvoinen nuoruus. Nuorisobarometri [Dignified Youth. Youth Barometer]; Opetus-ja Kulttuuriministeriö. Nuorisoasiain Neuvottelukunta. Nuorisotutkimusverkosto [Ministry of Education and Culture, Advisory Council for Youth Affairs. Finnish Conference on Youth Studies]; Nuorisoasiain neuvottelukunnan julkaisuja [Advisory Council for Youth Affairs Publications]: Helsinki, Finland, 2014; ISSN 1455-268X. [Google Scholar]
- Tutkimuseettinen Neuvottelukunta (TENK) [National Advisory Board on Research Ethics]. Humanistisen, Yhteiskuntatieteellisen ja Käyttäytymistieteellisen Tutkimuksen Eettiset Periaatteet ja Ehdotus Eettisen Ennakkoarvioinnin Järjestämiseksi [Ethical Principles for Humanistic, Social and Behavioural Research and a Proposal for Organizing Ethical Pre-Evaluation]; Tenk: Helsinki, Finland, 2009. [Google Scholar]
- Clarke, A.; Putz, R.; Friede, T.; Ashdown, J.; Adi, Y.; Martin, S.; Flynn, P.; Blake, A.; Stewart-Brown, S.; Platt, S. Warwick-Edinburgh Mental Well-being Scale (WEMWBS) Acceptability and Validation in English and Scottish Secondary School Students (The WAVES Project). 2010. Available online: http://healthscotland.scot/media/1720/16796-wavesfinalreport.pdf (accessed on 4 January 2021).
- Reiss, F.; Meyrose, A.-K.; Otto, C.; Lampert, T.; Klasen, F.; Ravens-Sieberer, U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: Results of the German BELLA cohort study. PLoS ONE 2019, 14, e0213700. [Google Scholar] [CrossRef]
- Torikka, A.; Kaltiala-Heino, R.; Rimpelä, A.; Marttunen, M.; Luukkaala, T.; Rimpelä, M. Self-reported Depression Is Increasing among Socio-Economically Disadvantaged Adolescents—Repeated Cross-Sectional Surveys from Finland from 2000 to 2011. BMC Public Health 2014, 14, 408. [Google Scholar] [CrossRef]
- Schlechter, M.; Milevsky, A. Parental level of education: Associations with psychological well-being, academic achievement and reasons for pursuing higher education in adolescence. Educ. Psychol. 2010, 30, 1–10. [Google Scholar] [CrossRef]
- Bjørnsen, H.N.; Espnes, G.A.; Eilertsen, M.-E.B.; Ringdal, R.; Moksnes, U.K. The Relationship between Positive Mental Health Literacy and Mental Well-Being among Adolescents: Implications for School Health Services. J. Sch. Nurs. 2019, 35, 107–116. [Google Scholar] [CrossRef]
- Gutman, L.M.; Vorhaus, J. The Impact of Pupil Behaviour and Wellbeing on Educational Outcomes. Childhood Wellbeing Research Centre. 2012. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/219638/DFE-RR253.pdf (accessed on 14 January 2021).
- Yeo, S.C.; Tan, J.; Lo, J.C.; Chee, M.W.L.; Gooley, J.J. Associations of time spent on homework or studying with nocturnal sleep behavior and depression symptoms in adolescents from Singapore. Sleep Health 2020, 6, 758–766. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.; Molcho, M.; Martin Weber, M.; et al. Health Policy for Children and Adolescents, No. 7. Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. W.H.O. 2016. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/303438/HSBC-No.7-Growing-up-unequal-Full-Report.pdf (accessed on 4 January 2021).
- Sakellari, E. Exploring the Impact of Mental Health Education on Adolescents’ Perceptions about Mental Health and Mental Illness. Improving Community Health. Ph.D. Thesis, Department of Nursing Science, University of Turku, Turku, Finland, 2014. Annales Universitatis Turkuensis D 1133. Available online: https://www.utupub.fi/bitstream/handle/10024/98972/Annales%20D%201133%20Sakellari%20DISS%20%281%29.pdf?sequence=2&isAllowed=y (accessed on 20 January 2021).
- Myllyniemi, S. Monipolvinen hyvinvointi [Multigenerational wellbeing]. Nuorisobarometri 2012 [Youth Barometer 2012]; Opetus-ja kulttuuriministeriö. Nuorisotutkimusverkosto [Ministry of Education and Culture. Finnish Conference on Youth Studies]; Nuorisoasiain neuvottelukunta [Advisory Council for Youth Affairs]: Helsinki, Finland, 2012. [Google Scholar]
- Hasumi, T.; Ahsan, F.; Couper, C.M.; Laguayo, J.L.; Jacobsen, K.H. Parental Involvement and Mental Well-being of Indian Adolescents. Indian Pediatr. 2012, 49, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.E.; Horwitz, A.; Thomas, A.; Opperman, K.; Gipson, P.; Burnside, A.; Stone, D.M.; King, C.A. Connectedness to family, school, peers, and community in socially vulnerable adolescents. Child Youth Serv. Rev. 2017, 81, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Sourander, A.; McGrath, P.J.; Ristkari, T.; Cunningham, C.; Huttunen, J.; Lingley-Pottie, P.; Hinkka-Yli-Salomäki, S.; Kinnunen, M.; Vuorio, J.; Sinokki, A.; et al. Internet-Assisted Parent Training Intervention for Disruptive Behavior in 4-year-old Children: A Randomized Control Trial. JAMA Psychiatry 2016, 73, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.M.; Janta, B.; Gardner, F. Positive Parenting Interventions. Empowering Parents with Positive Parenting Techniques for Lifelong Health and Well-Being. 2019. Available online: https://op.europa.eu/en/publication-detail/-/publication/d4226270-6a28-11e9-9f05-01aa75ed71a1/language-en (accessed on 4 January 2021).
- McDaid, D.; Zechmeister, I.; Kilian, R.; Medeiros, R.; Knapp, M.; Kennelly, B.; The MHEEN Group. Making the Economic Case for the Promotion of Mental Well-Being and the Prevention of Mental Health Problems. 2008. Personal Social Services Unit, London School of Economics and Political Science Houghton Street. London. Available online: http://eprints.lse.ac.uk/4274/1/MHEEN_policy_briefs_3_promotion(LSERO).pdf (accessed on 4 January 2021).
- Anttila, N.; Huurre, T.; Malin, M.; Santalahti, P. Mielenterveyden edistäminen varhaiskasvatuksesta toisen asteen koulutukseen. Katsaus menetelmiin ja kirjallisuu-teen Suomessa [Promoting Mental Health from Early Childhood Education to Secondary Education. Review of Methods and Literature in Finland]; Työpaperi 3/2016 [Working paper 3/2016]; Terveyden ja hyvinvoinnin laitos (THL) [Finnish Institute for Health and Welfare]: Helsinki, Finland, 2016; Available online: https://www.julkari.fi/bitstream/handle/10024/130003/URN_ISBN_978-952-302-613-1.pdf?sequence=1 (accessed on 4 January 2021).
- Elamé, E. Discriminatory Bullying; Springer: Milano, Italy, 2013. [Google Scholar] [CrossRef]
- Benner, A.D.; Wang, Y.; Shen, Y.; Boyle, A.E.; Polk, R.; Cheng, Y.P. Racial/ethnic discrimination and well-being during adolescence: A meta-analytic review. Am. Psychol. 2018, 73, 855–883. [Google Scholar] [CrossRef]
- Ríos-Salas, V.; Larson, A. Perceived discrimination, socioeconomic status, and mental health among Latino adolescents in US immigrant families. Child Youth Serv. Rev. 2015, 56, 116–125. [Google Scholar] [CrossRef]
- Wilson, E.C.; Chen, Y.-H.; Arayasirikul, S.; Raymond, H.F.; McFarland, W. The impact of discrimination on the mental health of trans*female youth and the protective effect of parental support. AIDS Behav. 2016, 20, 2203–2211. [Google Scholar] [CrossRef]
- Assari, S.; Moazen-Zadeh, E.; Caldwell, C.H.; Zimmerman, M.A. Racial discrimination during adolescence predicts mental health deterioration in adulthood: Gender differences among blacks. Front. Public Health 2017, 5, 104. [Google Scholar] [CrossRef]
- Amos, R.; Manalastas, E.J.; White, R.; Bos, H.; Patalay, P. Mental health, social adversity, and health-related outcomes in sexual minority adolescents: A contemporary national cohort study. Lancet Child Adolesc. Health. 2020, 4, 36–45. [Google Scholar] [CrossRef]
- Watson, R.J.; Peter, T.; McKay, T.; Edkins, T.; Saewyc, E. Evidence of changing patterns in mental health and depressive symptoms for sexual minority adolescents. J. Gay Lesbian Ment. Health. 2018, 22, 120–138. [Google Scholar] [CrossRef]
- Marshal, M.P.; Dietz, L.J.; Friedman, M.S.; Stall, R.; Smith, H.A.; McGinley, J.; Thoma, B.C.; Murray, P.J.; D’Augelli, A.R.; Brent, D.A. Suicidality and Depression Disparities Between Sexual Minority and Heterosexual Youth: A Meta-Analytic Review. J Adolesc. Health. 2011, 49, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.R.; Choukas-Bradley, S.; Salk, R.H.; Marshal, M.P.; Thoma, B.C. Mental health among sexual and gender minority adolescents: Examining interactions with race and ethnicity. J. Consult. Clin. Psychol. 2020, 88, 402–415. [Google Scholar] [CrossRef]
- Delamater, A.M.; Guzman, A.; Aparicio, K. Mental health issues in children and adolescents with chronic illness. Int. J. Hum. Rights Healthc. 2017, 10, 163–173. [Google Scholar] [CrossRef]
- Travlos, V.; Downs, J.; Wilson, A.; Hince, D.; Patman, S. Mental wellbeing in non-ambulant youth with neuromuscular disorders: What makes the difference? Neuromuscul. Disord. 2019, 29, 48–58. [Google Scholar] [CrossRef]
- Spears Brown, C. Discrimination in Childhood and Adolescence: A Developmental Intergroup Approach; Taylor & Francis: Oxfordshire, UK, 2017. [Google Scholar]
- European Commission. Special Eurobarometer 493. Report. 2019. Available online: https://ec.europa.eu/commfrontoffice/publicopinionmobile/index.cfm/Survey/getSurveyDetail/surveyKy/2251 (accessed on 6 January 2021).
- Katz-Wise, S.L.; Rosario, M.; Tsappis, M. Lesbian, Gay, Bisexual, and Transgender Youth and Family Acceptance. Pediatr. Clin. N. Am. 2016, 63, 1011–1025. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.M.B.; Bandara, D.K.; Robinson, E.M.; Atatoa Carr, P.E. In the 21st Century, what is an acceptable response rate? Aust. N. Z. J. Publ. Health 2012, 36, 106–108. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | n (%) |
|---|---|
| Age (years) | |
| <16 | 48 (42.1) |
| ≥16 | 66 (57.9) |
| Gender | |
| Male | 49 (42.1) |
| Female | 63 (55.3) |
| Other | 2 (1.7) |
| Father’s occupation status | |
| Other * | 24 (21.1) |
| Employed | 90 (78.9) |
| Mother’s occupation status | |
| Other * | 20 (17.5) |
| Employed | 94 (82.5) |
| Educational level of the father | |
| Don’t know | 47 (41.2) |
| ≤12 years | 27 (23.7) |
| >12 years | 40 (35.1) |
| Educational level of the mother | |
| Don’t know | 41 (36) |
| ≤12 years | 20 (17.5) |
| >12 years | 53 (46.5) |
| Living with | |
| Both parents | 72 (63.2) |
| One parent | 34 (29.8) |
| Other ** | 8 (7) |
| Relation with family (1 = excellent to 10 = very bad), median (IQR) | 2 (1–3) |
| Diagnosed emotional difficulties | |
| No | 104 (91.2) |
| Yes | 10 (8.8) |
| Pressure from homework | |
| None/little | 59 (51.8) |
| Enough/very much | 55 (48.2) |
| Belonging to a minority due to: | |
| Ideology | |
| No | 107 (93.9) |
| Yes | 7 (6.1) |
| Religion | |
| No | 107 (93.9) |
| Yes | 7 (6.1) |
| Origin | |
| No | 110 (96.5) |
| Yes | 4 (3.5) |
| Appearance | |
| No | 107 (93.9) |
| Yes | 7 (6.1) |
| Sexual orientation | |
| No | 107 (93.9) |
| Yes | 7 (6.1) |
| Chronic disease | |
| No | 110 (96.5) |
| Yes | 4 (3.5) |
| Gender identity | |
| No | 110 (96.5) |
| Yes | 4 (3.5) |
| Other | |
| No | 111 (97.4) |
| Yes | 3 (2.6) |
| Belong to any minority | |
| No | 90 (78.9) |
| Yes | 24 (21.1) |
| Have you ever experienced discrimination | |
| No | 47 (41.2) |
| Can’t answer | 15 (13.2) |
| Yes | 52 (45.6) |
| Warwick–Edinburgh Mental Well-Being Scale Score | |||
|---|---|---|---|
| Mean | SD | p | |
| Age (years) | |||
| <16 | 46.8 | 14.3 | 0.620 ǁ |
| ≥16 | 48.0 | 12.3 | |
| Gender | |||
| Male | 47.2 | 16.1 | 0.733 ǁ |
| Female | 48.1 | 10.6 | |
| Father’s occupation status | |||
| Other * | 46.5 | 13.9 | 0.673 ǁ |
| Employed | 47.8 | 13.0 | |
| Mother’s occupation status | |||
| Other * | 44.7 | 12.1 | 0.285 ǁ |
| Employed | 48.1 | 13.3 | |
| Educational level of the father | |||
| Don’t know | 43.6 | 14.7 | 0.053 ¶ |
| ≤12 years | 50.6 | 11.6 | |
| >12 years | 50.0 | 11.0 | |
| Educational level of the mother | |||
| Don’t know A | 42.3 C | 15.2 | 0.004 ¶ |
| ≤12 years B | 48.4 | 12.2 | |
| >12 years C | 51.2 A | 10.2 | |
| Living with | |||
| Both parents A | 48.9 B | 12.9 | 0.018 ¶ |
| One parent B | 42.7 A,C | 12.9 | |
| Other C | 54.9 | 10.4 | |
| Diagnosed emotional difficulties | |||
| No | 47.0 | 13.0 | 0.209 ǁ |
| Yes | 52.5 | 13.6 | |
| Pressure from homework | |||
| None/little | 50.6 | 11.5 | 0.008 ǁ |
| Enough/very much | 44.1 | 14.0 | |
| Warwick–Edinburgh Mental Well-Being Scale Score | |||
|---|---|---|---|
| Mean | SD | p | |
| Belonging to a minority due to: | |||
| Ideology | |||
| No (n = 107) | 47.7 | 13.3 | 0.467 ǁ |
| Yes (n = 7) | 44.0 | 10.1 | |
| Religion | |||
| No (n = 107) | 48.0 | 12.8 | 0.158 ǁ |
| Yes (n = 7) | 40.7 | 16.9 | |
| Origin | |||
| No (n = 110) | 47.6 | 12.8 | 0.846 ǁ |
| Yes (n = 4) | 46.3 | 23.0 | |
| Appearance | |||
| No (n = 107) | 48.2 | 12.4 | 0.020 ǁ |
| Yes (n = 4) | 36.4 | 19.2 | |
| Sexual orientation | |||
| No (n = 107) | 48.2 | 12.9 | 0.035 ǁ |
| Yes (n = 7) | 37.4 | 13.3 | |
| Chronic disease | |||
| No (n = 110) | 48.0 | 13.0 | 0.039 ǁ |
| Yes (n = 4) | 34.3 | 11.6 | |
| Gender identity | |||
| No (n = 110) | 47.9 | 12.9 | 0.120 ǁ |
| Yes (n = 4) | 37.5 | 17.6 | |
| Other | |||
| No (n = 111) | 47.8 | 12.9 | 0.221 ǁ |
| Yes (n = 3) | 38.3 | 21.8 | |
| Belong to any minority | |||
| No (n = 90) | 48.4 | 12.6 | 0.141 ǁ |
| Yes (n = 24) | 44.0 | 14.6 | |
| Experienced discrimination | |||
| No A (n = 47) | 52.1 C | 12.4 | 0.006 ¶ |
| Can’t answer B (n = 15) | 45.1 | 9.6 | |
| Yes C (n = 52) | 44.1 A | 13.5 | |
| β ⱡ | SE ǁ | b ¶ | p | |
|---|---|---|---|---|
| Mother’s educational level: | ||||
| Other, reference | ||||
| >12 years | 4.83 | 2.19 | 0.18 | 0.029 |
| Relation with family (1 = excellent to 10 = very bad) | −2.00 | 0.59 | −0.29 | 0.001 |
| Belonging to a minority due to sexual orientation: | ||||
| No, reference | ||||
| Yes | −10.13 | 3.99 | −0.22 | 0.013 |
| Belonging to a minority due to chronic disease: | ||||
| No, reference | ||||
| Yes | −12.23 | 5.89 | −0.17 | 0.040 |
| Have you ever experienced discrimination: | ||||
| No, reference | ||||
| Can’t answer | −2.52 | 3.51 | −0.07 | 0.474 |
| Yes | −6.92 | 2.44 | −0.26 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kokkonen, P.; Athanasopoulou, C.; Leino-Kilpi, H.; Sakellari, E. Secondary School Pupils’ Mental Wellbeing Is Associated with Belonging to a Perceived Minority and Experiencing Discrimination. Children 2021, 8, 71. https://doi.org/10.3390/children8020071
Kokkonen P, Athanasopoulou C, Leino-Kilpi H, Sakellari E. Secondary School Pupils’ Mental Wellbeing Is Associated with Belonging to a Perceived Minority and Experiencing Discrimination. Children. 2021; 8(2):71. https://doi.org/10.3390/children8020071
Chicago/Turabian StyleKokkonen, Pinja, Christina Athanasopoulou, Helena Leino-Kilpi, and Evanthia Sakellari. 2021. "Secondary School Pupils’ Mental Wellbeing Is Associated with Belonging to a Perceived Minority and Experiencing Discrimination" Children 8, no. 2: 71. https://doi.org/10.3390/children8020071
APA StyleKokkonen, P., Athanasopoulou, C., Leino-Kilpi, H., & Sakellari, E. (2021). Secondary School Pupils’ Mental Wellbeing Is Associated with Belonging to a Perceived Minority and Experiencing Discrimination. Children, 8(2), 71. https://doi.org/10.3390/children8020071