
Anxiety Reduction and Improved Concentration in Schoolchildren through Wingwave® Coaching


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
2.3. Procedure
3. Results
3.1. Multivariate Results
3.2. Post Hoc Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, C.A.; Lazarus, R.S. Emotion and adaption. In Handbook of Personality: Theory and Research, 1st ed.; Pervin, L.A., Ed.; Guilford: New York, NY, USA, 1990; pp. 609–637. [Google Scholar]
- De Corte, E.; Depaepe, F.; Op’t Eynde, P.; Verschaffel, L. Students’ self-regulation of emotions in mathematics: An analysis of meta-emotional knowledge and skills. ZDM Int. J. Math. Educ. 2011, 43, 483–495. [Google Scholar] [CrossRef]
- Schutz, P.A.; Distefano, C.; Benson, J.; Davis, H.A. The emotional regulation during test-taking scale. Anxiety Stress Coping Int. J. 2004, 17, 253–269. [Google Scholar] [CrossRef]
- Chen, R.; Gillespie, A.; Zhao, Y.; Xi, Y.; Ren, Y.; McLean, L. The efficacy of eye movement desensitization and reprocessing in children and adults who have experienced complex childhood trauma: A systematic review of randomized controlled trials. Front. Psychol. 2018, 9, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, G.; Farrell, D.; Barron, I.; Hutchins, J.; Whybrow, D.; Kiernan, M.D. The use of eye-movement desensitization reprocessing (EMDR): Therapy in treating post-traumatic stress disorder—A systematic narrative review. Front. Psychol. 2018, 9, 923. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-R.; Hung, K.-W.; Tsai, J.-C.; Chu, H.; Chung, M.-H.; Chen, S.-R.; Liao, Y.-M.; Ou, K.-L.; Chang, Y.-C.; Chou, K.-R. Efficacy of eye-movement desensitization and reprocessing for patients with posttraumatic-stress disorder: A meta-analysis of randomized controlled trials. PLoS ONE 2014, 9, e103676. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, F. Eye Movement and Desensitization (EMDR) Therapy, 3rd ed.; Guilford: New York, NY, USA, 2018. [Google Scholar]
- Shapiro, F. Eye movement desensitization: A new treatment for post-traumatic stress disorder. J. Behav. Ther. Exp. Psychiatry 1989, 20, 211–217. [Google Scholar] [CrossRef]
- Shapiro, F.; Maxfield, L. Eye Movement Desensitization and Reprocessing (EMDR): Information Processing in the Treatment of Trauma. J. Clin. Psychol. 2002, 58, 933–946. [Google Scholar] [CrossRef]
- Landin-Romero, R.; Moreno-Alcazar, A.; Pagani, M.; Amann, B.L. How does eye movement desensitization and reprocessing therapy work? A systematic review on suggested mechanisms of action. Front. Psychol. 2018, 9, 1395. [Google Scholar] [CrossRef]
- Horst, F.; Den Oudsten, B.; Zijlstra, W.; de Jongh, A.; Lobbestael, J.; De Vries, J. Cognitive behavioral therapy vs. eye movement desensitization and reprocessing for treating panic disorder: A randomized controlled trial. Front. Psychol. 2017, 8, 1409. [Google Scholar] [CrossRef] [Green Version]
- Benor, D.; Rossiter-Thornton, J.; Toussaint, L. A randomized, controlled trial of wholistic hybrid derived from eye movement desensitization and reprocessing and emotional freedom technique (WHEE) for self-treatment of pain, depression, and anxiety in chronic pain patients. J. Evid.-Based Complementary Altern. Med. 2017, 22, 268–277. [Google Scholar] [CrossRef]
- Shapiro, F.; Maxfield, L. In the blink of an eye. Psychologist 2002, 15, 120–124. [Google Scholar]
- Lee, C.W.; Cuijpers, P. A meta-analysis of the contribution of eye movements in processing emotional memories. J. Behav. Ther. Exp. Psychiatry 2013, 44, 231–239. [Google Scholar] [CrossRef] [Green Version]
- De Voogd, L.D.; Kanen, J.W.; Neville, D.A.; Roelofs, K.; Fernández, G.; Hermans, E.J. Eye-movement intervention enhances extinction via amygdala deactivation. J. Neurosci. 2018, 38, 8694–8706. [Google Scholar] [CrossRef]
- Bisson, J.I.; Roberts, N.P.; Andrew, M.; Cooper, R.; Lewis, C. Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst. Rev. 2013, 12, CD003388. [Google Scholar] [CrossRef]
- American Psychiatric Association. Eye Movement Desensitization and Reprocessing (EMDR) Therapy 2017. Washington, DC. Available online: https://www.apa.org/ptsd-guideline/treatments/eye-movement-reprocessing (accessed on 13 September 2021).
- Rodenburg, R.; Benjamin, A.; de Roos, C.; Meijer, A.M.; Stams, G.J. Efficacy of EMDR in children: A meta-analysis. Clin. Psychol. Rev. 2009, 29, 599–606. [Google Scholar] [CrossRef]
- Maxfield, L.; Melnyk, W.T. Single session treatment of test anxiety with eye movement desensitization and reprocessing (EMDR). Int. J. Stress Manag. 2000, 7, 87–101. [Google Scholar] [CrossRef]
- Foster, S.; Lendl, J. Eye movement desensitization and reprocessing: Four case studies of a new tool for executive coaching and restoring employee performance after setbacks. Consult. Psychol. J. Pract. Res. 1996, 48, 155–161. [Google Scholar] [CrossRef]
- Falls, N.; Barker, J.B.; Turner, M.J. The effects of eye movement desensitization and reprocessing on prospective imagery and anxiety in golfers. J. Appl. Sport Psychol. 2018, 30, 171–184. [Google Scholar] [CrossRef]
- Brooker, E. Music performance anxiety: A clinical outcome study into the effects of cognitive hypnotherapy and eye movement desensitization and reprocessing in advanced pianists. Psychol. Music. 2018, 46, 107–124. [Google Scholar] [CrossRef]
- Vauthier, M.; Paquet, Y.; Krumm, C.-M.; Tarquinio, C. Vers une nouvelle appréhension des mathématiques par traitement EMDR: Actualités et perspectives. [Towards a new understanding of mathematics through Eyes Movement Desensitization and Reprocessing: News and perspectives.] Psychol. Française 2019, 64, 295–304. [Google Scholar] [CrossRef]
- Besser-Siegmund, C.; Siegmund, L.; Siegmund, H. Wingwave® Coaching. Like the Beat of a Butterfly’s Wings, 1st ed.; Junfermann: Paderborn, Germany, 2020. [Google Scholar]
- Omura, Y. A new, simple, non-invasive imaging technique of internal organs and various cancer tissues using extended principles of the “Bi-Digital O-Ring Test” without using expensive imaging instruments or exposing the patient to any undesirable radiation. Acupunct. Electro-Ther. Res. 1985, 10, 255–277. [Google Scholar] [CrossRef]
- Lu, D.P.; Lu, G.P.; Lu, W.I. Anxiety control of dental patients by clinical combination of acupuncture, Bi-Digital O-Ring Test, and eye movement desensitization with sedation via submucosal route. Acupunct. Electro-Ther. Res. 2007, 32, 15–30. [Google Scholar] [CrossRef]
- Lu, D.P.; Wu, P.-S.; Lu, W. Sedating Pediatric Dental Patients by Oral Ketamine with Alternating Bi-lateral Stimulation of Eye Movement Desensitization and minimizing Adverse Reaction of Ketamine by Acupuncture and Bi-Digital O-Ring Test. Acupunct. Electro-Ther. Res. 2012, 37, 103–123. [Google Scholar] [CrossRef]
- Rathschlag, M.; Memmert, D. The influence of self-generated emotions on physical performance: An investigation of happiness, anger, anxiety, and sadness. J. Sport Exerc. Psychol. 2013, 35, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Rathschlag, M.; Memmert, D. Reducing anxiety and enhancing physical performance by using an advanced version of EMDR: A pilot study. Brain Behav. 2014, 4, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Koetter, T.; Niebuhr, F. Resource-oriented coaching for reduction of examination-related stress in medical students: An exploratory randomised controlled trial. Adv. Med. Educ. Pract. 2016, 7, 497–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naumenko, K.; Steinhaeuser, J.; Niebuhr, F.; Goetz, K. Short report: Coaching as an intervention to treat mild form of fear of flying. Psychol. Health Med. 2020, 4, 1–8. [Google Scholar] [CrossRef]
- Dalbert, C.; Stöber, J. Forschung zur Schuelerpersoenlichkeit [Research on students‘ personality]. In Handbuch der Schulforschung, 1st ed.; Helsper, W., Böhme, J., Eds.; vs. Verlag fuer Sozialwissenschaften: Wiesbaden, Germany, 2004; pp. 881–902. [Google Scholar]
- Donat, M.; Gallschütz, C.; Dalbert, C. The relation between students’ justice experiences and their school refusal behavior. Soc. Psychol. Educ. Int. J. 2018, 21, 447–475. [Google Scholar] [CrossRef]
- Yamamoto, K. Children’s ratings of the stressfulness of experience. Dev. Psychol. 1979, 15, 581–582. [Google Scholar] [CrossRef]
- Nitkowski, D.; Lohbeck, A.; Petermann, U.; Petermann, F. Hat die Angstauspraegung bei Kindern und Jugendlichen in Deutschland von 1974 bis 2016 zugenommen? Eine Analyse des saekularen Trends von Angst ueber eine Zeitspanne von 42 Jahren. [Did the level of anxiety among children and adolescents in Germany increase between 1974 and 2016? An analysis of the secular trend in fear over a 42-year period.]. Kindh. Entwickl. 2017, 26, 110–117. [Google Scholar]
- Wieczerkowski, W.; Nickel, H.; Janowski, A.; Fittkau, B.; Rauer, W.; Petermann, F. Angstfragebogen fuer Schueler (AFS) [Anxiety Questionnaire for Students], 1st ed.; Hogrefe: Goettingen, Germany, 2016. [Google Scholar]
- Dueker, H.; Lienert, G.A. Konzentrations-Leistungs-Test–Revidierte Fassung [Concentration Performance Test–Revised Version], 1st ed.; Hogrefe: Goettingen, Germany, 2001. [Google Scholar]
- Rousseau, P.-F.; El Khoury-Malhame, M.; Reynaud, E.; Boukezzi, S.; Cancel, A.; Zendjidjian, X.; Guyon, V.; Samuelian, J.-C.; Guedj, E.; Chaminade, T.; et al. Fear extinction learning improvement in PTSD after EMDR therapy: An fMRI study. Eur. J. Psychotraumatol. 2019, 10, 1568132. [Google Scholar] [CrossRef] [Green Version]
- Lewey, J.H.; Smith, C.L.; Burcham, B.; Saunders, N.L.; Elfallal, D.; O’Toole, S.K. Comparing the effectiveness of EMDR and TF-CBT for children and adolescents: A meta-analysis. J. Child Adolesc. Trauma 2018, 11, 457–472. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Effect | F | df | p | η2 | ε | |
|---|---|---|---|---|---|---|
| KLT-R total answers | group | 0.35 | 1, 51 | 0.556 | - | - |
| time | 16.47 | 1.63, 83.09 | <0.001 | 0.24 | 0.82 | |
| group * time | 1.15 | 1.63, 83.09 | 0.310 | - | 0.82 | |
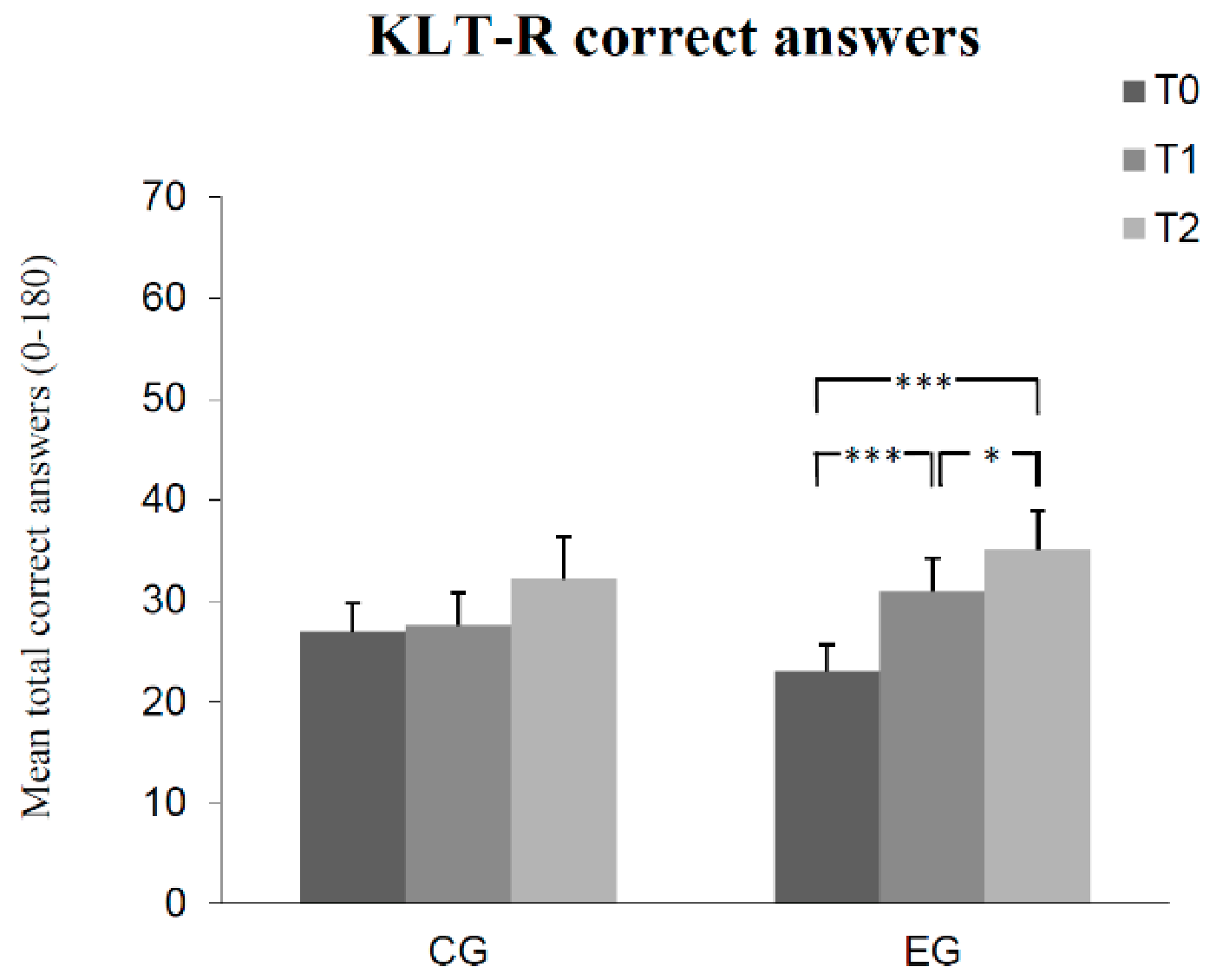
| KLT-R correct answers | group | 0.03 | 1, 51 | 0.871 | - | - |
| time | 17.15 | 1.49, 76.10 | <0.001 | 0.25 | 0.75 | |
| group * time | 3.72 | 1.49, 76.10 | 0.041 | 0.07 | 0.75 | |
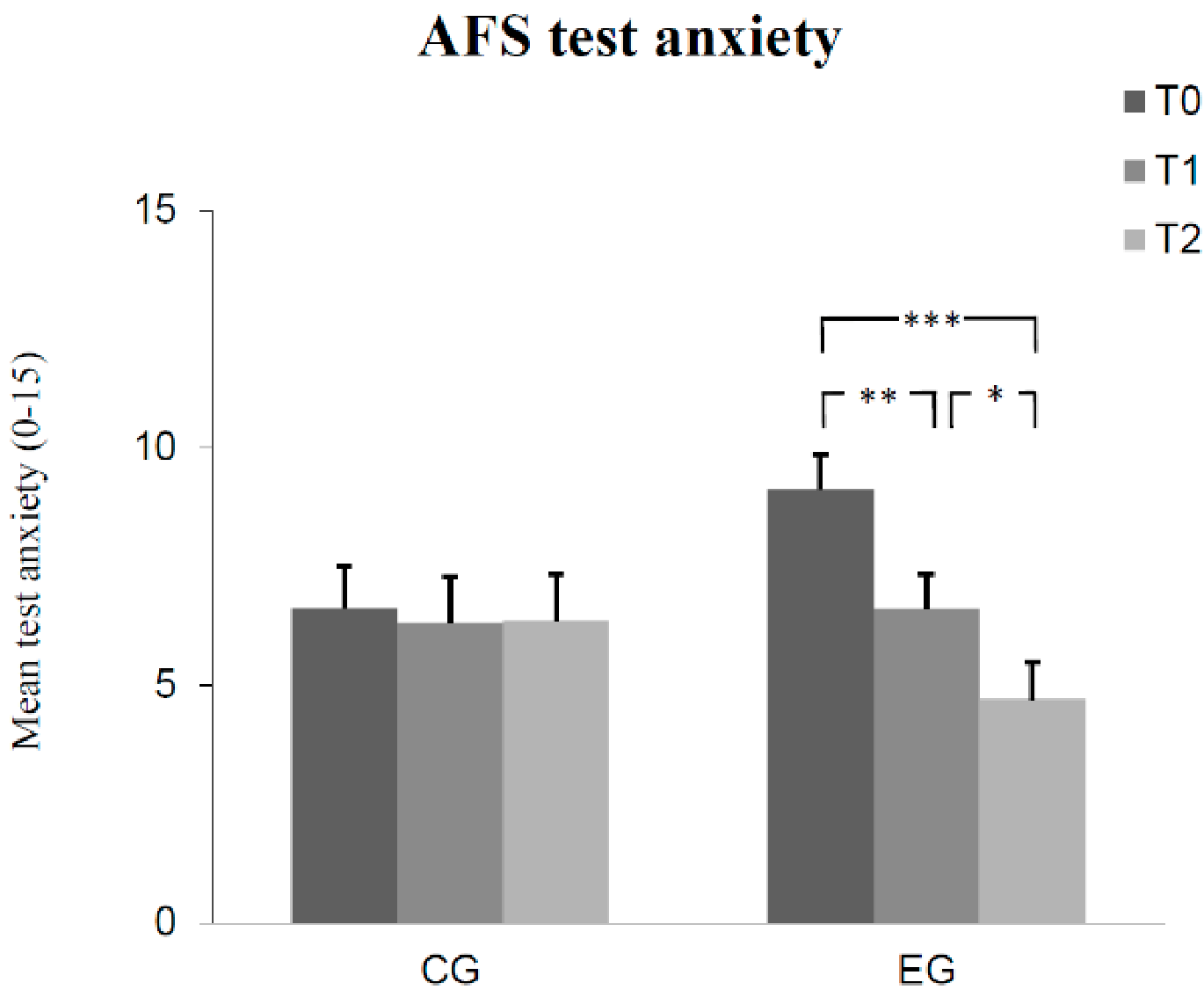
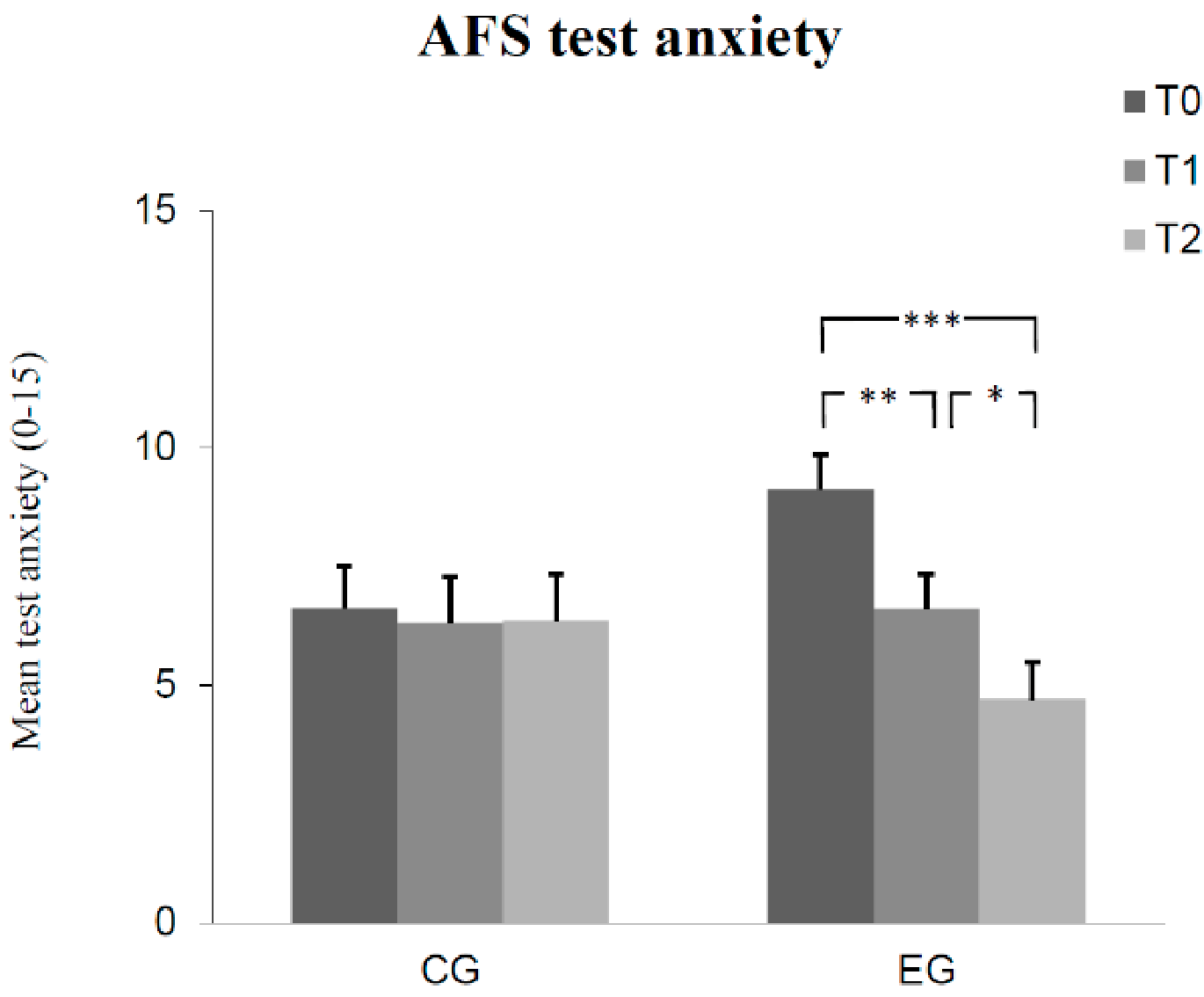
| AFS test anxiety | group | 0.13 | 1, 51 | 0.716 | - | - |
| time | 12.98 | 2, 102 | <0.001 | 0.20 | - | |
| group * time | 10.12 | 2, 102 | <0.001 | 0.17 | - | |
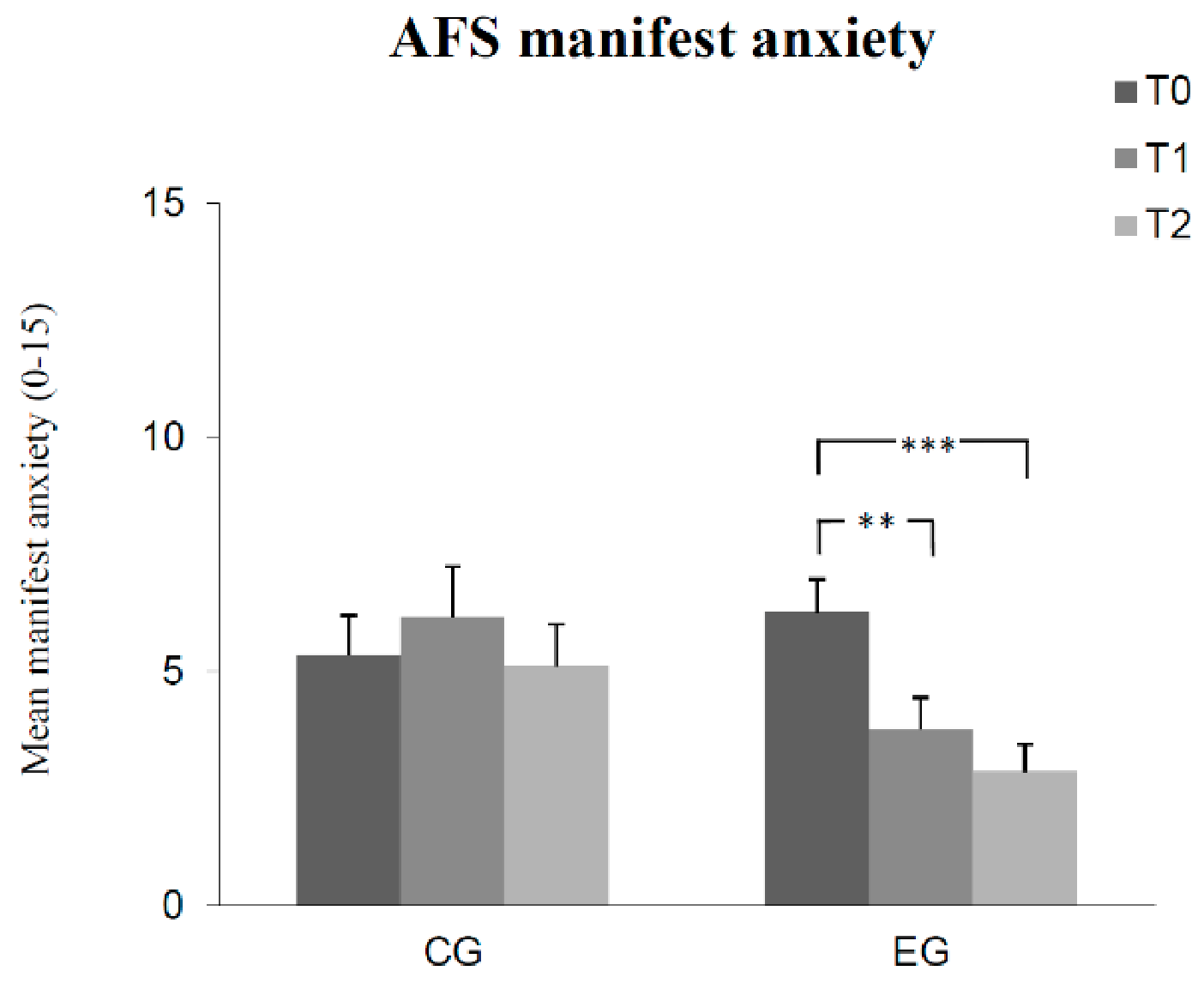
| AFS manifested anxiety | group | 1.54 | 1, 51 | 0.221 | - | - |
| time | 10.27 | 2, 102 | <0.001 | 0.17 | - | |
| group * time | 11.08 | 2, 102 | <0.001 | 0.18 | - | |
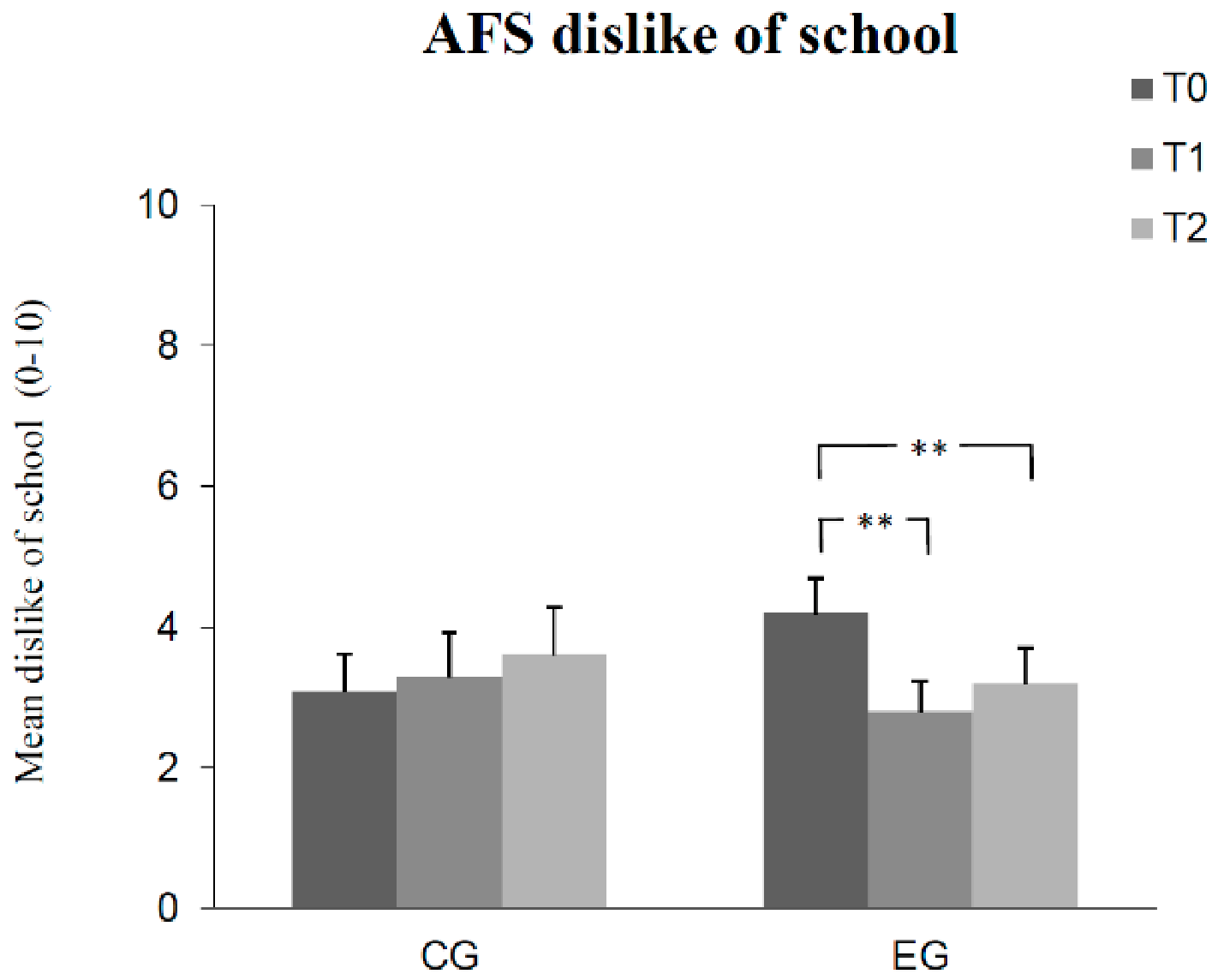
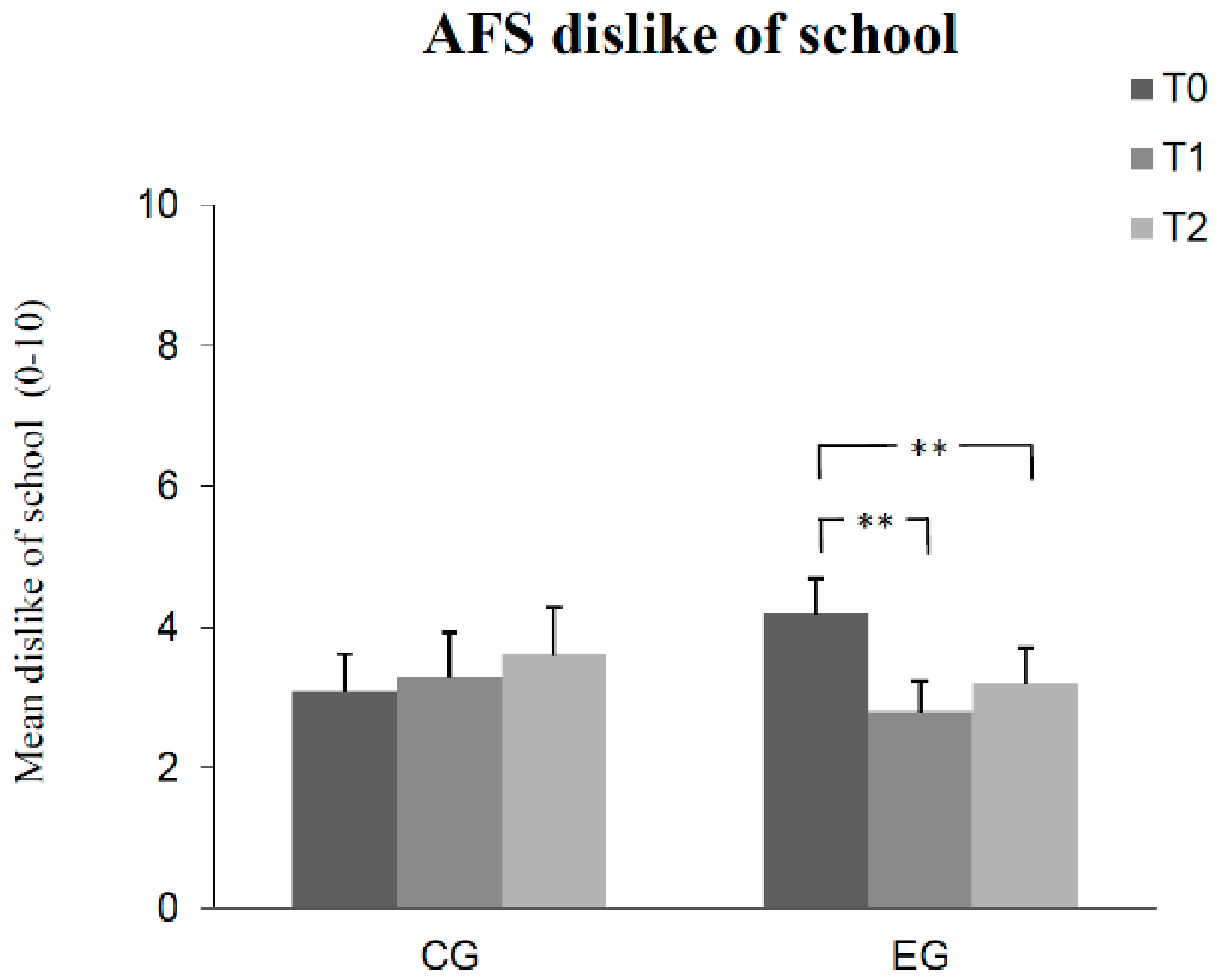
| AFS dislike of school | group | 0.01 | 1, 51 | 0.924 | - | - |
| time | 2.35 | 2, 102 | 0.100 | - | - | |
| group * time | 5.48 | 2, 102 | 0.006 | 0.10 | - | |
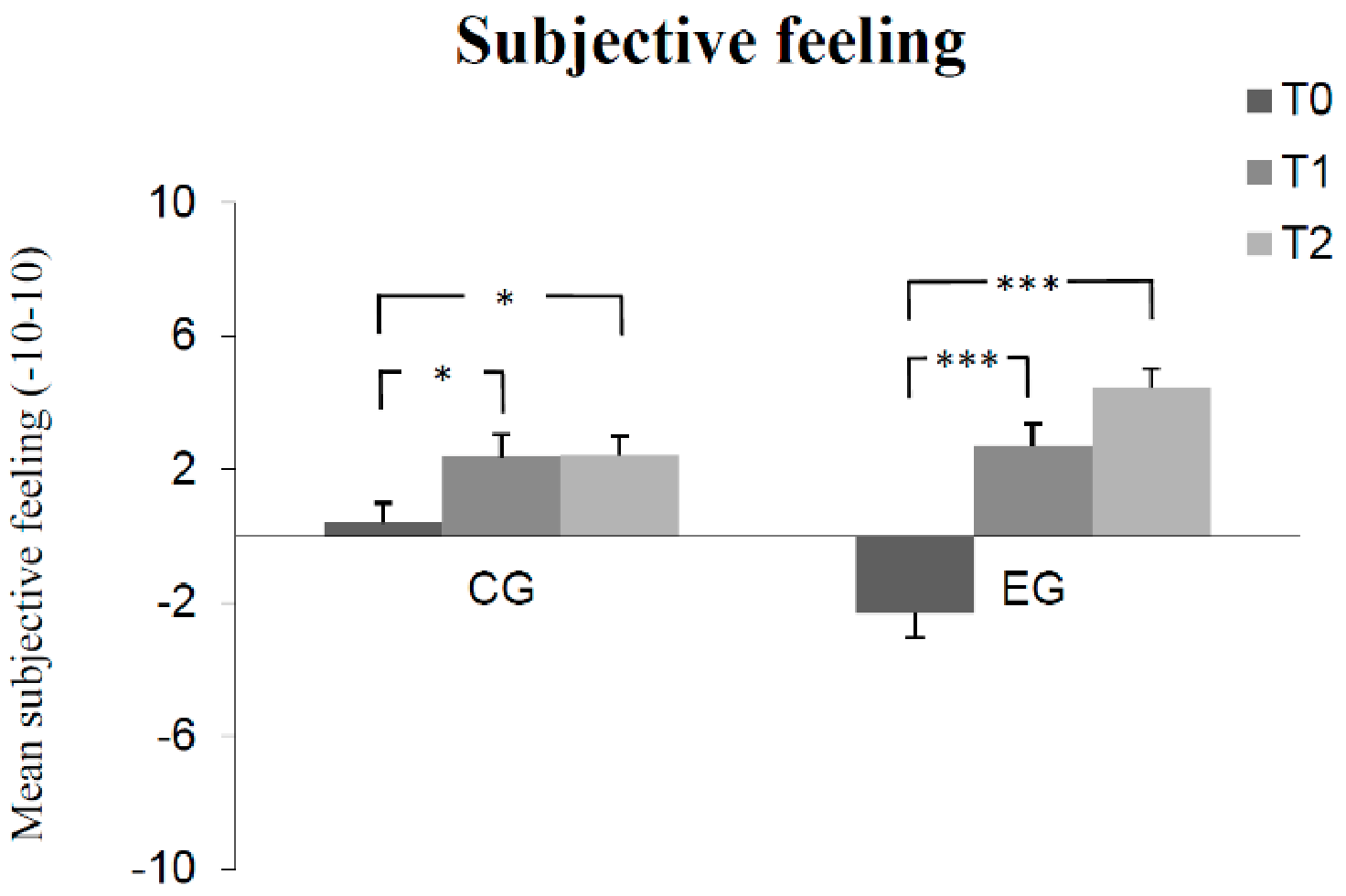
| Subjective feeling | group | 0.03 | 1, 51 | 0.868 | - | - |
| time | 44.99 | 2, 102 | <0.001 | 0.47 | - | |
| group * time | 12.05 | 2, 102 | <0.001 | 0.19 | - |
| Time of Measurement | ||||||
|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Retention Test | ||||
| Mean | SD | Mean | SD | Mean | SD | |
| KLT-R total answers | ||||||
| Experimental group | 32.37 | 14.78 | 38.60 | 18.72 | 43.43 | 21.41 |
| Control group | 37.78 | 14.57 | 41.09 | 21.16 | 44.26 | 21.33 |
| KLT-R correct answers | ||||||
| Experimental group | 23.00 | 14.83 | 30.93 | 18.01 | 35.13 | 20.79 |
| Control group | 26.96 | 13.43 | 27.61 | 15.36 | 32.30 | 19.89 |
| AFS test anxiety | ||||||
| Experimental group | 9.13 | 3.98 | 6.60 | 4.07 | 4.70 | 4.28 |
| Control group | 6.61 | 4.25 | 6.30 | 4.70 | 6.35 | 4.74 |
| AFS manifested anxiety | ||||||
| Experimental group | 6.27 | 3.86 | 3.77 | 3.65 | 2.87 | 3.17 |
| Control group | 5.35 | 4.09 | 6.17 | 5.16 | 5.13 | 4.22 |
| AFS dislike of school | ||||||
| Experimental group | 4.20 | 2.72 | 2.80 | 2.38 | 3.20 | 2.75 |
| Control group | 3.09 | 2.52 | 3.30 | 2.99 | 3.61 | 3.24 |
| Subjective feeling | ||||||
| Experimental group | −2.32 | 3.34 | 2.70 | 4.08 | 4.45 | 4.00 |
| Control group | 0.41 | 3.65 | 2.39 | 3.17 | 2.43 | 2.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiland, F.P.G.; Rathschlag, M.; Klatt, S. Anxiety Reduction and Improved Concentration in Schoolchildren through Wingwave® Coaching. Children 2021, 8, 1102. https://doi.org/10.3390/children8121102
Weiland FPG, Rathschlag M, Klatt S. Anxiety Reduction and Improved Concentration in Schoolchildren through Wingwave® Coaching. Children. 2021; 8(12):1102. https://doi.org/10.3390/children8121102
Chicago/Turabian StyleWeiland, Frank P. G., Marco Rathschlag, and Stefanie Klatt. 2021. "Anxiety Reduction and Improved Concentration in Schoolchildren through Wingwave® Coaching" Children 8, no. 12: 1102. https://doi.org/10.3390/children8121102
APA StyleWeiland, F. P. G., Rathschlag, M., & Klatt, S. (2021). Anxiety Reduction and Improved Concentration in Schoolchildren through Wingwave® Coaching. Children, 8(12), 1102. https://doi.org/10.3390/children8121102