
A Qualitative Exploration of the Referral Process of Children with Common Infections from Private Low-Level Health Facilities in Western Uganda

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design and Setting
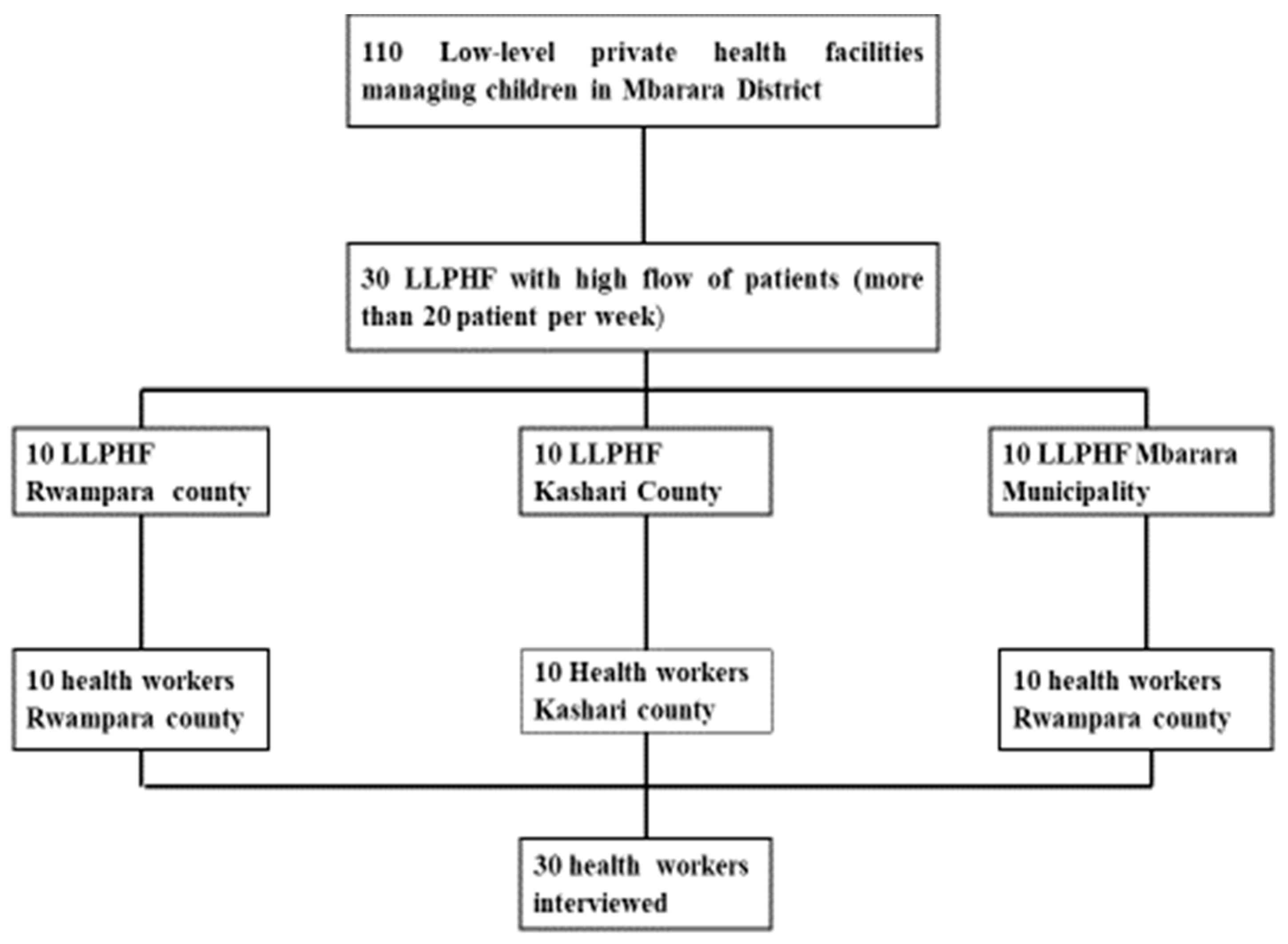
2.2. Sampling and Recruitment
- They were used at an LLPHF; and
- Had been providing clinical care for children in a private facility for at least 6 months.
2.3. Data Collection
2.4. Analytical Process
2.5. Ethical Approval
3. Results
3.1. Demographics Characteristics of Study Participants
3.2. Overarching Themes
3.2.1. Reasons for Referral
“In most cases, like in neonates, you find that the child has difficulty breathing, and we don’t have an oxygen cylinder or concentrator…. Another reason is that the child may have HIV, in addition to malaria or pneumonia, and is in critical condition, and you need to refer because the child needs additional support and treatment of HIV.” (HW1, male nurse, Mbarara Municipality)
“The health worker did not know the exact diagnosis for the child and did not have the treatment as well. She checked for malaria, which was negative, and told me that she did not have any other medication apart from Coartem (malaria medicine) and cough medicines. She told me to take the child to experts.” (CT1, mother of a child with a fever)
“If it is [a] simple condition that we can manage but the caretaker cannot afford the payment, then I refer such patients.” (HW2, male clinical officer, Mbarara Municipality)
“Sometimes we provide the services and even give transport to severely ill patients because you do not want the child to die from your clinic.” (HW3, female nursing assistant, Rwampara)
3.2.2. Process of Referral: Person Responsible, Where to Refer and How Are Referrals Done
“Each and every patient who comes, I have to let the doctor know about the condition wherever he is. I don’t tamper with them; he tells me every step to take, how the prognosis is and then comes to review them if possible, then refers them.” (HW4, female nurse, Kashari)
“The owner of the clinic determines the referrals. When I get complicated cases, I consult her first, so she is the decision maker.” (HW5, female nurse, Rwampara)
“I prefer referring to Mbarara Regional Referral Hospital (MRRH) because when they receive a referral, they attend to it immediately….” (HW6, female nurse, Rwampara)
“Mbarara is a regional referral facility and has many patients and is overcrowded. When you refer the patient there, they may not go. It’s not that they are not delivering services, but the number of health workers is very small compared to the patients.” (HW1, male nurse, Mbarara Municipality)
“As a medical officer without specialisation, sometimes I refer to a specialist physician in another private clinic. I look at it at that level, and there you get good feedback; you learn from the case, and the patient gets helped. But if you send someone in the referral hospital (MRRH), immediately they attend to the patient, but you never get feedback.” (HW7, male doctor, Mbarara Municipality)
“We usually write referral notes and the treatment if the patient has been here, but in most cases, if we have not touched the patient and have not given any medication yet, we tell them verbally to go. If he has been our client, we write everything we have done and refer.” (HW1, male nurse, Mbarara Municipality)
“They bring you physically with the health worker, who leaves after handing you over, and they have initiated treatment.” (CT2, 32-year-old mother of a newborn infant)
3.2.3. Attitudes of the Health Workers about Referring Patients
“If you make a call and they say the child is improving, of course you feel good; you say my referral is of advantage now.” (HW8, female nurse, Mbarara Municipality).
“Referring cases I cannot handle creates for me confidence and trust from the public because I direct them where they can get proper management. When I get the chance and see the treatment that the child was given or the diagnosis that was made, I learn from it, and next time if I get a similar condition, I treat according to what I have observed.” (HW9, male nurse, Mbarara Municipality).
“You don’t feel good to refer, because it’s a private clinic, and when you refer, they may think you are unable to deliver services very well. People outside may think that you are incompetent.” (HW4, female nurse, Rwampara).
3.2.4. Challenges to the Referral Process
- Non-adherence to referral instructions by the caretakers
- Loss of revenue to the clinic
- Lack of feedback concerning the referral from referral facilities
“The main problem is most of the caretakers are unable to find money for transport fare when I refer them to the Mbarara or Itojo hospital; they instead go to another private facility around…” (HW10, female nurse, Rwampara)
“The health worker referred us to Mbarara (hospital), but we instead went to Kobi, a health facility in our neighbourhood and easy for us to access… we were told the child had no blood, and he died from there.” (CT3, 29-year-old mother who did not comply with the referral)
“At the children’s hospital where the doctor had referred us, they cared for the patients well, but we left that hospital because the medical bills were high and we did not have enough money.” (CT4, 26-year-old father of child with fever and convulsions)
“They told me to go to the MRRH, that big hospital; I did not go there, because the child improved when we got the treatment… so since I saw he (child) was ok (improved), I decided not to bother myself.” (CT5, 23-year-old mother of a child with pneumonia)
“When we refer them, they feel like we have done nothing for their children. They resist paying us for the care received before referral, because they believe we have failed.” (HW11, male nurse, Mbarara Municipality)
“They (the referral health facility) are supposed to fill what was done on the form at the time of discharge so that if the patient comes back, you get to know what was done. But we never get any feedback….” (HW7, male doctor, Mbarara Municipality)
3.2.5. Experiences of Caregivers during the Referral Process
- Incurring high costs for transport, medical care and feeding
- Difficulty in accessing transport
- Overcrowding on the ward spaces
- Unfriendly health facility staff
- Delays in accessing care
- Possibility for the child to receive appropriate care
- Caring health workers
- Not having to pay for medical care
“Here, the expenditures are high because I had to pay for the scan and blood investigations. I no longer have any money to even buy food.” (CT6, 45-year-old grandmother of a newborn, at a public hospital)
“I could not afford to buy a full dose of treatment for the baby, because I came expecting free services and now I have to pay….” (CT7, father of a 6-month-old with pneumonia, at a public hospital)
“They told me that the ambulance would cost UGX 70,000 (USD 19), and I only had UGX 10,000, so I took a bodaboda (taxi motorbike) that left me on the main road….” (CT8, 50-year-old grandmother of a newborn)
“…. the roads from our place have not been worked on; they have stones, so reaching here with the patient is a hard process.” (CT6, 45-year-old grandmother of a newborn)
“The clinic doctor said the child was badly off because the cold wind affected her, and she got pneumonia. Now we had to again take the same child on a bodaboda. She was going to get worse….” (CT9, 25-year-old father of a child with pneumonia)
“They work from very small rooms congested with patients and machines. There is even no space for the one who is weighing the babies. You just peep through the glass to see if the doctor has finished seeing the baby.” (CT10, 25-year-old mother of a child with pneumonia, in a public hospital)
“The medical personnel need to learn how to speak properly to the patients… I am already shuttered with [my] child’s sickness, so if you just shout at me, I don’t feel good.” (CT10, 25-year-old mother of a child with pneumonia)
“What annoyed us are the cleaning staff at the hospital, who abused us and poured water on us while we were sleeping….” (CT6, 45-year-old grandmother in a public hospital)
“I did not find a conducive situation for receiving very sick children at the main referral hospital. My husband wasn’t happy with the way they were not minding about us, and as a parent, you panic thinking that the child might die, so he decided to go to Holy Innocents (a private children’s hospital)…” (CT10, 25-year-old mother of a child with pneumonia)
“We spent a long time at the laboratory. I reached there at 9:00 am or 9:30 am and left at 12 midday. The laboratory personnel were not busy but were concentrating on their phones…” (CT11, mother of a child with fever)
“At the other clinic, we had spent 3 days, but the child’s condition was worsening…but when we reached the [Mbarara] Regional Referral Hospital, they quickly helped us; they put her on oxygen, checked her blood to confirm the disease and later gave her treatment through the cannula which they put on the hand.” (CT12, 36-year-old father of a child with pneumonia)
“At the regional hospital, the health workers cared for my baby a lot. As a parent, I could not understand what the health workers were doing, but you could see them moving here and there, doing this and that, explaining to me why they are doing somethings, assuring me that the baby will be fine. I could see the baby cry, and I thought she had pain when they put the feeding tube, but they explained to me that in her condition, she should not be on empty stomach. They were giving us psychological care and making sure we understood what was going on.” (CT7, father of a 6-month-old baby with pneumonia)
3.2.6. Views on How to Improve the Referral Process from LLPHFs
- Reduce the waiting time
- Improve transportation
- Reduce costs incurred during the referral process
- Improve communication
“The government needs to add more doctors because what I saw there was too much; there were very many sick children and only two doctors. This is the reason why we were not worked on quickly. At least, they should be four doctors.” (CT5, 25-year-old mother of a child with pneumonia, at a public hospital)
“Private clinics should employ enough staff so that the referred child is accompanied by a nurse regardless of whether there is an ambulance or not and handed over to staff at the referral facility.” (HW12, male clinical officer, Kashari)
“Another thing that should be improved is the way we are referred…usually in the clinics, they perform the first tests and so know how the child is. I may not know how to explain this result when I reach the hospital, so it is better if it is written down….” (CT9, 25-year-old father of a child with pneumonia)
“Even though some things are not available, they (government) need to get for us ambulances….” (CT12, 36-year-old father)
“If those bigger facilities could put in place ambulances at a cost that is affordable and even collaborate with the health facilities around…. when you get a condition to refer here, then we contact them.” (HW10, female nurse, Rwampara)
“The government should make better roads, and where we are referring them for better services” (HW13, female nurse, Kashari)
“The government should put for us facilities in the village like the one you get from here (MRRH) so that when the children are sick, you go to the nearest hospital and we stop struggling when our children fall sick.” (CT6, 45-year-old grandmother)
“They should make sure that in case a child comes and needs oxygen, it should be available. They may not be so many, but the available ones must be in good working condition because when I was still in the hospital, there are some children who died; you could see the health worker struggling, but the oxygen failed, yet the health worker did all she could to save this child’s life.” (CT7, father of a6 month-old with pneumonia)
“The best way to handle this is to tell the clients where our capacity stops during the course of assessment, so that when we refer them they understand our limits.” (HW14, male nurse, Kashari)
“When you are referring someone, put your contacts because more explanations may be required of you from the facility you refer the child to, and they may want to give you feedback…” (HW15, male doctor, Mbarara Municipality)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF; WHO; World Bank Group; United Nations. Levels and Trends in Child Mortality 2020; Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; United Nations Children’s Fund: New York, NY, USA, 2020.
- United Nations. Sustainable Development Goals: United Nations. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 4 March 2021).
- United Nations Children’s Fund (Ed.) UNICEF Data: Monitoring the Situation of Children and Women; Trends in Under-Five Mortality Rate; UNICEF: New York, NY, USA, 2018.
- UNDP. Sustainable Development Goals: UNDP Library. Available online: http://www.undp.org/content/dam/undp/library/corporate/brochure/SDGs_Booklet_Web_En.pdf (accessed on 14 October 2020).
- AAgweyu, A.; Lilford, R.J.; English, M.; Irimu, G.; Ayieko, P.; Akech, S.; Githanga, D.; Were, F.; Kigen, B.; Ng’Arng’Ar, S.; et al. Appropriateness of clinical severity classification of new WHO childhood pneumonia guidance: A multi-hospital, retrospective, cohort study. Lancet Glob. Health 2018, 6, e74–e83. [Google Scholar] [CrossRef]
- Marsh, K.; Forster, D.; Waruiru, C.; Mwangi, I.; Winstanley, M.; Marsh, V.; Newton, C.; Winstanley, P.; Warn, P.; Peshu, N.; et al. Indicators of Life-Threatening Malaria in African Children. N. Engl. J. Med. 1995, 332, 1399–1404. [Google Scholar] [CrossRef]
- Bradley, S.E.; Rosapep, L.; Shiras, T. Where Do Caregivers Take Their Sick Children for Care? An Analysis of Care Seeking and Equity in 24 USAID Priority Countries. Glob. Health Sci. Pract. 2020, 8, 518–533. [Google Scholar] [CrossRef] [PubMed]
- Buregyeya, E.; Rutebemberwa, E.; LaRussa, P.; Lal, S.; Clarke, S.E.; Hansen, K.S.; Magnussen, P.; Mbonye, A.K. Comparison of the capacity between public and private health facilities to manage under-five children with febrile illnesses in Uganda. Malar. J. 2017, 16, 183. [Google Scholar] [CrossRef][Green Version]
- World Health Organization. Management of Health Facilities: Referral Systems. 2017. Available online: https://www.who.int/management/facility/referral/en/ (accessed on 9 May 2021).
- Erin, L.; Katie, R.N.T.; Shelina, M.J.; Von Saint André-von Arnim, A.; Musa, N.L. A Review of Pediatric Critical Care in Resource-Limited Settings: A Look at Past, Present, and Future Directions. Front. Pediatrics 2016, 4, 5. [Google Scholar]
- Gera, T.; Shah, D.; Garner, P.; Richardson, M.; Sachdev, H.S. Integrated management of childhood illness (IMCI) strategy for children under five. Cochrane Database Syst. Rev. 2016, 6. [Google Scholar] [CrossRef]
- Kolstad, P.R.; Burnham, G.; Kalter, H.D.; Kenya-Mugisha, N.; Black, R.E. The integrated management of childhood illness in western Uganda. Bull. World Health Organ. 1997, 75 (Suppl. S1), 77–85. [Google Scholar] [PubMed]
- Kalter, H.; Schillinger, J.A.; Hossain, M.; Burnham, G.; Saha, S.; De Wit, V.; Khan, N.Z.; Schwartz, B.; Black, R. Identifying sick children requiring referral to hospital in Bangladesh. Bull. World Health Organ. 1997, 75 (Suppl. S1), 65. [Google Scholar]
- Perkins, B.A.; Zucker, J.R.; Otieno, J.; Jafari, H.S.; Paxton, L.; Redd, S.C.; Nahlen, B.L.; Schwartz, B.; Oloo, A.J.; Olango, C.; et al. Evaluation of an algorithm for integrated management of childhood illness in an area of Kenya with high malaria transmission. Bull. World Health Organ. 1997, 75 (Suppl. S1), 33–42. [Google Scholar] [PubMed]
- Molyneux, E.; Ahmad, S.; Robertson, A. Improved triage and emergency care for children reduces inpatient mortality in a resource-constrained setting. Bull. World Health Organ. 2006, 84, 314–319. [Google Scholar] [CrossRef]
- Graham, S.M.; English, M.; Hazir, T.; Penny Enarson, P.T.D. Challenges to improving case management of childhood pneumonia at health facilities in resource-limited settings. Bull. World Health Organ. 2008, 86, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.; Nsungwa-Sabiiti, J.; Were, W.; Nsabagasani, X.; Magumba, G.; Nambooze, J.; Mukasa, G. Coping with paediatric referral—Ugandan parents’ experience. Lancet 2004, 363, 1955–1956. [Google Scholar] [CrossRef]
- Nanyonjo, A.; Bagorogoza, B.; Kasteng, F.; Ayebale, G.; Makumbi, F.; Tomson, G.; Källander, K.; inSCALE Study Group. Estimating the cost of referral and willingness to pay for referral to higher-level health facilities: A case series study from an integrated community case management programme in Uganda. BMC Health Serv. Res. 2015, 15, 347. [Google Scholar] [CrossRef]
- Uganda Ministry of Health. Health Systems 20/20, Makerere University School of Public Health. Uganda Health System Assessment 2011; Ministry of Health: Kampala, Uganda, 2012.
- Eskandari, M.; Abbaszadeh, A.F.B. Barriers of Referral System to Health Care Provision in Rural Societies in Iran. J. Caring Sci. 2013, 2, 229–236. [Google Scholar] [PubMed]
- Mwanga-Amumpaire, J.; Alfvén, T.; Obua, C.; Källander, K.; Migisha, R.; Lundborg, C.S.; Ndeezi, G.; Kalyango, J. Appropriateness of Care for Common Childhood Infections at Low-Level Private Health Facilities in a Rural District in Western Uganda. Int. J. Environ. Res. Public Health 2021, 18, 7742. [Google Scholar] [CrossRef]
- Ministry of Health Uganda. Annual Health Perfomance Report; Contract No.: 2018/2019; Ministry of Health Uganda: Kampala, Uganda, 2019.
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design: Choosing among Five Approaches; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Morse, J.M. Determining Sample Size; Sage Publications Sage CA: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Friese, S. Qualitative Data Analysis with ATLAS. ti; SAGE Publications Limited: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Mbonye, A.K.; Buregyeya, E.; Rutebemberwa, E.; Clarke, S.E.; Lal, S.; Hansen, K.S.; Magnussen, P.; LaRussa, P. Referral of children seeking care at private health facilities in Uganda. Malar. J. 2017, 16, 76. [Google Scholar] [CrossRef][Green Version]
- Treleaven, E.; Pham, T.N.; Le, D.N.; Brooks, T.N.; Le, H.T.; Partridge, J.C. Referral patterns, delays, and equity in access to advanced paediatric emergency care in Vietnam. Int. J. Equity Health 2017, 16, 1–11. [Google Scholar] [CrossRef]
- Shittu, F.; Agwai, I.C.; Falade, A.G.; Bakare, A.A.; Graham, H.; Iuliano, A.; Aranda, Z.; McCollum, E.D.; Isah, A.; Bahiru, S.; et al. Health system challenges for improved childhood pneumonia case management in Lagos and Jigawa, Nigeria. Pediatr. Pulmonol. 2020, 55, S78–S90. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Uganda. Health Sector Development Plan 2015/16–2019/20; Ministry of Health Uganda: Kampala, Uganda, 2015.
- Beyene, H.; Hailu, D.; Tadele, H.; Persson, L.Å.; Berhanu, D. Insufficient referral practices of sick children in Ethiopia shown in a cross-sectional survey. Acta Paediatr. 2020, 109, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- Cyr, M.E.; Etchin, A.G.; Guthrie, B.J.; Benneyan, J.C. Access to specialty healthcare in urban versus rural US populations: A systematic literature review. BMC Health Serv. Res. 2019, 19, 1–17. [Google Scholar] [CrossRef]
- Simba, D.O.; Warsame, M.; Kimbute, O.; Kakoko, D.; Petzold, M.; Tomson, G.; Premji, Z.; Gomes, M. Factors influencing adherence to referral advice following pre-referral treatment with artesunate suppositories in children in rural Tanzania. Trop. Med. Int. Health 2009, 14, 775–783. [Google Scholar] [CrossRef]
- Lal, S.; Ndyomugenyi, R.; Paintain, L.; Alexander, N.D.; Hansen, K.S.; Magnussen, P.; Chandramohan, D.; Clarke, S.E. Caregivers’ compliance with referral advice: Evidence from two studies introducing mRDTs into community case management of malaria in Uganda. BMC Health Serv. Res. 2018, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wammanda, R.D.; Adamu, S.A.; Joshua, H.D.; Bin Nisar, Y.; Qazi, S.A.; Aboubaker, S.; Bahl, R. Implementation of the WHO guideline on treatment of young infants with signs of possible serious bacterial infection when hospital referral is not feasible in rural Zaria, Nigeria: Challenges and solutions. PLoS ONE 2020, 15, e0228718. [Google Scholar] [CrossRef] [PubMed]
- Kamau, K.J.; Osuga, B.O.; Njuguna, S. Challenges facing implementation of referral system for quality health care services in Kiambu county, Kenya. Health Syst. Policy Res. 2017, 4, 1–8. [Google Scholar] [CrossRef]
- Newbrander, W.; Ickx, P.; Werner, R.; Mujadidi, F. Compliance with referral of sick children: A survey in five districts of Afghanistan. BMC Pediatr. 2012, 12, 46. [Google Scholar] [CrossRef]
- Allen, E.P.; Muhwezi, W.W.; Henriksson, D.K.; Mbonye, A.K. Health facility management and access: A qualitative analysis of challenges to seeking healthcare for children under five in Uganda. Health Policy Plan. 2017, 32, 934–942. [Google Scholar] [CrossRef]
- Jones, C.H.; Ward, A.; Hodkinson, P.W.; Reid, S.J.; Wallis, L.A.; Harrison, S.; Argent, A.C. Caregivers’ experiences of pathways to care for seriously Ill children in Cape Town, South Africa: A qualitative investigation. PLoS ONE 2016, 11, e0151606. [Google Scholar] [CrossRef]
- Sunny, A.K.; Gurung, R.; Gurung, A.; Basnet, O.; Kc, A. Out of Pocket Expenditure for Sick Newborn Care in Referral Hospitals of Nepal. Matern. Child Health J. 2020, 24, 57–65. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, A.S.; Reschovsky, J.D. Referral and Consultation Communication Between Primary Care and Specialist Physicians: Finding Common Ground. Arch. Intern. Med. 2011, 171, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Ezhumalai, G.; Jayashree, M.; Nallasamy, K.; Bansal, A.; Bharti, B. Referrals to a pediatric emergency department of a tertiary care teaching hospital before and after introduction of a referral education module-a quality improvement study. BMC Health Serv. Res. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Ministry of Health Uganda. Annual Health Sector Perfomance Report 2019–2020; Ministry of Health Uganda: Kampala, Uganda, 2020.
- Kenya Ministry of Health. Kenya Health Sector Referral Strategy (2014–2018); Ministry of Health, Division of Emergency and Disaster Risk Management: Nairobi, Kenya, 2014.
- Massavon, W.; Wilunda, C.; Nannini, M.; Majwala, R.K.; Agaro, C.; De Vivo, E.; Lochoro, P.; Putoto, G.; Criel, B. Effects of demand-side incentives in improving the utilisation of delivery services in Oyam District in northern Uganda: A quasi-experimental study. BMC Pregnancy Childbirth 2017, 17, 431. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Local Governement Republic of Uganda (Ed.) Discretionary Development Equalisation Grant (DDEG) Budget and Implementation Guidelines Effective from FY 2020/21; Ministry of Local Governement Republic of Uganda: Kampala, Uganda, 2020.


{kind=link}
| Level of Health Unit | Target Population | Services Provided and Structures |
|---|---|---|
| Village health teams (Health centre I) | 1000 | First contact for populations living in rural areas, providing community-based preventive and health promotion services, community mobilisation and referral of sick members to health facilities. No physical structures. |
| Health centre II | 5000 | Parish-level facility offering disease prevention, health promotion and outpatient curative health services for uncomplicated conditions, antenatal care and immunisation for children. |
| Health centre III | 20,000 | Sub-county-level facility offering preventive, health promotion, outpatient curative, maternity, inpatient health services and laboratory services for malaria testing and tuberculosis microscopy. |
| Health centre IV | 100,000 | County-level facility offering disease preventive services, health promotion, outpatient curative, maternity, inpatient health services, emergency surgery and blood transfusion and laboratory services. |
| General hospital | 500,000 | District-level facility. In addition to services offered at HC IV, it offers general services and in-service training, consultation and research to community-based healthcare programs. |
| Regional referral hospital | 2,000,000 | In addition to services offered at the general hospital, it offers specialist services, such as psychiatry; ear, nose and throat; ophthalmology; dentistry; intensive care; radiology; pathology; and higher-level surgical and medical services. |
| National referral hospital | 10,000,000 | Offers comprehensive specialist services and is involved in teaching and research. |
| Characteristic | Statistic |
|---|---|
| Caretaker participants (N = 16) | |
| Female sex | 11 |
| Average age | 30.8 years |
| Relationship to child | |
| Mother | 9 |
| Father | 5 |
| Grandmother | 2 |
| Health worker participants (N = 30) | |
| Male sex | 17 |
| Female sex | 13 |
| Average period in practice in years | 6.5 |
| Nurses | 18 |
| Clinical officers | 6 |
| Doctors | 3 |
| Laboratory assistant | 1 |
| Nursing assistants | 2 |
| Theme | Subtheme | Codes |
|---|---|---|
| Reasons for referral | Severely ill child |
|
| Avoiding loss of revenue |
| |
| Loss of prestige |
| |
| Process of referral | Person responsible for referral |
|
| Where to refer |
| |
| How are the referrals done |
| |
| Health worker attitudes to referral | Positive |
|
| Negative feelings |
| |
| Experiences of caretakers | Negative experiences |
|
| Positive experiences |
| |
| Challenges in referral | Non-adherence to referral instructions by caretakers |
|
| Loss of revenue to clinic |
| |
| Lack of feedback from referral facilities |
| |
| How the referral process could be improved | Reduce waiting time |
|
| Improve transportation |
| |
| Reduce costs incurred |
| |
| Improved communication |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mwanga-Amumpaire, J.; Kalyango, J.N.; Ndeezi, G.; Rujumba, J.; Owokuhaisa, J.; Stålsby Lundborg, C.; Alfvén, T.; Obua, C.; Källander, K. A Qualitative Exploration of the Referral Process of Children with Common Infections from Private Low-Level Health Facilities in Western Uganda. Children 2021, 8, 996. https://doi.org/10.3390/children8110996
Mwanga-Amumpaire J, Kalyango JN, Ndeezi G, Rujumba J, Owokuhaisa J, Stålsby Lundborg C, Alfvén T, Obua C, Källander K. A Qualitative Exploration of the Referral Process of Children with Common Infections from Private Low-Level Health Facilities in Western Uganda. Children. 2021; 8(11):996. https://doi.org/10.3390/children8110996
Chicago/Turabian StyleMwanga-Amumpaire, Juliet, Joan Nakayaga Kalyango, Grace Ndeezi, Joseph Rujumba, Judith Owokuhaisa, Cecilia Stålsby Lundborg, Tobias Alfvén, Celestino Obua, and Karin Källander. 2021. "A Qualitative Exploration of the Referral Process of Children with Common Infections from Private Low-Level Health Facilities in Western Uganda" Children 8, no. 11: 996. https://doi.org/10.3390/children8110996
APA StyleMwanga-Amumpaire, J., Kalyango, J. N., Ndeezi, G., Rujumba, J., Owokuhaisa, J., Stålsby Lundborg, C., Alfvén, T., Obua, C., & Källander, K. (2021). A Qualitative Exploration of the Referral Process of Children with Common Infections from Private Low-Level Health Facilities in Western Uganda. Children, 8(11), 996. https://doi.org/10.3390/children8110996