
Level of Adherence to the Mediterranean Diet and Weight Status among Adolescent Female Gymnasts: A Cross-Sectional Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Inclusion and Exclusion Criteria
2.3. Ethical Permission, Consent and Anonymity
2.4. Questionnaires and Tools Applied
2.4.1. Adherence to the MD
2.4.2. Social Desirability Scale
2.4.3. Anthropometric Indices
2.5. Statistical Analyses
3. Results
3.1. Population Characteristics
3.2. Anthromometric Characteristics
3.3. Adherence to the MD
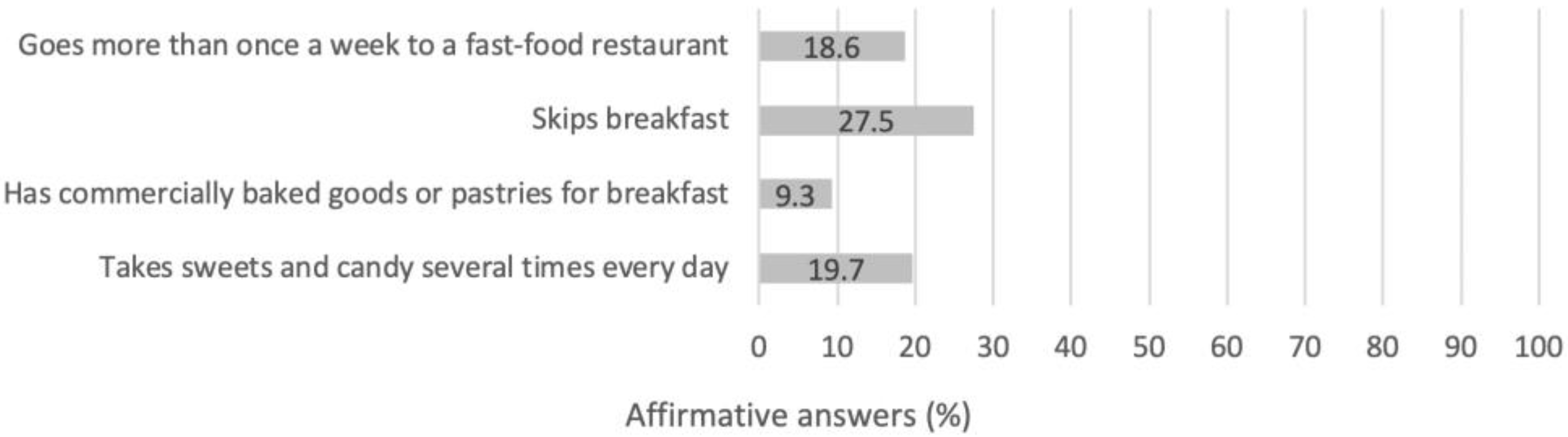
3.4. Individual Eating Habits
4. Discussion
4.1. Anthropometric Characteristics
4.2. Adherence to the MD
4.3. Adherence to the MD with Respect to Anthropometric Characteristics
4.4. Individual Eating Habits and BMI
4.5. Limitations
4.6. Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spear, B.A. Adolescent growth and development. J. Am. Diet. Assoc. 2002, 102, S23–S29. [Google Scholar] [CrossRef]
- United Nations Children’s Fund (UNICEF). Programming Guidance: Nutrition in Middle Childhood and Adolescence; UNICEF: New York, NY, USA, 2021.
- Grammatikopoulou, M.G.; Gkiouras, K.; Daskalou, E.; Apostolidou, E.; Theodoridis, X.; Stylianou, C.; Galli-Tsinopoulou, A.; Tsigga, M.; Dardavessis, T.; Chourdakis, M. Growth, the Mediterranean diet and the buying power of adolescents in Greece. J. Pediatr. Endocrinol. Metab. 2018, 31, 773–780. [Google Scholar] [CrossRef]
- Christian, P.; Smith, E.R. Adolescent Undernutrition: Global Burden, Physiology, and Nutritional Risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef]
- Prentice, A.M.; Ward, K.A.; Goldberg, G.R.; Jarjou, L.M.; Moore, S.E.; Fulford, A.J.; Prentice, A. Critical windows for nutritional interventions against stunting. Am. J. Clin. Nutr. 2013, 97, 911–918. [Google Scholar] [CrossRef] [Green Version]
- Inchley, J.; Currie, D.; Budisavljevic, S.; Torsheim, T.; Jåstad, A.; Cosma, A.; Kelly, C.; Arnarsson, Á.M. Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report. Volume 1. Key Findings; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Benetou, V.; Kanellopoulou, A.; Kanavou, E.; Fotiou, A.; Stavrou, M.; Richardson, C.; Orfanos, P.; Kokkevi, A. Diet-Related Behaviors and Diet Quality among School-Aged Adolescents Living in Greece. Nutrients 2020, 12, 3804. [Google Scholar] [CrossRef]
- Grammatikopoulou, M.G.; Maraki, M.I.; Giannopoulou, D.; Poulimeneas, D.; Sidossis, L.S.; Tsigga, M. Similar Mediterranean diet adherence but greater central adiposity is observed among Greek diaspora adolescents living in Istanbul, compared to Athens. Ethn. Health 2018, 23, 221–232. [Google Scholar] [CrossRef]
- Klimis-Zacas, D.J.; Kalea, A.Z.; Yannakoulia, M.; Matalas, A.L.; Vassilakou, T.; Papoutsakis-Tsarouhas, C.; Yiannakouris, N.; Polychronopoulos, E.; Passos, M. Dietary intakes of Greek urban adolescents do not meet the recommendations. Nutr. Res. 2007, 27, 18–26. [Google Scholar] [CrossRef]
- Ludwig, D.S. Weight loss strategies for adolescents: A 14-year-old struggling to lose weight. JAMA 2012, 307, 498–508. [Google Scholar] [CrossRef]
- Mendes, V.; Araújo, J.; Lopes, C.; Ramos, E. Determinants of weight loss dieting among adolescents: A longitudinal analysis. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2014, 54, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Carter, S.; Constantini, N.; Lebrun, C.; Meyer, N.; Sherman, R.; Steffen, K.; Budgett, R.; et al. Relative Energy Deficiency in Sport (RED-S). Br. J. Sports Med. 2015, 49, 421–423. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.A.; Dewoolkar, A.V.; Baker, N.; Dodich, C. The female athlete triad: Special considerations for adolescent female athletes. Transl. Pediatr. 2017, 6, 144–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.W.; Holmes, M.E.; McAllister, M.J. Nutritional Considerations for Performance in Young Athletes. J. Sports Med. 2015, 2015, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Hannon, M.P.; Close, G.L.; Morton, J.P. Energy and Macronutrient Considerations for Young Athletes. Strength Cond. J. 2020, 42, 109–119. [Google Scholar] [CrossRef]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P. American College of Sports Medicine position stand. The female athlete triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1882. [Google Scholar] [CrossRef]
- Benardot, D. Gymnastics. In Sports Nutrition; Maughan, R.J., Ed.; John Wiley & Sons, Ltd.: Hichester, UK, 2014; Volume 19, pp. 596–606. [Google Scholar]
- Malina, R.M.; Baxter-Jones, A.D.G.; Armstrong, N.; Beunen, G.P.; Caine, D.; Daly, R.M.; Lewis, R.D.; Rogol, A.D.; Russell, K. Role of intensive training in the growth and maturation of artistic gymnasts. Sports Med. 2013, 43, 783–802. [Google Scholar] [CrossRef] [Green Version]
- Bacciotti, S.; Baxter-Jones, A.; Gaya, A.; Maia, J. The Physique of Elite Female Artistic Gymnasts: A Systematic Review. J. Hum. Kinet. 2017, 58, 247–259. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, H.; Slater, G. Losing, Gaining and Making Weight for Athletes. In Sport and Exercise Nutrition; John Wiley & Sons, Ltd.: Hoboken, NJ, USA; pp. 210–232. ISSN 978-1-4443-4490-5. [CrossRef]
- Sundgot-Borgen, J.; Garthe, I. Elite athletes in aesthetic and Olympic weight-class sports and the challenge of body weight and body composition. J. Sports Sci. 2011, 29 (Suppl. S1), S101–S114. [Google Scholar] [CrossRef]
- Sherman, R.T.; Thompson, R.A.; Rose, J.S. Body mass index and athletic performance in elite female gymnasts. J. Sport Behav. 1996, 19, 338–346. [Google Scholar]
- O’Connor, H. The Overweight Athlete. In The Encyclopaedia of Sports Medicine; John Wiley & Sons, Ltd.: Hichester, UK, 2013; pp. 503–512. ISBN 978-1-118-69231-8. [Google Scholar]
- Claessens, A.L.; Lefevre, J.; Beunen, G.; Malina, R.M. The contribution of anthropometric characteristics to performance scores in elite female gymnasts. J. Sports Med. Phys. Fit. 1999, 39, 355–360. [Google Scholar]
- Malina, R.M. Physical growth and biological maturation of young athletes. Exerc. Sport Sci. Rev. 1994, 22, 389–433. [Google Scholar] [CrossRef]
- Tan, J.O.A.; Calitri, R.; Bloodworth, A.; McNamee, M.J. Understanding Eating Disorders in Elite Gymnastics: Ethical and Conceptual Challenges. Clin. Sports Med. 2016, 35, 275–292. [Google Scholar] [CrossRef]
- Okano, G.; Holmes, R.A.; Mu, Z.; Yang, P.; Lin, Z.; Nakai, Y. Disordered eating in Japanese and Chinese female runners, rhythmic gymnasts and gymnasts. Int. J. Sports Med. 2005, 26, 486–491. [Google Scholar] [CrossRef]
- Sweeney, E.; Howell, D.R.; Seehusen, C.N.; Tilley, D.; Casey, E. Health outcomes among former female collegiate gymnasts: The influence of sport specialization, concussion, and disordered eating. Phys. Sportsmed. 2020, 49, 438–444. [Google Scholar] [CrossRef]
- Donti, O.; Donti, A.; Gaspari, V.; Pleksida, P.; Psychountaki, M. Are they too perfect to eat healthy? Association between eating disorder symptoms and perfectionism in adolescent rhythmic gymnasts. Eat. Behav. 2021, 41, 101514. [Google Scholar] [CrossRef] [PubMed]
- Kontele, I.; Vassilakou, T. Nutritional Risks among Adolescent Athletes with Disordered Eating. Children 2021, 8, 715. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.D.; Castrogiovanni, S.; Barale, A.; Morelli, E. Nutrition survey in elite rhythmic gymnasts. J. Sports Med. Phys. Fit. 2000, 40, 350–355. [Google Scholar]
- Michopoulou, E.; Avloniti, A.; Kambas, A.; Leontsini, D.; Michalopoulou, M.; Tournis, S.; Fatouros, I.G. Elite premenarcheal rhythmic gymnasts demonstrate energy and dietary intake deficiencies during periods of intense training. Pediatr. Exerc. Sci. 2011, 23, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.-R.G.; Paiva, T. Low energy availability and low body fat of female gymnasts before an international competition. Eur. J. Sport Sci. 2014, 15, 591–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, M.-R.G.; Silva, H.-H.; Paiva, T. Sleep duration, body composition, dietary profile and eating behaviours among children and adolescents: A comparison between Portuguese acrobatic gymnasts. Eur. J. Pediatr. 2018, 177, 815–825. [Google Scholar] [CrossRef]
- Thein-Nissenbaum, J.M.; Rauh, M.J.; Carr, K.E.; Loud, K.J.; Mcguine, T.A. Associations between disordered eating, menstrual dysfunction, and musculoskeletal injury among high school athletes. J. Orthop. Sports Phys. Ther. 2011, 41, 60–69. [Google Scholar] [CrossRef]
- Villa, M.; Villa-Vicente, J.G.; Seco-Calvo, J.; Mielgo-Ayuso, J.; Collado, P.S. Body Composition, Dietary Intake and the Risk of Low Energy Availability in Elite-Level Competitive Rhythmic Gymnasts. Nutrients 2021, 13, 2083. [Google Scholar] [CrossRef]
- Miteva, S.; Yanev, I.; Kolimechkov, S.; Petrov, L.; Mladenov, L.; Georgieva, V.; Somlev, P. Nutrition and body composition of elite rhythmic gymnasts from Bulgaria. Int. J. Sports Sci. Coach. 2019, 15, 108–116. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. NMCD 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Jacobs, D.R.; Steffen, L.M. Nutrients, foods, and dietary patterns as exposures in research: A framework for food synergy. Am. J. Clin. Nutr. 2003, 78, 508S–513S. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Implausible results in human nutrition research. BMJ 2013, 347, 66–98. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, J.D.; Ioannidis, J.P. Is everything we eat associated with cancer? A systematic cookbook review. Am. J. Clin. Nutr. 2013, 97, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [Green Version]
- Grammatikopoulou, M.G.; Nigdelis, M.P.; Theodoridis, X.; Gkiouras, K.; Tranidou, A.; Papamitsou, T.; Bogdanos, D.P.; Goulis, D.G. How fragile are Mediterranean diet interventions? A research-on-research study of randomized controlled trials. BMJ Nutr. Prev. Health 2021, 4, e000188. [Google Scholar] [CrossRef]
- Klonizakis, M.; Bugg, A.; Hunt, B.; Theodoridis, X.; Bogdanos, D.P.; Grammatikopoulou, M.G. Assessing the Physiological Effects of Traditional Regional Diets Targeting the Prevention of Cardiovascular Disease: A Systematic Review of Randomized Controlled Trials Implementing Mediterranean, New Nordic, Japanese, Atlantic, Persian and Mexican Dietary Interventions. Nutrients 2021, 13, 3034. [Google Scholar] [CrossRef]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The effect of the mediterranean diet on metabolic health: A systematic review and meta-analysis of controlled trials in adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Mourouti, N.; Papavagelis, C.; Plytzanopoulou, P.; Kontogianni, M.; Vassilakou, T.; Malamos, N.; Linos, A.; Panagiotakos, D. Dietary patterns and breast cancer: A case–control study in women. Eur. J. Nutr. 2015, 54, 609–617. [Google Scholar] [CrossRef]
- Kontogianni, M.D.; Farmaki, A.-E.; Vidra, N.; Sofrona, S.; Magkanari, F.; Yannakoulia, M. Associations between Lifestyle Patterns and Body Mass Index in a Sample of Greek Children and Adolescents. J. Am. Diet. Assoc. 2010, 110, 215–221. [Google Scholar] [CrossRef]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.I.; Dardavessis, T.; Chourdakis, M. Food insecurity and Mediterranean diet adherence among Greek university students. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 477–485. [Google Scholar] [CrossRef]
- Tambalis, K.D.; Panagiotakos, D.B.; Moraiti, I.; Psarra, G.; Sidossis, L.S. Poor dietary habits in Greek schoolchildren are strongly associated with screen time: Results from the EYZHN (National Action for Children’s Health) Program. Eur. J. Clin. Nutr. 2018, 72, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, F.; Lorini, C.; Tanini, T.; Indiani, L.; Lastrucci, V.; Comodo, N.; Bonaccorsi, G. Adherence to mediterranean diet in a sample of Tuscan adolescents. Nutrition 2014, 30, 1379–1383. [Google Scholar] [CrossRef]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Weight Status, Adherence to the Mediterranean Diet, and Physical Fitness in Spanish Children and Adolescents: The Active Health Study. Nutrients 2020, 12, 1680. [Google Scholar] [CrossRef]
- Santana, M.V.; Mirón, I.M.; Vargas, L.A.; Bedoya, J.L. Comparative analysis of adherence to the Mediterranean diet among girls and adolescents who perform rythmic gymnastics. Rev. Bras. Med. Esporte 2019, 25, 280–284. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Poulimeneas, D.; Grammatikopoulou, M.G.; Devetzi, P.; Petrocheilou, A.; Kaditis, A.G.; Papamitsou, T.; Doudounakis, S.E.; Vassilakou, T. Adherence to Dietary Recommendations, Nutrient Intake Adequacy and Diet Quality among Pediatric Cystic Fibrosis Patients: Results from the GreeCF Study. Nutrients 2020, 12, 3126. [Google Scholar] [CrossRef]
- Poulimeneas, D.; Vlachos, D.; Maraki, M.I.; Daskalou, E.; Grammatikopoulou, M.; Karathanou, L.; Kotsias, E.; Tsofliou, F.; Tsigga, M.; Grammatikopoulou, M.G. Diet quality, overweight and daily monetary allowance of Greek adolescents. Int. J. Adolesc. Med. Health 2019, 31, 20170019. [Google Scholar] [CrossRef]
- Reynolds, W.M. Development of reliable and valid short forms of the marlowe-crowne social desirability scale—Reynolds—1982—Journal of Clinical Psychology—Wiley Online Library. J. Clin. Psychol. 1982, 38, 119–125. [Google Scholar] [CrossRef]
- Psychountaki, M.; Ekkekakis, P.; Zervas, I. Short-Form of Social Desirability Scale: Adaptation of the Marlowe-Crowne Scale; National & Kapodistrian University of Athens: Athens, Greece, 1993. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- López-Varela, S.; Montero, A.; Chandra, R.K.; Marcos, A. Nutritional status of young female elite gymnasts. Int. J. Vitam. Nutr. Res. Int. Z. Vitam.-Ernahr. J. Int. Vitaminol. Nutr. 2000, 70, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Soric, M.; Misigoj-Durakovic, M.; Pedisic, Z. Dietary intake and body composition of prepubescent female aesthetic athletes. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 343–354. [Google Scholar] [CrossRef]
- Filaire, E.; Lac, G. Nutritional status and body composition of juvenile elite female gymnasts. J. Sports Med. Phys. Fit. 2002, 42, 65–70. [Google Scholar]
- Avila-Carvalho, L.; Klentrou, P.; Palomero, M.L.; Lebre, E. Body composition profile of elite group rhythmic gymnasts. Sci. Gymnast. J. 2012, 4, 21–32. [Google Scholar]
- D’Alessandro, C.; Morelli, E.; Evangelisti, I.; Galetta, F.; Franzoni, F.; Lazzeri, D.; Piazza, M.; Cupisti, A. Profiling the diet and body composition of subelite adolescent rhythmic gymnasts. Pediatr. Exerc. Sci. 2007, 19, 215–227. [Google Scholar] [CrossRef]
- Grammatikopoulou, M.G.; Poulimeneas, D.; Gounitsioti, I.S.; Gerothanasi, K.; Tsigga, M.; Kiranas, E.; ADONUT Study Group. Prevalence of simple and abdominal obesity in Greek adolescents: The ADONUT study. Clin. Obes. 2014, 4, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Kotanidou, E.P.; Grammatikopoulou, M.G.; Spiliotis, B.E.; Kanaka-Gantenbein, C.; Tsigga, M.; Galli-Tsinopoulou, A. Ten-year obesity and overweight prevalence in Greek children: A systematic review and meta-analysis of 2001–2010 data. Horm. Athens Greece 2013, 12, 537–549. [Google Scholar] [CrossRef] [Green Version]
- Farajian, P.; Risvas, G.; Karasouli, K.; Pounis, G.D.; Kastorini, C.M.; Panagiotakos, D.B.; Zampelas, A. Very high childhood obesity prevalence and low adherence rates to the Mediterranean diet in Greek children: The GRECO study. Atherosclerosis 2011, 217, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Tzotzas, T.; Kapantais, E.; Tziomalos, K.; Ioannidis, I.; Mortoglou, A.; Bakatselos, S.; Kaklamanou, M.; Lanaras, L.; Kaklamanos, I. Epidemiological survey for the prevalence of overweight and abdominal obesity in Greek adolescents. Obesity 2008, 16, 1718–1722. [Google Scholar] [CrossRef]
- Arnaoutis, G.; Georgoulis, M.; Psarra, G.; Milkonidou, A.; Panagiotakos, D.B.; Kyriakou, D.; Bellou, E.; Tambalis, K.D.; Sidossis, L.S. Association of Anthropometric and Lifestyle Parameters with Fitness Levels in Greek Schoolchildren: Results from the EYZHN Program. Front. Nutr. 2018, 5, 10. [Google Scholar] [CrossRef] [Green Version]
- Costarelli, V.; Koretsi, E.; Georgitsogianni, E. Health-related quality of life of Greek adolescents: The role of the Mediterranean diet. Qual. Life Res. 2013, 22, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Kontogianni, M.D.; Vidra, N.; Farmaki, A.-E.; Koinaki, S.; Belogianni, K.; Sofrona, S.; Magkanari, F.; Yannakoulia, M. Adherence rates to the Mediterranean diet are low in a representative sample of Greek children and adolescents. J. Nutr. 2008, 138, 1951–1956. [Google Scholar] [CrossRef] [Green Version]
- Mazaraki, A.; Tsioufis, C.; Dimitriadis, K.; Tsiachris, D.; Stefanadi, E.; Zampelas, A.; Richter, D.; Mariolis, A.; Panagiotakos, D.; Tousoulis, D.; et al. Adherence to the Mediterranean diet and albuminuria levels in Greek adolescents: Data from the Leontio Lyceum ALbuminuria (3L study). Eur. J. Clin. Nutr. 2011, 65, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Zorzou, A.; Kastritsiou, M.; Anagnostopoulou, S.; Balatsouras, M.; Vlassis, I.; Nikolaidis, P. Adherence of Athletes to Mediterranean Diet: A Pilot Study on the Role of Gender and Age. Hell. J. Nutr. Diet. 2019, 11, 131. [Google Scholar]
- Philippou, E.; Middleton, N.; Pistos, C.; Andreou, E.; Petrou, M. The impact of nutrition education on nutrition knowledge and adherence to the Mediterranean Diet in adolescent competitive swimmers. J. Sci. Med. Sport 2017, 20, 328–332. [Google Scholar] [CrossRef]
- Silva, M.-R.G.; Paiva, T. Poor precompetitive sleep habits, nutrients’ deficiencies, inappropriate body composition and athletic performance in elite gymnasts. Eur. J. Sport Sci. 2016, 16, 726–735. [Google Scholar] [CrossRef]
- di Cagno, A.; Baldari, C.; Battaglia, C.; Brasili, P.; Merni, F.; Piazza, M.; Toselli, S.; Ventrella, A.; Guidetti, L. Leaping ability and body composition in rhythmic gymnasts for talent identification. J. Sports Med. Phys. Fit. 2008, 48, 341–346. [Google Scholar]
- Jakše, B.; Jakše, B.; Mis, N.F.; Jug, B.; Šajber, D.; Godnov, U.; Čuk, I. Nutritional Status and Cardiovascular Health in Female Adolescent Elite-Level Artistic Gymnasts and Swimmers: A Cross-Sectional Study of 31 Athletes. J. Nutr. Metab. 2021, 2021, 8810548. [Google Scholar] [CrossRef]
- Collese, T.S.; Nascimento-Ferreira, M.V.; de Moraes, A.C.F.; Rendo-Urteaga, T.; Bel-Serrat, S.; Moreno, L.A.; Carvalho, H.B. Role of fruits and vegetables in adolescent cardiovascular health: A systematic review. Nutr. Rev. 2017, 75, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Leandro, C.G.; Fonseca, E.V.d.S.d.; Lim, C.R.d.; Tchamo, M.E.; Ferreira-e-Silva, W.T. Barriers and Enablers That Influence Overweight/Obesity/Obesogenic Behavior in Adolescents From Lower-Middle Income Countries: A Systematic Review. Food Nutr. Bull. 2019, 40, 562–571. [Google Scholar] [CrossRef]
- Thiel, A.; Diehl, K.; Giel, K.E.; Schnell, A.; Schubring, A.M.; Mayer, J.; Zipfel, S.; Schneider, S. The German Young Olympic Athletes’ Lifestyle and Health Management Study (GOAL Study): Design of a mixed-method study. BMC Public Health 2011, 11, 410. [Google Scholar] [CrossRef] [Green Version]
- Kastorini, C.-M.; Critselis, E.; Zota, D.; Coritsidis, A.L.; Nagarajan, M.K.; Papadimitriou, E.; Belogianni, K.; Benetou, V.; Linos, A.; Team, on behalf of the G.N.D.G.S. National Dietary Guidelines of Greece for children and adolescents: A tool for promoting healthy eating habits. Public Health Nutr. 2019, 22, 2688–2699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, E.A.; Stewart, A.W.; Braithwaite, I.; Murphy, R.; Hancox, R.J.; Wall, C.; Beasley, R.; The ISAAC Phase Three Study Group. Factors associated with body mass index in children and adolescents: An international cross-sectional study. PLoS ONE 2018, 13, e0196221. [Google Scholar] [CrossRef] [Green Version]
- Wall, C.R.; Stewart, A.W.; Hancox, R.J.; Murphy, R.; Braithwaite, I.; Beasley, R.; Mitchell, E.A.; The ISAAC Phase Three Study Group. Association between Frequency of Consumption of Fruit, Vegetables, Nuts and Pulses and BMI: Analyses of the International Study of Asthma and Allergies in Childhood (ISAAC). Nutrients 2018, 10, 316. [Google Scholar] [CrossRef] [Green Version]
- Moreno, J.P.; Johnston, C.A.; El-Mubasher, A.A.; Papaioannou, M.A.; Tyler, C.; Gee, M.; Foreyt, J.P. Peanut consumption in adolescents is associated with improved weight status. Nutr. Res. 2013, 33, 552–556. [Google Scholar] [CrossRef]
- Mead, L.C.; Hill, A.M.; Carter, S.; Coates, A.M. The Effect of Nut Consumption on Diet Quality, Cardiometabolic and Gastrointestinal Health in Children: A Systematic Review of Randomized Controlled Trials. Int. J. Environ. Res. Public. Health 2021, 18, 454. [Google Scholar] [CrossRef] [PubMed]
- Lachat, C.; Nago, E.; Verstraeten, R.; Roberfroid, D.; Van Camp, J.; Kolsteren, P. Eating out of home and its association with dietary intake: A systematic review of the evidence. Obes. Rev. 2012, 13, 329–346. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.S.; Del-Ponte, B.; Assunção, M.C.F.; Santos, I.S. Consumption of ultra-processed foods and body fat during childhood and adolescence: A systematic review. Public Health Nutr. 2018, 21, 148–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapantais, E.; Chala, E.; Kaklamanou, D.; Lanaras, L.; Kaklamanou, M.; Tzotzas, T. Breakfast skipping and its relation to BMI and health-compromising behaviours among Greek adolescents. Public Health Nutr. 2011, 14, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Dialektakou, K.D.; Vranas, P.B.M. Breakfast Skipping and Body Mass Index among Adolescents in Greece: Whether an Association Exists Depends on How Breakfast Skipping Is Defined. J. Am. Diet. Assoc. 2008, 108, 1517–1525. [Google Scholar] [CrossRef]
- Vassilakou, T.; Gnardellis, C.; Trichopoulou, A. Body Mass Index in Relation to Frequency of Breakfast Consumption among Greek Students. Arch. Hell. Med. 2000, 17, 61–67. [Google Scholar]
- Van Diepen, S.; Scholten, A.M.; Korobili, C.; Kyrli, D.; Tsigga, M.; Van Dieijen, T.; Kotzamanidis, C.; Grammatikopoulou, M.G. Greater Mediterranean diet adherence is observed in Dutch compared with Greek university students. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 534–540. [Google Scholar] [CrossRef]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast Habits, Nutritional Status, Body Weight, and Academic Performance in Children and Adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef]
- Blondin, S.A.; Anzman-Frasca, S.; Djang, H.C.; Economos, C.D. Breakfast consumption and adiposity among children and adolescents: An updated review of the literature. Pediatr. Obes. 2016, 11, 333–348. [Google Scholar] [CrossRef]
- Hassan, B.K.; Cunha, D.B.; da Veiga, G.V.; Pereira, R.A.; Hoffman, D.J.; Sichieri, S. Breakfast Consumption, Family Breakfast, and Adiposity Trajectory in Adolescence-The Adolescent Nutritional Assessment Longitudinal Cohort Study. J. Acad. Nutr. Diet. 2019, 119, 944–956. [Google Scholar] [CrossRef]
- Giménez-Legarre, N.; Miguel-Berges, M.L.; Flores-Barrantes, P.; Santaliestra-Pasías, A.M.; Moreno, L.A. Breakfast Characteristics and Its Association with Daily Micronutrients Intake in Children and Adolescents–A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3201. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age (years) | 13.89 ± 1.75 | |
| Body weight (kg) | 47.44 ± 8.84 | |
| Height (cm) | 157.4 ± 8.4 | |
| BMI (kg/m2) | 19.00 ± 2.45 | |
| Weight status | Underweight/normoweight/overweight (n, %) | 28 (10.4%)/226 (84.0%)/15 (5.6%) |
| Sport | Artistic gymnastics (n, %) | n = 50, 18.6% |
| Rhythmic gymnastics (n, %) | n = 42, 15.6% | |
| Trampoline and tumbling (n, %) | n = 65, 24.2% | |
| Acrobatics and aerobics (n, %) | n = 22, 8.2% | |
| Gymnastics for all (n, %) | n = 90, 33.5% | |
| Competition level: international/national/local (%) | 20.2%/50.2%/29.6% | |
| Duration of training: >8 years/6–8 years/<6 years (%) | 27%/37.5%/35.5% | |
| Weekly training frequency: ≥5 times/3–4 times/1–2 times | 50%/34.3%/15.7% | |
| Artistic Gymnastics (n = 50) | Rhythmic Gymnastics (n = 42) | Trampoline/ Tumbling (n = 65) | Acrobatics/ Aerobics (n = 22) | Gymnastics for All (n = 90) | Significance | |
|---|---|---|---|---|---|---|
| Age (years) | 13.69 ± 1.70 | 13.58 ± 1.64 | 13.99 ± 1.79 | 13.82 ± 1.56 | 14.08 ±1.84 | p = 0.533 |
| Body weight (kg) | 43.9 ± 8.2 | 42.5 ± 6.8 | 49.3 ± 8.7 **,††† | 49.5 ± 8.3 † | 49.9 ± 8.8 ***,††† | p ≤ 0.001 |
| Height (cm) | 152.8 ± 8.71 | 157.2 ± 8.8 | 157.8 ± 8.2 * | 160.8 ± 7.1 *** | 159.1 ± 7.6 *** | p ≤ 0.001 |
| BMI (kg/m2) | 18.65 ± 2.21 † | 17.07 ± 1.34 | 19.66 ± 2.18 ††† | 19.02 ± 2.13 † | 19.62 ± 2.75 ††† | p ≤ 0.001 |
| Underweight ‡ (n, %) | 7 (14.0%) | 12 (28.6%) | 2 (3.1%) | 1 (4.5%) | 6 (6.7%) | p ≤ 0.001 |
| Normoweight ‡ (n, %) | 40 (80.0%) | 30 (71.4%) | 61 (93.8%) | 21 (95.5%) | 74 (82.2%) | |
| Overweight ‡ (n, %) | 3 (6.0%) | 0 (0.0%) | 2 (3.1%) | 0 (0.0%) | 10 (11.1%) |
| n | Low Adherence (KIDMED ≤ 3) | Moderate Adherence (KIDMED 4–7) | High Adherence (KIDMED ≥ 8) | Significance | ||
|---|---|---|---|---|---|---|
| Body weight (kg) | 269 | 51.76 ± 7.56 | 48.07 ± 9.16 | 45.31 ± 8.11 | p = 0.002 * | |
| BMI (kg/m2) | 269 | 19.88 ± 1.96 | 19.22 ± 2.71 | 18.43 ± 1.98 | p = 0.009 * | |
| Weight status | Underweight | 28 | 0 (0.0%) | 18 (64.3%) | 10 (35.7%) | p = 0.035 |
| Normoweight | 226 | 22 (9.7%) | 121 (53.5%) | 83 (36.7%) | ||
| Overweight | 15 | 2 (13.3%) | 12 (80.0%) | 1 (6.7%) | ||
| Sport discipline | Artistic gymnastics | 50 | 4 (8.0%) | 27 (54.0%) | 19 (38.0%) | p = 0.504 |
| Rhythmic gymnastics | 42 | 0 (0.0%) | 26 (61.9%) | 16 (38.1%) | ||
| Trampoline/tumbling | 65 | 6 (9.2%) | 40 (61.5%) | 19 (29.2%) | ||
| Acrobatics/aerobics | 22 | 3 (13.6%) | 11 (50.0%) | 8 (36.4%) | ||
| Gymnastics for all | 90 | 11 (12.2%) | 47 (52.2%) | 32 (35.6%) | ||
| Competition level | International | 54 | 5 (9.3%) | 29 (53.7%) | 20 (37.0%) | p = 0.849 |
| National | 134 | 10 (7.5%) | 70 (59.0%) | 45 (33.6%) | ||
| Regional | 79 | 9 (11.4%) | 42 (53.2%) | 28 (35.4%) | ||
| Weekly training frequency | ≥5 times | 134 | 7 (5.2%) | 77 (57.5%) | 50 (37.3%) | p = 0.065 |
| 3–4 times | 92 | 12 (13.0%) | 55 (59.8%) | 25 (27.2%) | ||
| 1–2 times | 42 | 5 (11.9%) | 18 (42.9%) | 19 (45.2%) | ||
| 95% CI | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Constant | B | SE | β | t | p | Lower | Upper | ||
| Model 1 | KIDMED (all athletes) | 20.77 | −0.27 | 0.07 | −0.24 | −4.03 | <0.001 | −0.41 | −0.14 |
| Model 2 | KIDMED (exclude overweight) | 19.97 | −0.19 | 0.06 | −0.2 | −3.2 | 0.002 | −0.31 | −0.07 |
| Model 3 | KIDMED (exclude underweight) | 20.94 | −0.25 | 0.07 | −0.24 | −3.74 | <0.001 | −0.38 | −0.12 |
| Model 4 | KIDMED (only normoweight) | 20.15 | −0.17 | 0.06 | −0.19 | −2.97 | 0.003 | −0.29 | −0.06 |
| KIDMED Questions | Answers | Statistics | ||
|---|---|---|---|---|
| Yes | No | t | Significance | |
| Takes a fruit or fruit juice every day | 18.9 ± 2.5 | 19.6 ± 1.8 | 1.54 | p = 0.124 |
| Has a second fruit every day | 18.7 ± 2.4 | 19.3 ± 2.5 | 2.03 | p = 0.043 |
| Has fresh/cooked vegetables regularly once/day | 19 ± 2.4 | 19.1 ± 2.5 | 0.35 | p = 0.725 |
| Has fresh/cooked vegetables ≥once/day | 18.6 ± 2.3 | 19.2 ± 2.5 | 1.60 | p = 0.110 |
| Consumes fish regularly (≥2–3 times/week) | 18.7 ± 2 | 19.1 ± 2.6 | 1.24 | p = 0.213 |
| Goes ≥once/week to a fast-food restaurant | 20.1 ± 2.6 | 18.7 ± 2.4 | 3.67 | p = 0.000 |
| Likes pulses and eats them ≥once/week | 18.8 ± 2.2 | 19.3 ± 2.8 | 1.60 | p = 0.110 |
| Consumes pasta/rice almost every day (≥5 times/week) | 18.8 ± 2.3 | 19.3 ± 2.6 | 1.71 | p = 0.088 |
| Has cereals or grains (bread, etc.) for breakfast | 19 ± 2.5 | 19 ± 2.4 | −0.14 | p = 0.884 |
| Consumes nuts regularly (≥2–3 times/week) | 18.4 ± 2.3 | 19.5 ± 2.5 | 3.65 | p = 0.000 |
| Uses olive oil at home | 19 ± 2.4 | 18.6 ± 2.8 | −0.70 | p = 0.481 |
| Skips breakfast | 19.6 ± 2.7 | 18.8 ± 2.3 | 2.56 | p = 0.011 |
| Has a dairy product for breakfast (yoghurt, milk, etc.) | 19 ± 2.5 | 18.9 ± 2.3 | −0.42 | p = 0.672 |
| Has commercially baked goods or pastries for breakfast | 18.8 ± 2.2 | 19 ± 2.5 | −0.49 | p = 0.621 |
| Takes two yoghurts and/or some cheese (40 g) daily | 19 ± 2.5 | 19 ± 2.5 | −0.23 | p = 0.816 |
| Takes sweets and candy several times every day | 19.2 ± 2.5 | 18.9 ± 2.4 | 0.80 | p = 0.424 |
| 95% CI | ||||||||
|---|---|---|---|---|---|---|---|---|
| Components of the Analysis | Answer | B | SE | β | t | p | Lower | Upper |
| Eating a second fruit every day | No | Reference category | ||||||
| Yes | −0.167 | 0.304 | −0.034 | −0.548 | 0.584 | −0.765 | 0.432 | |
| Consuming nuts at least 2–3 times/week | No | Reference category | ||||||
| Yes | −0.83 | 0.305 | −0.168 | −2.723 | 0.007 | −1.431 | −0.23 | |
| Eating fast-food more than once a week | Yes | Reference category | ||||||
| No | −1.159 | 0.373 | −0.184 | −3.106 | 0.002 | −1.893 | −0.424 | |
| Skipping breakfast | Yes | Reference category | ||||||
| No | −0.625 | −0.329 | −0.114 | −1.901 | 0.058 | −1.272 | 0.022 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontele, I.; Grammatikopoulou, M.G.; Vassilakou, T. Level of Adherence to the Mediterranean Diet and Weight Status among Adolescent Female Gymnasts: A Cross-Sectional Study. Children 2021, 8, 1135. https://doi.org/10.3390/children8121135
Kontele I, Grammatikopoulou MG, Vassilakou T. Level of Adherence to the Mediterranean Diet and Weight Status among Adolescent Female Gymnasts: A Cross-Sectional Study. Children. 2021; 8(12):1135. https://doi.org/10.3390/children8121135
Chicago/Turabian StyleKontele, Ioanna, Maria G. Grammatikopoulou, and Tonia Vassilakou. 2021. "Level of Adherence to the Mediterranean Diet and Weight Status among Adolescent Female Gymnasts: A Cross-Sectional Study" Children 8, no. 12: 1135. https://doi.org/10.3390/children8121135
APA StyleKontele, I., Grammatikopoulou, M. G., & Vassilakou, T. (2021). Level of Adherence to the Mediterranean Diet and Weight Status among Adolescent Female Gymnasts: A Cross-Sectional Study. Children, 8(12), 1135. https://doi.org/10.3390/children8121135