
Sun Exposure in Pediatric Age: Perspective of Caregivers


 ,
,  ,
,
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Internal Consistency of the Caregiver’s Knowledge Section
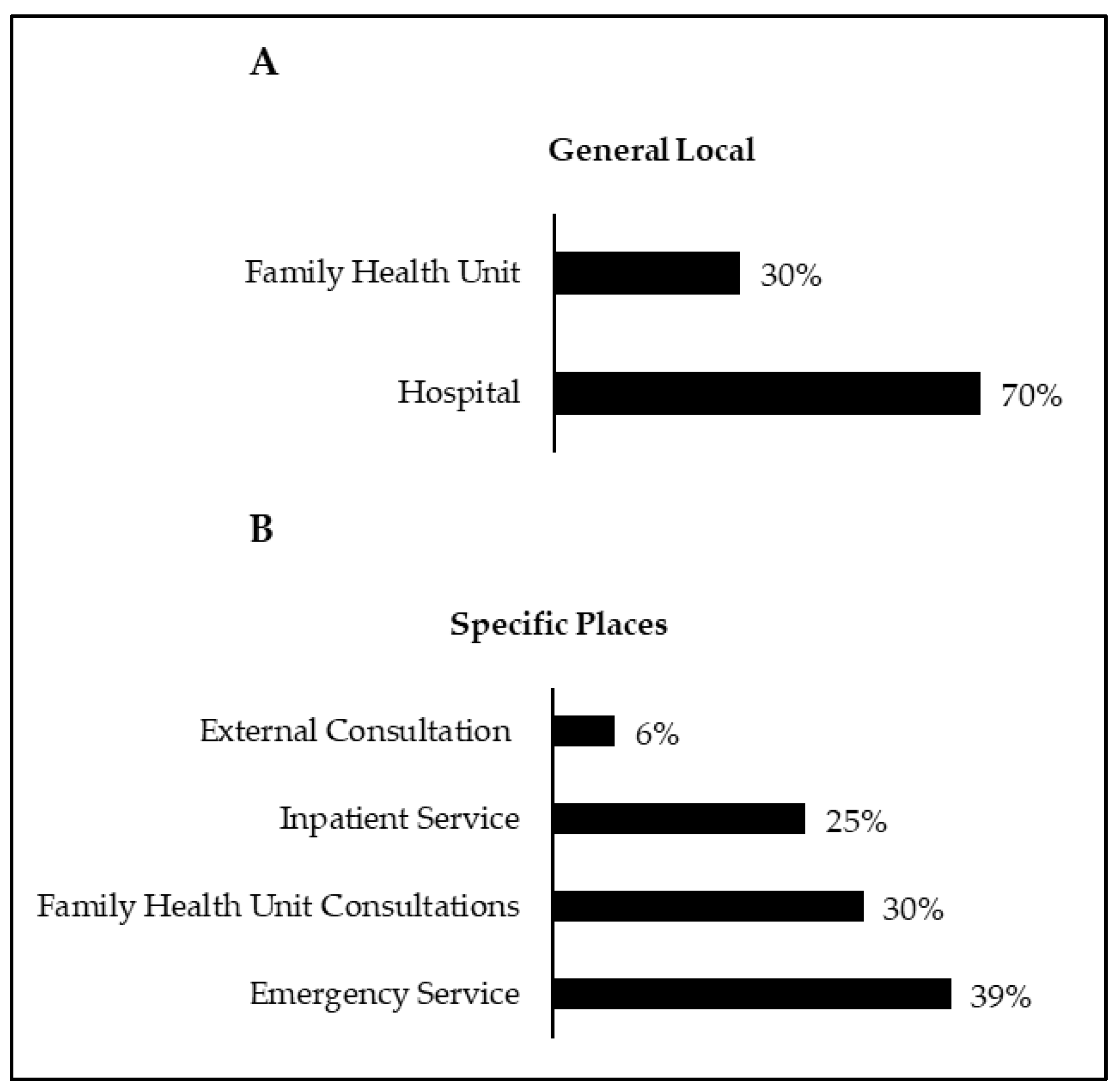
3.2. General Results
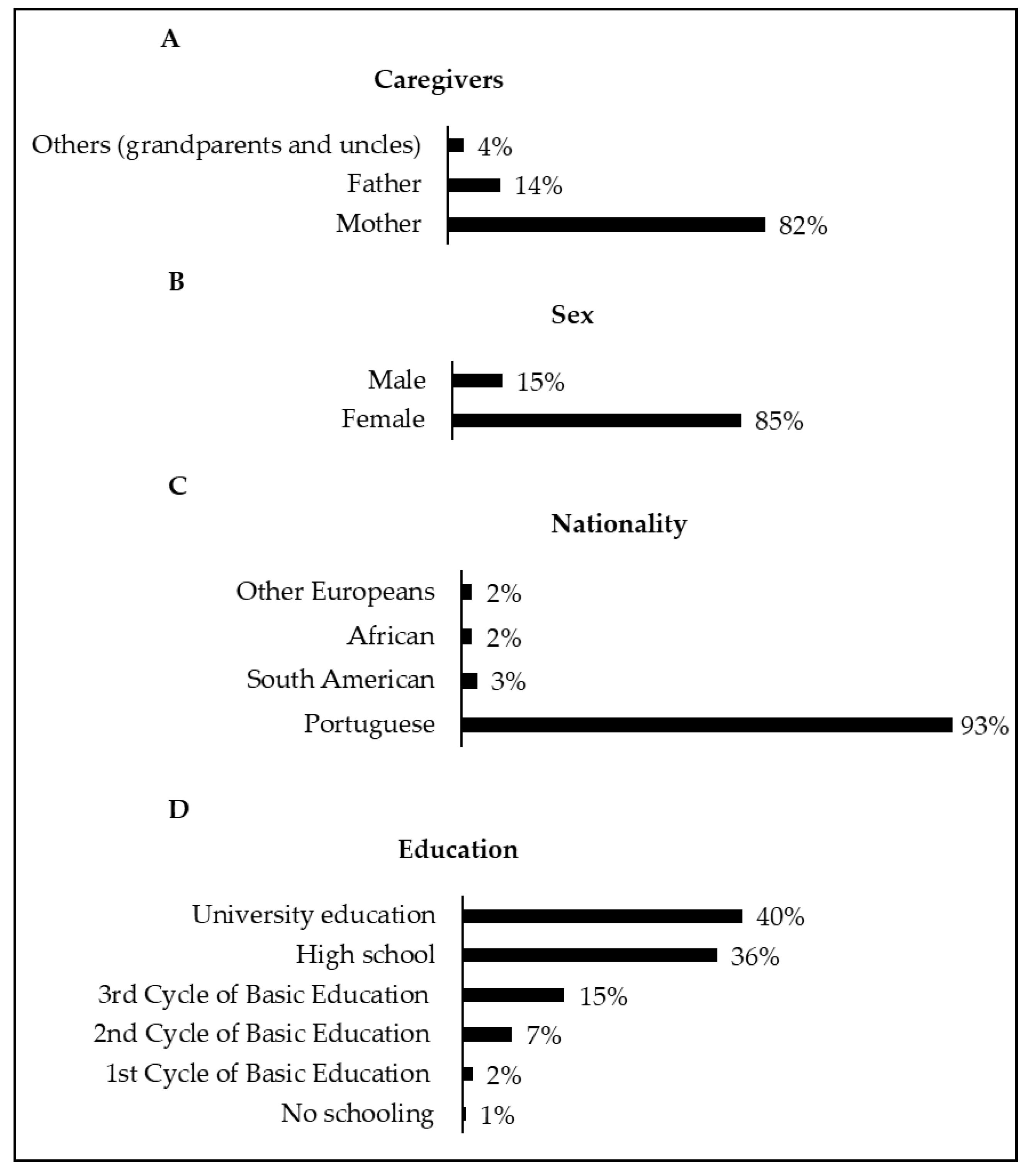
3.3. Characterization of the Caregiver and the Child/Adolescent
3.4. Caregivers’ Knowledge Regarding Exposure and Sun Protection in Children and Adolescents
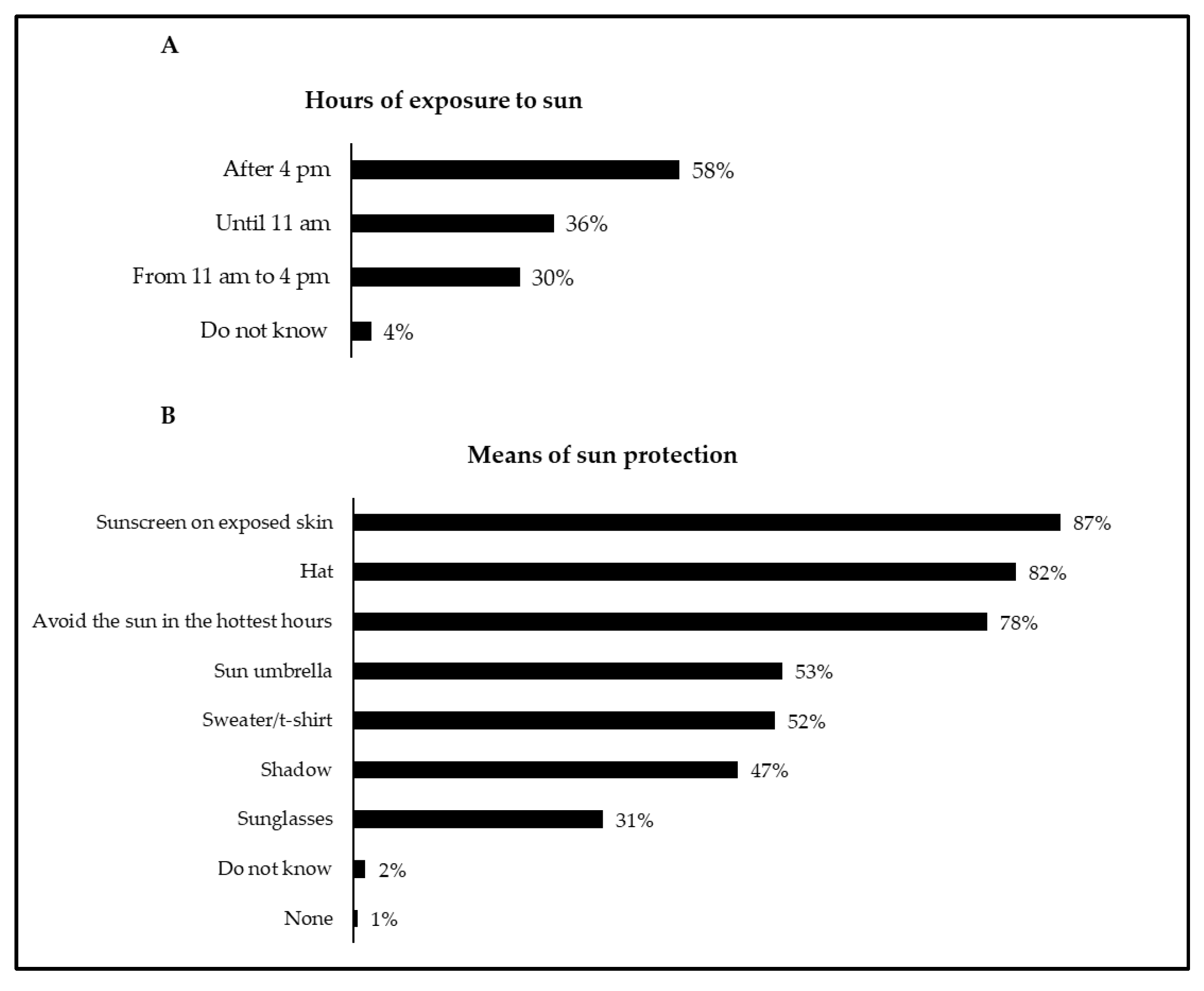
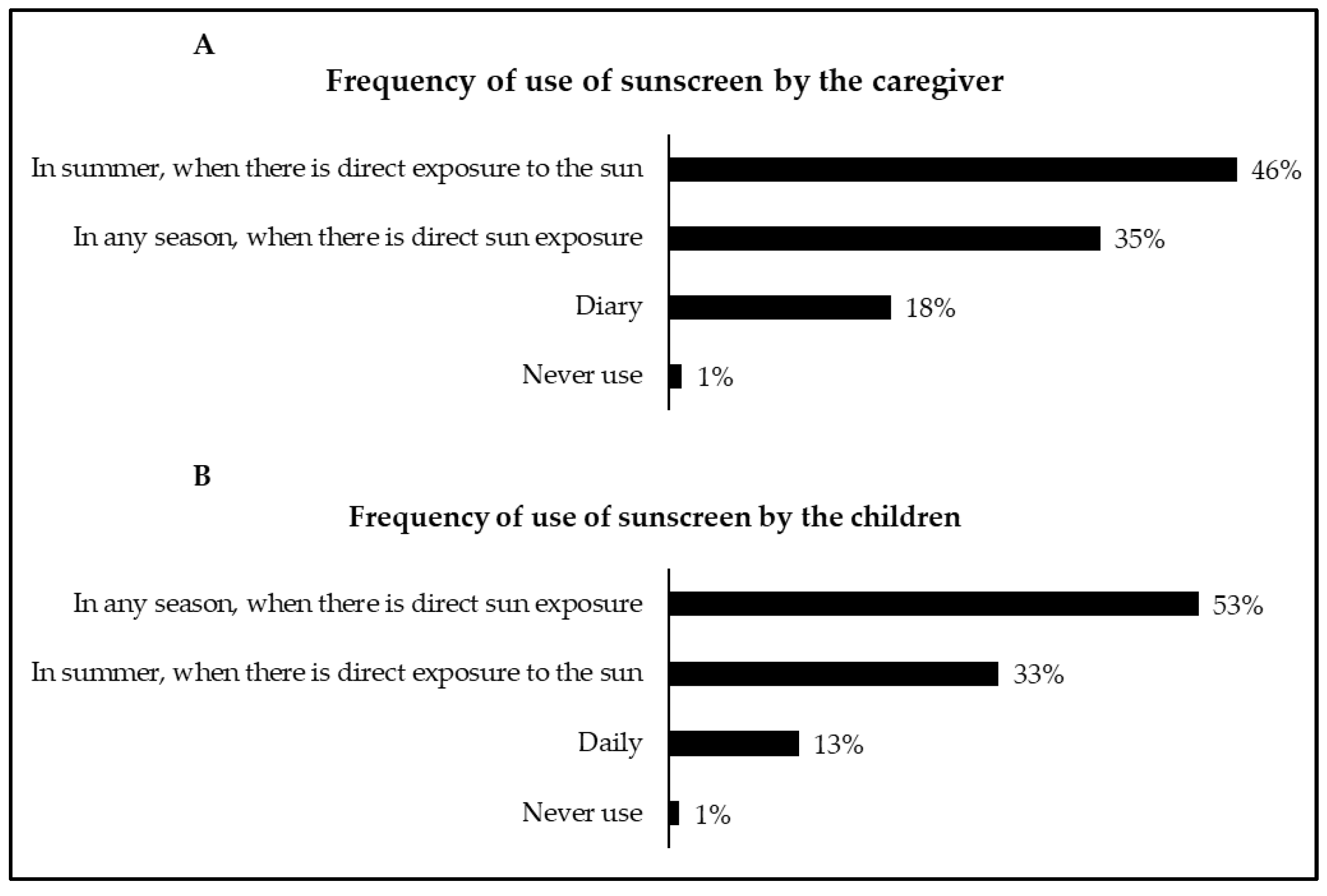
3.5. Attitudes of Caregivers Regarding Exposure and Sun Protection of Children and Adolescents
3.6. Educational Level vs. Caregivers’ Knowledge Regarding Exposure and Sun Protection in Children and Adolescents
3.7. Knowledge vs. Attitudes of Caregivers Regarding Exposure and Sun Protection in Children and Adolescents
4. Discussion
4.1. General Findings
4.2. Caregivers’ Knowledge Regarding Exposure and Sun Protection in Children and Adolescents
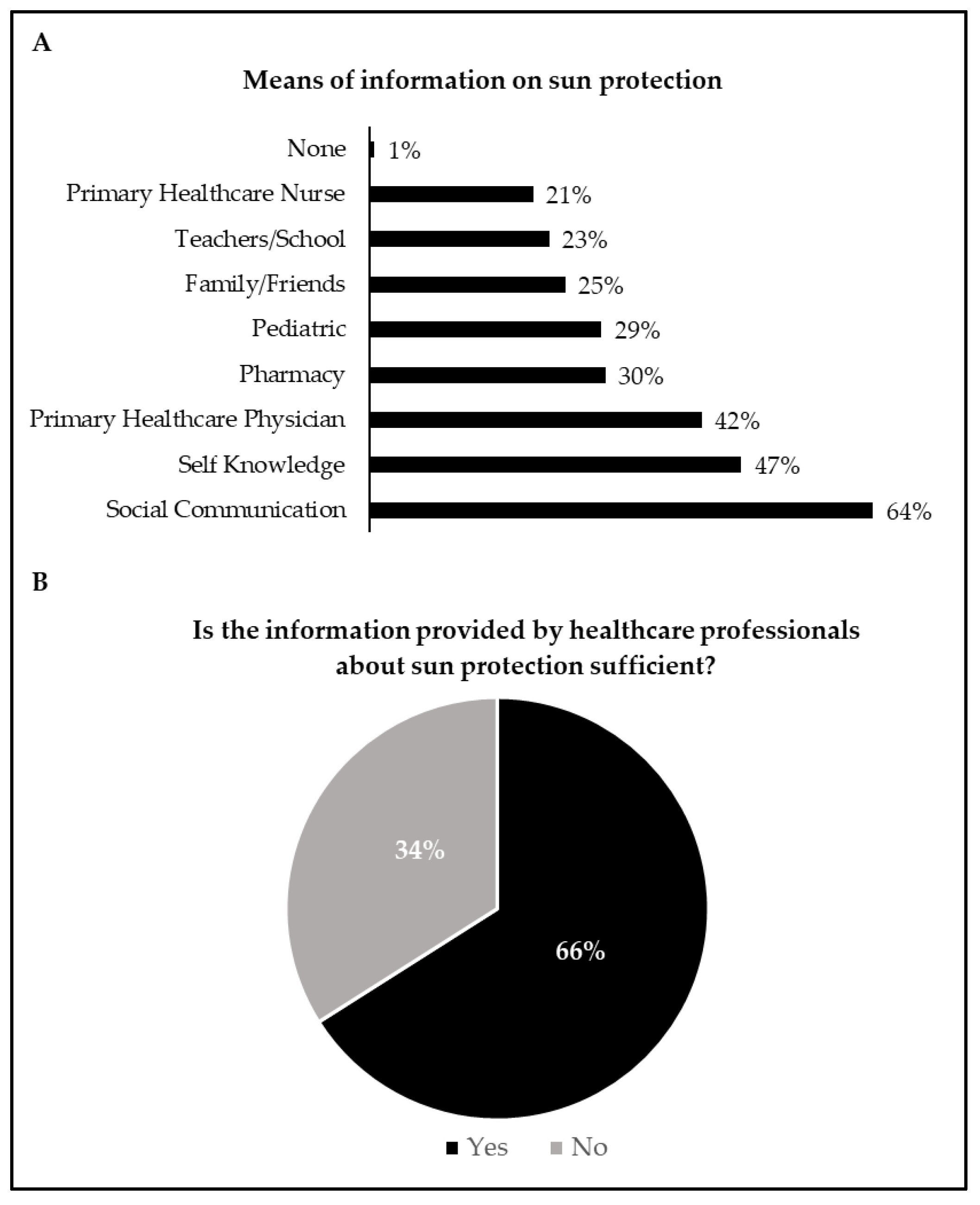
4.3. Means of Information on Sun Protection
4.4. Caregivers’ Attitudes Regarding Exposure and Sun Protection in Children and Adolescents
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gallagher, R.P.; Lee, T.K.; Bajdik, C.D.; Borugian, M. Ultraviolet radiation. Chronic Dis. Can. 2010, 29 (Suppl. 1), 51–68. [Google Scholar] [CrossRef]
- Council on Environmental Health and Section on Dermatology. Ultraviolet Radiation: A Hazard to Children and Adolescents. Pediatrics 2011, 127, 588–597. [Google Scholar] [CrossRef]
- World Health Organization. Artificial Tanning Devices: Public Health Interventions to Manage Sunbeds; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Moan, J.; Grigalavicius, M.; Baturaite, Z.; Dahlback, A.; Juzeniene, A. The relationship between UV exposure and incidence of skin cancer. Photodermatol. Photoimmunol. Photomed. 2015, 31, 26–35. [Google Scholar] [CrossRef]
- Amaro-Ortiz, A.; Yan, B.; D’Orazio, J. Ultraviolet Radiation, Aging and the Skin: Prevention of Damage by Topical cAMP Manipulation. Molecules 2014, 19, 6202–6219. [Google Scholar] [CrossRef]
- Lowe, J.B. Behavior of caregivers to protect their infants from exposure to the sun in Queensland, Australia. Health Educ. Res. 2002, 17, 405–414. [Google Scholar] [CrossRef][Green Version]
- Oliveria, S.A.; Saraiya, M.; Geller, A.C.; Heneghan, M.K.; Jorgensen, C. Sun exposure and risk of melanoma. Arch. Dis. Child. 2005, 91, 131–138. [Google Scholar] [CrossRef]
- Cust, A.E.; Jenkins, M.A.; Goumas, C.; Armstrong, B.K.; Schmid, H.; Aitken, J.F.; Giles, G.G.; Kefford, R.F.; Hopper, J.L.; Mann, G.J. Early-life sun exposure and risk of melanoma before age 40 years. Cancer Causes Control 2011, 22, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Long, M. Sun Exposure. Pediatr. Rev. 2017, 38, 446–447. [Google Scholar] [CrossRef] [PubMed]
- RON. Registo Oncológico Nacional 2018; Registo Oncológico Nacional: Lisboa, Portugal, 2018; ISBN 978-989-95380-3-0. [Google Scholar]
- Robinson, J.K.; Rigel, D.S.; Amonette, R.A. Summertime sun protection used by adults for their children. J. Am. Acad. Dermatol. 2000, 42, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Julian, E.; Palestro, A.M.; Thomas, J.A. Pediatric Sunscreen and Sun Safety Guidelines. Clin. Pediatr. 2015, 54, 1133–1140. [Google Scholar] [CrossRef]
- Balato, N.; Gaudiello, F.; Balato, A.; Monfrecola, G. Sun habits in the children of Southern Italy. J. Am. Acad. Dermatol. 2007, 57, 883–887. [Google Scholar] [CrossRef]
- Green, A.C.; Wallingford, S.C.; McBride, P. Childhood exposure to ultraviolet radiation and harmful skin effects: Epidemiological evidence. Prog. Biophys. Mol. Biol. 2011, 107, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Leite, J.; Domingues, S.; Sampaio, J.; Braga, R. Conhecimentos e Atitudes dos Cuidadores acerca da Exposição Solar em Idade Pediátrica. Acta Pediátr. Port. 2014, 45, 22–25. [Google Scholar]
- Ribeiro, C.; Relvas, A.; Carvalho, L.; Costa, V.; Gomes, L.; Costa, M. Proteção solar: Conhecimentos e hábitos na população pediátrica. Nascer E Crescer Birth Growth Med. J. 2017, 26, 31–35. [Google Scholar]
- Görig, T.; Södel, C.; Pfahlberg, A.B.; Gefeller, O.; Breitbart, E.W.; Diehl, K. Sun Protection and Sunburn in Children Aged 1–10 Years in Germany: Prevalence and Determinants. Children 2021, 8, 668. [Google Scholar] [CrossRef] [PubMed]
- Thoonen, K.; Schneider, F.; Candel, M.; de Vries, H.; van Osch, L. Childhood sun safety at different ages: Relations between parental sun protection behavior towards their child and children’s own sun protection behavior. BMC Public Health 2019, 19, 1044. [Google Scholar] [CrossRef]
- Whicher, D.; Wu, A.W. Ethics Review of Survey Research: A Mandatory Requirement for Publication? Patient-Patient-Cent. Outcomes Res. 2015, 8, 477–482. [Google Scholar] [CrossRef]
- Alsoghair, M.; Almazyad, M.; Alburaykan, T.; Alsultan, A.; Alnughaymishi, A.; Almazyad, S.; Alharbi, M.; Alkassas, W.; Almadud, A.; Alsuhaibani, M. Medical Students and COVID-19: Knowledge, Preventive Behaviors, and Risk Perception. Int. J. Environ. Res. Public Health 2021, 18, 842. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Hisham, R.; Ng, C.J.; Liew, S.M.; Lai, P.S.M.; Chia, Y.C.; Khoo, E.M.; Hanafi, N.S.; Othman, S.; Lee, P.Y.; Abdullah, K.L.; et al. Development and validation of the Evidence Based Medicine Questionnaire (EBMQ) to assess doctors’ knowledge, practice and barriers regarding the implementation of evidence-based medicine in primary care. BMC Fam. Pract. 2018, 19, 98. [Google Scholar] [CrossRef] [PubMed]
- Gefeller, O.; Uter, W.; Pfahlberg, A.B. Good, but Not Perfect: Parental Knowledge About Risk Factors for Skin Cancer and the Necessity of Sun Protection in Southern Germany. Pediatr. Dermatol. 2015, 32, e159–e160. [Google Scholar] [CrossRef]
- Cercato, M.C.; Nagore, E.; Ramazzotti, V.; Sperduti, I.; Guillén, C. Improving Sun-Safe Knowledge, Attitude and Behaviour in Parents of Primary School Children: A Pilot Study. J. Cancer Educ. 2013, 28, 151–157. [Google Scholar] [CrossRef]
- Li, J.; Uter, W.; Pfahlberg, A.; Gefeller, O. Parental perspective on sun protection for young children in Bavaria. Photodermatol. Photoimmunol. Photomed. 2011, 27, 196–202. [Google Scholar] [CrossRef]
- Gefeller, O.; Uter, W.; Pfahlberg, A. Protection from Ultraviolet Radiation during Childhood: The Parental Perspective in Bavaria. Int. J. Environ. Res. Public Health 2016, 13, 1011. [Google Scholar] [CrossRef]
- Mortier, L.; Lepesant, P.; Saiag, P.; Robert, C.; Sassolas, B.; Grange, F.; Lhomel, C.; Lebbe, C. Comparison of sun protection modalities in parents and children. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 16–19. [Google Scholar] [CrossRef]
- O’Riordan, D.L.; Geller, A.C.; Brooks, D.R.; Zhang, Z.; Miller, D.R. Sunburn reduction through parental role modeling and sunscreen vigilance. J. Pediatr. 2003, 142, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Horváth, Z.; Evelin, C.A.; Oláh, P.; Gyulai, R.; Lengyel, Z. Results of a Primary Skin-Cancer-Prevention Campaign in Early Childhood on Sun-Related Knowledge and Attitudes in Southern Hungary. Cancers 2021, 13, 3873. [Google Scholar] [CrossRef] [PubMed]
- Langbecker, D.; Diaz, A.; Chan, R.J.; Marquart, L.; Hevey, D.; Hamilton, J. Educational programmes for primary prevention of skin cancer. Cochrane Database Syst. Rev. 2018, 2018, CD011061. [Google Scholar] [CrossRef]
- Gefeller, O.; Li, J.; Uter, W.; Pfahlberg, A. The Impact of Parental Knowledge and Tanning Attitudes on Sun Protection Practice for Young Children in Germany. Int. J. Environ. Res. Public Health 2014, 11, 4768–4781. [Google Scholar] [CrossRef]
- Gefeller, O.; Uter, W.; Pfahlberg, A.B. Long-term development of parental knowledge about skin cancer risks in Germany: Has it changed for the better? Prev. Med. 2016, 89, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Køster, B.; Søndergaard, J.; Nielsen, J.B.; Christensen, K.B.; Allen, M.; Olsen, A.; Bentzen, J. Knowledge deficit, attitude and behavior scales association to objective measures of sun exposure and sunburn in a Danish population based sample. PLoS ONE 2017, 12, e0178190. [Google Scholar] [CrossRef]
- Uter, W.; Fießler, C.; Gefeller, O.; Pfahlberg, A. Knowledge and sources of knowledge about skin cancer risk factors in parents of 3 to 6 year old children. Bundesgesundheitsblatt Gesundheitsforsch. Gesundh. 2017, 60, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Uter, W.; Eversbusch, C.; Gefeller, O.; Pfahlberg, A. Quality of Information for Skin Cancer Prevention: A Quantitative Evaluation of Internet Offerings. Healthcare 2021, 9, 229. [Google Scholar] [CrossRef] [PubMed]
- Schlarbaum, J.P.; Hook, K.P. Characterizing online searches in pediatric dermatology. Pediatr. Dermatol. 2020, 37, 1212–1213. [Google Scholar] [CrossRef]
- Filipa, D.; Osvaldo, C.; João Nuno Maia e, S.; Cecília, M.; Ricardo, V.; António, P. Euromelanoma in Portugal 2010–2016. J. Port. Soc. Dermatol. Venereol. 2018, 75, 345–355. [Google Scholar] [CrossRef][Green Version]
- Narayanan, D.L.; Saladi, R.N.; Fox, J.L. Review: Ultraviolet radiation and skin cancer. Int. J. Dermatol. 2010, 49, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Klostermann, S.; Bolte, G. Determinants of inadequate parental sun protection behaviour in their children—Results of a cross-sectional study in Germany. Int. J. Hyg. Environ. Health 2014, 217, 363–369. [Google Scholar] [CrossRef]
- Kiely, A.D.; Hourihane, J. Sun exposure and sun protection practices of children and their parents. Ir. Med. J. 2009, 102, 139–140, 142–143. [Google Scholar]
- Vashist, P.; Tandon, R.; Murthy, G.V.S.; Barua, C.K.; Deka, D.; Singh, S.; Gupta, V.; Gupta, N.; Wadhwani, M.; Singh, R.; et al. Association of cataract and sun exposure in geographically diverse populations of India: The CASE study. First Report of the ICMR-EYE SEE Study Group. PLoS ONE 2020, 15, e0227868. [Google Scholar] [CrossRef]
- Tang, Y.; Ji, Y.; Ye, X.; Wang, X.; Cai, L.; Xu, J.; Lu, Y. The Association of Outdoor Activity and Age-Related Cataract in a Rural Population of Taizhou Eye Study: Phase 1 Report. PLoS ONE 2015, 10, e0135870. [Google Scholar] [CrossRef]
- Hamilton, K.; Cleary, C.; White, K.M.; Hawkes, A.L. Keeping kids sun safe: Exploring parents’ beliefs about their young child’s sun-protective behaviours. Psycho-Oncology 2016, 25, 158–163. [Google Scholar] [CrossRef] [PubMed]
- de Gálvez, M.V.; Aguilera, J.; Buendía, E.A.; Sánchez-Roldán, C.; Herrera-Ceballos, E. Time required for a standard sunscreen to become effective following application: A UV photography study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, e123–e124. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Colantonio, S.; Dawson, A.; Lin, X.; Beecker, J. Sunscreen Application, Safety, and Sun Protection: The Evidence. J. Cutan. Med. Surg. 2019, 23, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Direção-Geral da Saúde. Programa Nacional de Saúde Infantil e Juvenil 2013; DGS: Lisboa, Portugal, 2013.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sentence | CD | D | NAND | A | CA |
|---|---|---|---|---|---|
| 1. Excessive sun exposure carries health risks such as sunburn, premature skin aging, skin cancer, or eye problems. | 0.5% | 0.5% | 1% | 14% | 84% |
| 2. The risk of developing skin cancer is related to the amount of ultraviolet radiation a person is exposed to during their lifetime, especially during childhood. | 1% | 3% | 11% | 42% | 43% |
| 3. There is no need to use sun protection measures during the winter months. | 33% | 50% | 10% | 5% | 2% |
| 4. At the beach and pool, it is enough to put on sunscreen once. | 59% | 29% | 3% | 5% | 4% |
| 5. The smaller the shadow, the more dangerous the sun. | 6% | 17% | 26% | 28% | 23% |
| 6. There is no danger of being exposed to the sun longer if you use sunscreen. | 32% | 51% | 9% | 6% | 2% |
| 7. The proper time to apply the protector is on arrival at the beach. | 34% | 48% | 4% | 11% | 3% |
| 8. It is possible to suffer a sunburn on a cloudy day. | 1% | 3% | 3% | 35% | 58% |
| 9. Avoid sun exposure between 11:00 a.m. and 4:00 a.m. | 3% | 1% | 2% | 31% | 63% |
| 10. It is only necessary to use sunscreen at the beach or pool. | 48% | 45% | 4% | 1% | 2% |
| 11. People with dark skin do not need to take special care when they are in the sun. | 50% | 46% | 1.5% | 2% | 0.5% |
| 12. The tan protects you from additional sunburn. | 41% | 49% | 8% | 2% | 0% |
| 13. The higher the altitude, the more easily you can get sunburned. | 4% | 20% | 33% | 30% | 13% |
| 14. Being in the shade of a sun hat or awning is enough to avoid getting sunburned. | 24% | 54% | 13% | 8% | 1% |
| 15. The protective effectiveness starts right after the application of the sunscreen. | 11% | 35% | 17% | 34% | 3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvado, M.; Fraga, A.; Marques, D.L.; Pires, I.M.; Gonçalves, C.C.; Silva, N.M. Sun Exposure in Pediatric Age: Perspective of Caregivers. Children 2021, 8, 1019. https://doi.org/10.3390/children8111019
Salvado M, Fraga A, Marques DL, Pires IM, Gonçalves CC, Silva NM. Sun Exposure in Pediatric Age: Perspective of Caregivers. Children. 2021; 8(11):1019. https://doi.org/10.3390/children8111019
Chicago/Turabian StyleSalvado, Mafalda, Ana Fraga, Diogo Luís Marques, Ivan Miguel Pires, Carmo Coelho Gonçalves, and Nádia Mendes Silva. 2021. "Sun Exposure in Pediatric Age: Perspective of Caregivers" Children 8, no. 11: 1019. https://doi.org/10.3390/children8111019
APA StyleSalvado, M., Fraga, A., Marques, D. L., Pires, I. M., Gonçalves, C. C., & Silva, N. M. (2021). Sun Exposure in Pediatric Age: Perspective of Caregivers. Children, 8(11), 1019. https://doi.org/10.3390/children8111019