Abstract
(1) Background: the impact of a series of laboratory parameters (haemoglobin, haematocrit, foetal haemoglobin, peripheral oxygen saturation, iron, transferrin, ferritin, and albumin) on perimembranous ventricular septal defects spontaneous healing was tested. (2) Methods: one hundred and seven patients were enrolled in the study (57% males; mean age 2.1 ± 0.4 years) and were subsequently subdivided into two groups: self-healing (n = 36) and in need of intervention (n = 71). Self-healing subjects were defined on the basis of an absence of residual shunts at colorDoppler across the previous defect. (3) Results: no statistically significant differences were reported in the size of perimembranous ventricular septal defects between the two groups (p = ns). Conversely, prevalence of anaemia was significantly higher in those requiring intervention than in the self-healing group (p < 0.03), while haemoglobin, iron, ferritin, and albumin levels were lower (p < 0.001, p < 0.05, p < 0.02, p < 0.007, respectively). In multivariable linear regression analysis, only haemoglobin and albumin were found to be associated with spontaneous closure (p < 0.005 and p < 0.02, respectively). In multiple logistic regression analysis, haemoglobin independently increased the probability of self-healing of perimembranous ventricular septal defects (p = 0.03). All patients needing an interventional closure of perimembranous ventricular septal defects presented with haemoglobin <12.7 g/dL. (4) Conclusion: the self-resolution of perimembranous ventricular septal defects seems to rely on numerous factors, including oxygen content, which is likely to promote cell proliferation as well as tissue regeneration. Haemoglobin blood concentration seems to influence the natural history of perimembranous ventricular septal defects and improvement of anaemia by supplementation of iron intake might represent a simple and reliable method to promote self-healing.
1. Introduction
Ventricular septal defect, manifested either as an isolated event or in conjunction with other cardiac abnormalities in syndromic and non-syndromic patients, is by far the most frequently encountered congenital heart defect (CHD) after bicuspid aortic valve in clinical practice, accounting for approximately 20% of all diagnoses when isolated [1,2]. Numerous classifications for ventricular septal defects have been proposed, although it is indisputable that perimembranous ventricular septal defect is the most frequently observed subtype in children (Figure 1), whilst a muscular presentation is most common in newborns.
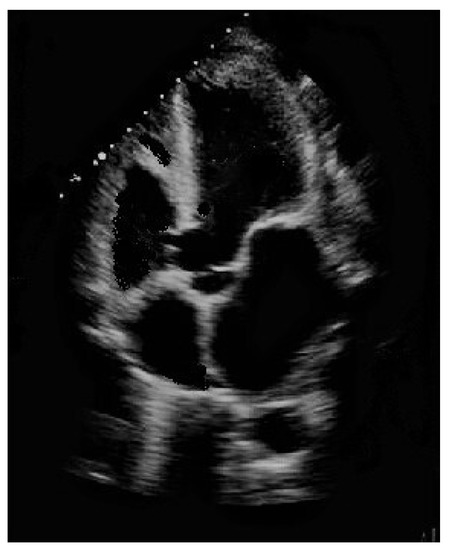
Figure 1.
Perimembranous ventricular septal defect partially occluded by tricuspid valve accessory tissue.
At birth, approx. 8% of detected ventricular septal defects are perimembranous, i.e., involving both the membranous septum and the adjacent muscular area [3]. Diagnosis of ventricular septal defect is usually simple, being mainly based on echocardiography, a widely used technique that also facilitates follow-up of the course of ventricular septal defect [4].
Numerous studies have demonstrated self-healing of perimembranous ventricular septal defects in 10–30% of cases, thus avoiding the potential peri-procedural complications associated with repairs performed by means of conventional surgery or transcatheter-occluding devices [5,6].
Anaemia is frequently observed in both children and adults affected by all types of CHD, including ventriular septal defects at all ages [7,8]. Renal impairment, abnormal iron metabolism, malnutrition, and circulatory congestion contribute independently toward the occurrence of anemia in CHD [9].
This study aimed to assess the impact of a series of laboratory parameters on spontaneous full healing of perimembranous ventricular septal defect: haemoglobin, haematocrit, foetal haemoglobin, peripheral oxygen saturation, iron, transferrin, ferritin, and albumin blood levels.
2. Materials and Methods
2.1. Patients in the Study
In this retrospective study, medical records of patients affected by perimembranous ventricular septal defect attending the Paediatric Cardiology Unit of the University of Cagliari (Italy) from January 1986 to February 2006 were examined. No additional subjects could be evaluated due to closure of the above-cited unit. Following a review of hardcopy medical records and electronic health records, one hundred and seven patients were included in the study (57% males), ranging from 1 day of life to 6 years (mean age 2.1 ± 0.4 years). Clinical and echocardiographic characteristics of study participants are listed in Table 1.

Table 1.
Characteristics of the patients in the study (mean ± standard deviation).
Inclusion criteria were: presence of a perimembranous ventricular septal defect without other CHD, with the exception of transient patent ductus arteriosus, small atrial septal defect and/or one or more minor muscular ventricular septal defects; when surgical closure was indicated due to a large volume left-to-right shunt (Qp/Qs > 2:1), in the presence of significant pulmonary arterial hypertension (pulmonary arterial pressure > 50% systemic), clinical signs of congestive heart failure, banding of the pulmonary artery, or when closure of the perimembranous ventricular septal defect was deemed clinically necessary by the treating physician. Exclusion criteria comprised: ventricular septal defect exceeding 10 mm and/or a ventricular septal defect size/aortic diameter ratio higher than 2/3 (in which case spontaneous closure is improbable); patients presenting with multiple severe muscular ventricular septal defects and/or complex CHD; presence of ongoing bacterial infections/sepsis; haematological disorders (mainly haemolytic disease of the newborn); insufficient laboratory findings. Patients were subdivided into two groups: self-healing (n = 36) and those in need of intervention (n = 71).
Diagnosis was formulated and echocardiographic follow-up implemented. A HP/Philips Sonos 5500, (Amstedam, The Netherlands) echo machine coupled with two probes (3–5 Mhz and 8–10 Mhz) was used. Patients diagnosed with perimembranous ventricular septal defect were followed-up until either the hole in the interventricular septum closed spontaneously or surgical closure was performed. The net defect was measured, which may be smaller than the true due to tricuspid pouch formation. The self-healing group was defined on the basis of an absence of residual shunts at colorDoppler across the former perimembranous ventricular septal defect.
Written informed consent was waived owing to the retrospective nature of the research, as per Italian Law. The research was formally approved by the internal Ethics Committee of the University of Cagliari (PG/2015/1859) and conducted in accordance with the Helsinki declaration.
2.2. Laboratory Tests
The following blood parameters capable of affecting tissue oxygenation were evaluated on a blood sample taken from an antecubital vein-haemoglobin: normal haemoglobin values for children vary according to the child’s age, sex, and race. Anaemia is defined in the presence of a haemoglobin value at or below the 2.5th percentile for age, race, and sex [9,10].
- -
- haematocrit [11,12]
- -
- foetal haemoglobin: the most important oxygen-transport protein in the human foetus [13]
- -
- oxygen saturation [14]
- -
- serum iron levels [15].
- -
- transferrin [16]
- -
- ferritin [16]
- -
-
Table 2. Laboratory parameters tested in the study.
Table 3. Haemoglobin hematic concentration (g/dL) normal values.
Table 4. Haematocrit normal values (%).
2.3. Statistical Analysis
The results obtained in the study population (n = 107) were analysed and the findings obtained in the self-healing group subsequently compared with those from the group requiring intervention using the parametric Student’s t-test, as the sample was normally distributed. Normality was assessed by means of the Kolmogorov–Smirnov test. Multivariate analysis was also performed to analyse more than one outcome variable. The model included the hematic variables which tested statistically significantly different between the two subgroups (i.e., haemoglobin, iron, ferritin, albumin) along with age and gender. For the purpose of this paper, statistical significance was set at <0.05. Commercially available computer software (SPSS version 22.0, SPSS Inc., Chicago, IL, USA) was used for all analyses.
3. Results
The findings obtained in the self-healing group vs the group requiring intervention are summarized in Table 5.
Table 5.
Results (SHG vs NIG).
Regarding the time required by the two groups to reach their outcome, it was statistically significant. Since no statistically significant differences were detected in the dimensions of ventricular septal defect between the two groups, the need for an early intervention was likely due to a drop in pulmonary vascular resistances, which led to a significant left-to-right shunt and in turn to pulmonary overflow and heart failure. Furthermore, anaemia was significantly more prevalent amongst subjects requiring intervention than in the self-healing group (p < 0.03), while haemoglobin, iron, ferritin, and albumin levels were lower (p < 0.001, p < 0.05, p < 0.02, p < 0.007, respectively).
At multivariable linear regression analysis only haemoglobin and albumin featuring an association with spontaneous closure of perimembranous ventricular septal defect (p < 0.005 and p < 0.02, respectively). Multiple logistic regression analysis revealed that haemoglobin independently raised the probability that self-resolution of ventricular septal defect would be achieved (p = 0.03).
Haemoglobin levels in all patients in the needing intervention group was less than 12.7 g/dL (Figure 2).
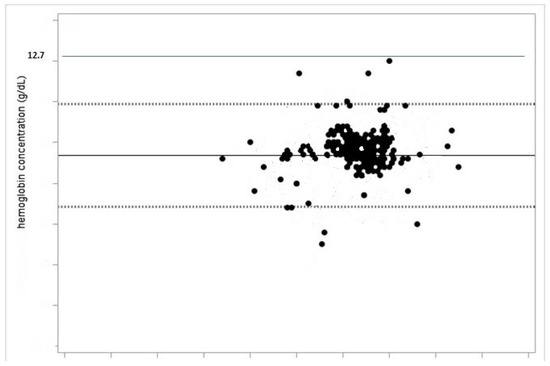
Figure 2.
All the patients in the study whose perimembranous ventricular septal defect did not heal by itself had a haemoglobin level less than 12.7 g/dL.
4. Discussion
In clinical practice, the most commonly observed CHD is represented by ventricular septal defect, of which a considerable percentage displays a tendency to decrease in size and to self-heal. Numerous mechanisms of spontaneous closure of perimembranous ventricular septal defect have been described previously [19].
The present study excluded both muscular ventricular septal defects and other subtypes. The former present with a completely different natural history compared with the perimembranous form, i.e., spontaneous healing in 85%–90% of cases due to a progressive muscularization of the left ventricle, while for other subtypes the rate of spontaneous healing is very low [20].
Furthermore, perimembranous ventricular septal defects with dimensions exceeding 10 mm and/or a ventricular septal defect size/aortic diameter >2/3 ratio were excluded from the study due to the improbability of spontaneous closure occurring [21]. This might explain why our findings highlighted no significant differences in ventricular septal defect size between the two groups studied.
A slight prevalence of the disease amongst males was detected in our cohort. Generally speaking, no significant sex-related differences in ventricular septal defect prevalence are reported in literature [22].
Numerous anatomical parameters have been put forward as potential independent predictors influencing the spontaneous healing of ventricular septal defects. However, more detailed knowledge should be acquired, and the biological mechanisms implicated better elucidated [23]. Accordingly, a series of hematic factors potentially underlying the spontaneous resolution of perimembranous ventricular septal defects were examined.
Anemic infants have ventricular septal defects more frequently than those with normal haemoglobin levels [24]. Haemoglobin is capable of promoting tissue regeneration, cells proliferation and wound healing, as both processes rely heavily on oxygenation. There is no doubt that an adequate supply of nutrients and oxygen to regenerating cells is crucial for their survival and functional maintenance [25].The natural healing of perimembranous ventricular septal defects involves a series of different mechanisms, including tissue growth from the remnant membranous septum or tricuspid valve and adhesion of tricuspid valve leaflets [19]. Tissue regeneration seems to be influenced by haemoglobin-related tissue oxygenation in a number of clinical scenarios [26]. Moreover, correct blood viscosity represents another factor of importance in promoting the adhesion of tricuspid valve leaflet to the tissue surrounding perimembranous ventricular septal defects [19]. Blood viscosity is intricately linked to haemoglobin content: the higher the haemoglobin levels, the higher the hematic viscosity and vice versa [27]. Anaemia, and subsequently reduced blood viscosity, may exert a negative influence on the above-stated adhesion, thus impinging on the natural resolution of ventricular septal defect [28]. Not only, but left-to-right shunt across ventricular septal defect may lead to a volume overload to the lungs, as expressed by QP/Qs ratio higher than 1.1, with consequent further dilution of haemoglobin [29]. Major and minor forms of thalassemia and other types of anaemia are considerably diffuse in Sardinia, i.e., the Italian region where the research was carried out, which may have negatively affected the number of self-healing patients in our cohort [30]. Our research showed a significantly lower prevalence of anaemia in the self-healing group than in those needing intervention. Our findings also suggest a value of 12.7 g/dL in haemoglobin content, above which level the self-healing of ventricular septal defect is unlikely. Overall, as confirmed also at multivariate analysis, haemoglobin blood concentration seems to influence the natural history of ventricular septal defect, and improvement of anaemia through supplementation of iron intake might represent a simple and reliable method of promoting the spontaneous healing of perimembranous vetricular septal defects [31].
Albumin levels were significantly higher in the self-healing group than in patients requiring intervention. In a previous study, hypoalbuminemia, commonly observed in patients with CHD, was found to be associated with an increased risk of death, even after adjustment for disease complexity, functional class, and other risk factors [32]. Low albumin levels are likely caused by acute and/or chronic heart disease due to systolic or diastolic left ventricular dysfunction, which are not uncommon in ventricular septal defect patients [33,34]. Some animal models have also suggested a role of albumin in promoting early wound healing [35,36].
This study is undoubtedly hampered by several limitations: (1) the study was of a single centre retrospective design and therefore contingent on the inherent bias associated with this type of study (missing data; referral and selection bias); (2) over the period examined (1986–2006), the majority of surgical procedures were delayed compared with current standard decision making and a smaller number of interventional perimembranous ventricular septal defect closures were performed [37]. This may have slightly influenced our findings; (3) other unevaluated factors of an epigenetic nature might have influenced the results [38]. In this setting, artificial intelligence and machine learning may represent a potential way to detect important predictors of perimembranous ventricular septal defect self-resolution. The superior performance of machine learning in detecting haemoglobin-related and genetic predictors of cardiovascular endpoints has been already shown in some papers [39,40]; (4) anaemia, or conversely, polycythaemia and ventricular septal defect are not uncommon in Trisomy 21 patients, although the possible effect of Down syndrome itself on self-healing was not investigated [41,42]; recently, a scoring system aimed at predicting spontaneous healing of perimembranous ventricular septal defect, mainly based on anatomical factors, was proposed, although it was not tested in this study [43].
5. Conclusions
Overall, the self-resolution of perimembranous ventricular septal defect seems to rely on numerous different factors, including oxygen content, which likely promotes cell proliferation as well as tissue regeneration. Accordingly, in the presence of low oxygen saturation at a high altitude, ventricular septal defects are more likely to remain open [44]. Furthermore, more in-depth studies are needed to better clarify this intriguing finding [45].
Author Contributions
Study design, writing and original draft preparation, P.P.B.; writing, review, and editing, G.C., M.D., A.R.M.; supervision and final approval of submission G.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the University of Cagliari (PG/2015/1859).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the research, as per Italian Law.
Data Availability Statement
With the corresponding author. Available on request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rao, P.S. Management of Congenital Heart Disease: State of the Art; Part I—ACYANOTIC Heart Defects. Children 2019, 6, 42. [Google Scholar] [CrossRef]
- Bassareo, P.P.; Saba, L.; Solla, P.; Barbanti, C.; Marras, A.R.; Mercuro, G. Factors influencing adaptation and performance at physical exercise in complex congenital heart diseases after surgical repair. BioMed Res. Int. 2014, 2014, 862372. [Google Scholar] [CrossRef] [PubMed]
- Dakkak, W.; Oliver, T.I. Ventricular Septal Defect. 8 June 2021. In StatPearls Internet. Treasure Island (FL); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Bassareo, P.P.; Marras, A.R.; Mercuro, G. Ventricular septal defect in a child with Alport syndrome. BMC Cardiovasc. Disord. 2010, 10, 48. [Google Scholar] [CrossRef] [PubMed]
- Atik, S.U.; Saltik, L. Transcatheter closure of ventricular septal defect with two different devices. Cardiol. Young 2018, 28, 1364–1366. [Google Scholar] [CrossRef] [PubMed]
- Siufflet, V.; Van de Bruaene, A.; Troost, E.; Gewillig, M.; Moons, P.; Post, M.C.; Budts, W. Behaviour of unrepaired perimembranous ventricular septal defect in young adults. Am. J. Cardiol. 2010, 105, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, G.F.; Shah, M.D.; Kantor, P.F.; Rossano, J.W.; Shaddy, R.E.; Chiou, K.; Hanna, J.; Hagan, J.L.; Cabrera, A.G.; Jeewa, A.; et al. Prevalence and Severity of Anemia in Children Hospitalized with Acute Heart Failure. Congenit. Heart Dis. 2016, 11, 622–629. [Google Scholar] [CrossRef]
- Sarwar, S.; Ehsan, F.; Tahir, A.; Jamil, M.; Sahid, S.U.; Hasnain, S.; Khan, A.; Hyder, S.N. Hematological and demographic profile of Pakistani children with isolated ventricular septal defects (VSDs). Egypt. J. Med. Hum. Genet. 2020, 21, 36. [Google Scholar] [CrossRef]
- Dimopoulos, K.; Diller, G.P.; Giannakoulas, G.; Petraco, R.; Chamaidi, A.; Karaoli, E.; Mullen, M.; Swan, L.; Piepoli, M.F.; Poole-Wilson, P.A.; et al. Anemia in adults with congenital heart disease relates to adverse outcome. J. Am. Coll. Cardiol. 2009, 54, 2093–2100. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, T.L.; Hansen, E.; Olesen, H. Reference intervals for haemoglobins estimated by isoelectric focusing. Scand. J. Clin. Lab. Investig. 1982, 42, 119–122. [Google Scholar] [CrossRef]
- Messmer, K. Dependance of Oxygen Delivery on Hematocrit. In Oxygen Transport to Tissue XVI. Advances in Experimental Medicine and Biology; Hogan, M.C., Mathieu-Costello, O., Poole, D.C., Wagner, P.D., Eds.; Springer: Boston, MA, USA, 1994; Volume 361, pp. 379–380. [Google Scholar]
- Gould, I.G.; Linninger, A.A. Hematocrit distribution and tissue oxygenation in large microcirculatory networks. Microcirculation 2015, 22, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Pritišanac, E.; Urlesberger, B.; Schwaberger, B.; Pichler, G. Accuracy of Pulse Oximetry in the Presence of Fetal Hemoglobin—A Systematic Review. Children 2021, 8, 361. [Google Scholar] [CrossRef]
- Bonafide, C.P.; Localio, A.R.; Ferro, D.F.; Orenstein, E.W.; Jamison, D.T.; Lavanchy, C.; Foglia, E.E. Accuracy of Pulse Oximetry-Based Home Baby Monitors. JAMA 2018, 320, 717–719. [Google Scholar] [CrossRef]
- Canaschella, C. Iron-deficiency anemia. N. Engl. J. Med. 2015, 372, 1832–1843. [Google Scholar] [CrossRef]
- Chricton, R.R.; Charloteaux-Wauters, M. Iron transport and storage. Eur. J. Biochem. 1987, 164, 485–506. [Google Scholar] [CrossRef]
- Farrugia, A. Albumin usage in clinical medicine: Tradition or therapeutic? Transfus. Med. Rev. 2010, 24, 53–63. [Google Scholar] [CrossRef]
- Granzotti, J.A.; Falha, S.L.; Nunes, M.D. Nutritional index in heart diseases in childhood. Arq. Bras. Cardiol. 1990, 55, 371–373. [Google Scholar]
- Anderson, R.H.; Lenox, C.C.; Zuberbuhler, J.R. Mechanisms of closure of perimembranous ventricular septal defect. Am. J. Cardiol. 1983, 52, 341–345. [Google Scholar] [CrossRef]
- Lopez, L.; Houyel, L.; Colan, S.D.; Anderson, R.H.; Béland, M.J.; Aiello, V.D.; Bailliard, F.; Cohen, M.S.; Jacobs, J.P.; Kurosawa, H.; et al. Classification of Ventricular Septal Defects for the Eleventh Iteration of the International Classification of Diseases-Striving for Consensus: A report from the International Society for Nomenclature of Paediatric and Congenital Heart Disease. Ann. Thorac. Surg. 2018, 106, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ko, J.M.; Guileyardo, J.M.; Roberts, W.C. A review of spontaneous closure of ventricular septal defect. Bayl. Univ. Med. Cent. Proc. 2015, 28, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Mercuro, G.; Bassareo, P.P.; Mariucci, E.; Deidda, M.; Zedda, A.M.; Bonvicini, M. Sex differences in congenital heart defects and genetically induced arrhythmias. J. Cardiovasc. Med. 2014, 15, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Liu, J.; Wang, J.; Liu, M.; Xu, H.; Yang, S. Factors influencing the spontaneous closure of ventricular septal defect in infants. Int. J. Clin. Exp. Pathol. 2015, 8, 5614–5623. [Google Scholar]
- Khan, Z.; Natarajan, G.; Sallaam, S.; Bondarenko, I.; Walters, H.L.; Delius, R.; Aggarwal, S. Association between anemia and packed cell transfusion and outcomes of ventricular septal defect and atrioventricular canal repair in children. Pediatr. Cardiol. 2014, 35, 471–478. [Google Scholar] [CrossRef]
- Hansen, E.S.; Wethelund, J.O.; Skajaa, K. Wound healing after leg and thigh amputation for arteriosclerotic and diabetic gangrene. The significance of preoperative and postoperative hemoglobin and hematocrit values. Ugeskr. Laeger 1987, 149, 2387–2390. [Google Scholar]
- Helg, F.; Hunt, F. Hemoglobin spray as adjunct therapy in complex wounds: Meta-analysis versus standard care alone in pooled data by wound type across three retrospective cohort controlled evaluations. SAGE Open Med. 2018, 6, 2050312118784313. [Google Scholar]
- Ho, C.H. Relationship between blood cells and blood viscosity. Am. J. Hematol. 2004, 75, 264. [Google Scholar] [CrossRef]
- Kontras, S.B.; Bodenbender, J.G.; Craenen, J.; Hosier, D.M. Hyperviscosity in congenital heart disease. J. Pediatr. 1970, 76, 214–220. [Google Scholar] [CrossRef]
- Black, S.M.; Field-Ridley, A.; Sharma, S.; Kumar, S.; Keller, R.L.; Kameny, R.; Maltepe, E.; Datar, S.A.; Fineman, J.R. Altered carnitine homeostasis in children with increased pulmonary blood flow due to ventricular septal defects. Pediatr. Crit. Care Med. 2017, 18, 931–934. [Google Scholar] [CrossRef] [PubMed]
- Cao, A.; Rosatelli, C.; Pirastu, M.; Galanello, R. Thalassemias in Sardinia: Molecular pathology, phenotype-genotype correlation, and prevention. Am. J. Pediatr. Hematol. Oncol. 1991, 13, 179–188. [Google Scholar] [CrossRef] [PubMed][Green Version]
- López-Ruzafa, E.; Vázquez-López, M.A.; Galera-Martínez, R.; Lendínez-Molinos, F.; Gómez-Bueno, S.; Martín-González, M. Prevalence and associated factors of iron deficiency in Spanish children aged 1 to 11 years. Eur. J. Pediatr. 2021, 180, 2773–2780. [Google Scholar] [CrossRef] [PubMed]
- Kempny, A.; Diller, G.P.; Alonso-Gonzalez, R.; Uebing, A.; Rafiq, I.; Li, W.; Swan, L.; Hooper, J.; Donovan, J.; Wort, S.J.; et al. Hypoalbuminaemia predicts outcome in adult patients with congenital heart disease. Heart 2015, 101, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Uthamalingam, S.; Kandala, J.; Daley, M.; Patvardhan, E.; Capodilupo, R.; Moore, S.A.; Januzzi, J.L., Jr. Serum albumin and mortality in acutely decompensated heart failure. Am. Heart J. 2010, 160, 1149–1155. [Google Scholar] [CrossRef]
- Slodki, S.J.; Bronski, D. Serum protein in cyanotic and acyanotic congenital heart disease. Am. Heart J. 1964, 68, 316–319. [Google Scholar] [CrossRef]
- Kobayashi, N.; Nagai, H.; Yasuda, Y.; Kanazawa, K. The early influence of albumin administration on protein metabolism and wound healing in burned rats. Wound Repair Regen. 2004, 12, 109–114. [Google Scholar] [CrossRef]
- Felcher, A.; Schwartz, J.; Shechter, C.; Levenson, S.M.; Demetriou, A.A. Wound healing in normal and analbuminemic (NAR) rats. J. Surg. Res. 1987, 43, 546–549. [Google Scholar] [CrossRef]
- Butera, G.; Piazza, L.; Saracino, A.; Chessa, M.; Carminati, M. Transcatheter Closure of Membranous Ventricular Septal Defects-Old Problems and New Solutions. Interv. Cardiol. Clin. 2013, 2, 85–91. [Google Scholar] [CrossRef]
- Lewis, C.J.; Stevenson, A.; Fear, M.W.; Wood, F.M. A review of epigenetic regulation in wound healing: Implications for the future of wound care. Wound Repair. Regen. 2020, 28, 710–718. [Google Scholar] [CrossRef]
- Sarajlic, P.; Simonsson, M.; Jernberg, T.; Bäck, M.; Hofmann, R. Incidence, associated outcomes, and predictors of upper gastrointestinal bleeding following acute myocardial infarction: A Swedeheart-based nationwide cohort study. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 23, pvab059. [Google Scholar] [CrossRef]
- Sarajlic, P.; Plunde, O.; Franco-Cereceda, A.; Bäck, M. Artificial Intelligence Models Reveal Sex-Specific Gene Expression in Aortic Valve Calcification. JACC Basic Transl. Sci. 2021, 6, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.K.; Kochilas, L.K.; Knight, J.; McCracken, C.; Thomas, A.S.; Moller, J.H.; Setty, S.P. Long-Term Survival and Causes of Death in Children with Trisomy 21 After Congenital Heart Surgery. J. Pediatr. 2021, 231, 246–253.e3. [Google Scholar] [CrossRef]
- David, O.; Fiorucci, G.C.; Tosi, M.T.; Altare, F.; Valori, A.; Saracco, P.; Asinardi, P.; Ramenghi, U.; Gabutti, V. Hematological studies in children with Down syndrome. Pediatr. Hematol. Oncol. 1996, 13, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Sun, K.; Chen, S.; Yao, L.; Zhang, Y. A new scoring system for spontaneous closure prediction of perimembranous ventricular septal defects in children. PLoS ONE 2014, 9, e113822. [Google Scholar] [CrossRef] [PubMed]
- Li, J.J.; Liu, Y.; Xie, S.Y.; Zhao, G.D.; Dai, T.; Chen, H.; Mu, L.F.; Qi, H.Y.; Li, J. Newborn screening for congenital heart disease using echocardiography and follow-up at high altitude in China. Int. J. Cardiol. 2019, 274, 106–112. [Google Scholar] [CrossRef]
- Sayers, D.R.; Witkop, C.T.; Webber, B.J. Impact of Altitude-based Hemoglobin Modification on Pediatric Iron Deficiency Anemia Screening. J. Pediatr. 2020, 221, 196–200. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).