
Forced Oscillation Technique for Monitoring the Respiratory Status of Children with Cystic Fibrosis: A Systematic Review


Abstract
1. Introduction
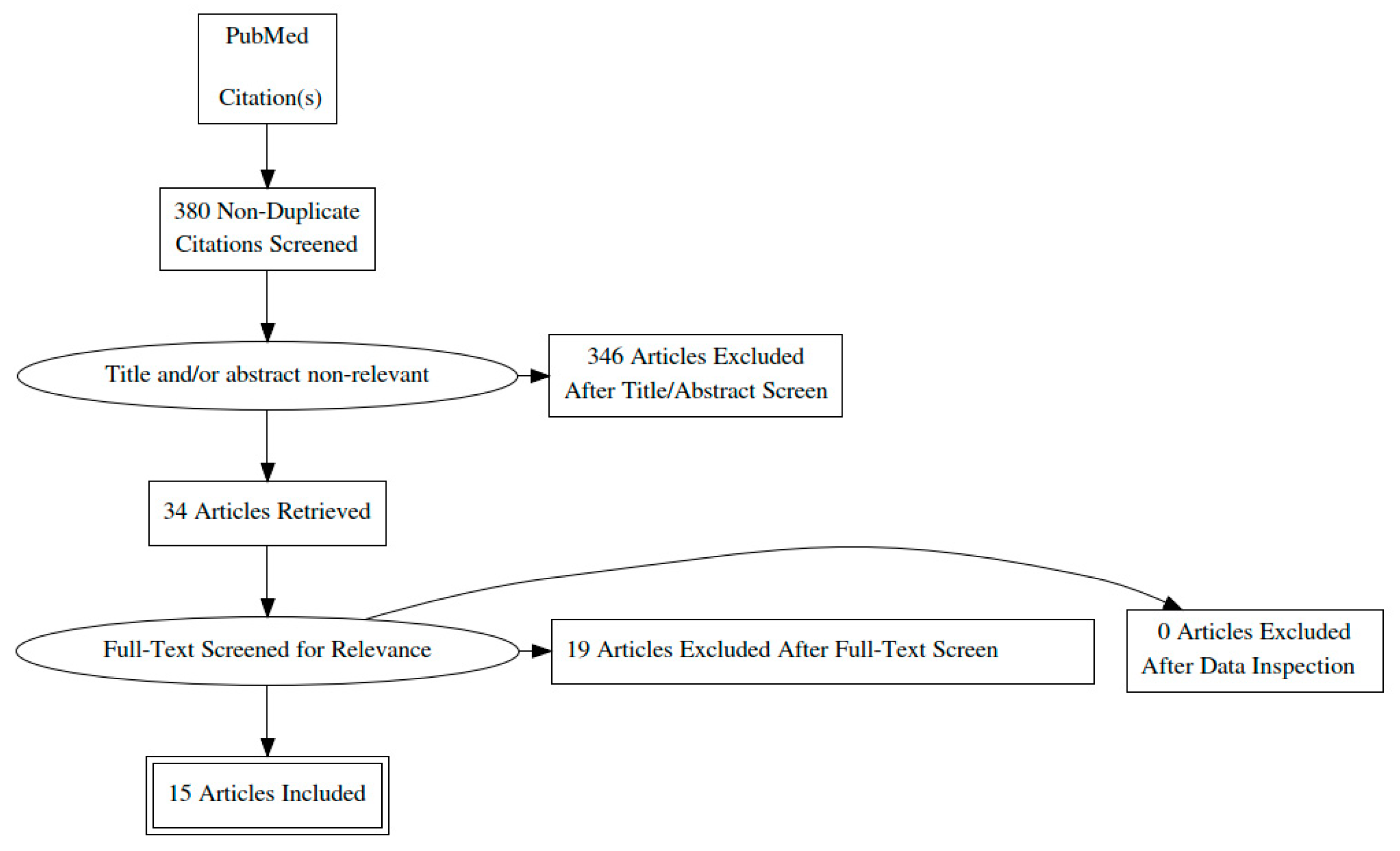
2. Methods
3. Result
3.1. Forced Oscillation Technique-Background
3.2. Feasibility and Reliability
3.3. Correlation of Oscillometry and Spirometry Values in Children with Cystic Fibrosis
3.4. Distinguishing Subjects with Cystic Fibrosis from Healthy Controls by Oscillometry
3.5. Oscillometry and Its Association with the Clinical Condition in Subjects with CF
3.6. Oscillometry and Its Association with Pulmonary Inflammation, Infection, and Structural Lung Disease, in Subjects with CF
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
| Author | Year | Main Outcome Measures | Main Recorded Parameters | |
|---|---|---|---|---|
| Studies on feasibility and reliability of FOT in children with CF | ||||
| 1a | Kerby G | 2011 | Feasibility and short term reproducibility of oscillometry | Rrs and Xrs at 4, 6, 8 and 10 Hz |
| 2 | Wamosy RMG | 2021 | Assessment within trial reliability of 3 measures in IOS parameters. | Rrs at 5 and 20 Hz, Zr at 5 Hz, Xr at 5 Hz |
| 3a | Gangell C.L | 2007 | Evaluation of between measurement repeatability of oscillometry | Zrs, Rrs and Xrs at 6, 8 and 10 Hz |
| Studies on correlation between oscillometry and spirometry values | ||||
| 4 | Lebeque P | 1997 | Evaluation of Rrs to detect airway obstruction in patients with CF and in patients with bronchial asthma | Rrs at 10 Hz |
| 5 | Nielsen K | 2004 | Assessment of the usefulness of IOS in the evaluation of lung function | Rrs at 5 and 20 Hz, Xrs at 5 Hz, Zrs at 5 Hz |
| 6 | Moreau L | 2009 | Assessment of IOS values to quantify lung function impairment in relation to the respective spirometric indices at a cross sectional and longitudinal level | Rrs, Xrs, Zrs at 5 Hz |
| 7 | Raj D | 2014 | Evaluation of IOS utility for the detection of airway obstruction and its correlation with spirometric indices | Rrs at 5 and 20 Hz, Zrs, XRs at 5 Hz |
| 8 | Zannin E | 2019 | Evaluation of the relationship of FOT parameters with other lung function indices such as spirometry | Zrs at 8 Hz |
| 9a | Ozturk K | 2021 | Evaluation of the relationship of FOT parameters with spirometry values | Rrs and Xrs at 5, 10 and 20 Hz |
| Studies on the discrimination of subjects with CF from healthy subjects based on IOS values | ||||
| 10 | Cogswell J.J | 1973 | The use of oscillation technique in the evaluation of healthy children and in those with obstructive airway disease (asthma or cystic fibrosis) | Forced oscillation applying a sine wave frequency from 5–7 Hz. |
| 11 | Solymar L | 1985 | The use of oscillation technique in the evaluation of healthy children and in those with cricoid stenosis, cystic fibrosis or asthma | Rrs, Xrs and Zrs at 2, 4, 12 Hz |
| 1b | Kerby | 2011 | Comparison of the ability of the technique to differentiate patients with CF from healthy controls | Rrs and Xrs at 4, 6, 8 and 10 Hz |
| Studies on the correlation of clinical condition with oscillometry values | ||||
| 12 | Ren C.L | 2011 | Correlation between clinical features of CF patients with oscillometry indices and other lung function tests | Rrs and Xrs at 4, 6, 8 and 10 Hz |
| 13 | Buchs C | 2015 | Evaluation of oscilometry responsiveness properties in children with CF while on acute exacerbation, prior and following intravenous antibiotic treatment | Rrs and Xrs at 5, 10, 15 and 20 Hz. |
| 3b | Gangell C.L | 2007 | Oscillometry values in symptomatic and asymptomatic children with CF | Zrs, Rrs and Xrs at 6, 8 and 10 Hz |
| 9b | Ozturk K | 2021 | Evaluation of the relationship of FOT parameters with clinical scores | Rrs and Xrs at 5, 10 and 20 Hz |
| Studies on the correlation of oscilometry values with pulmonary inflammation, infection and structural changes | ||||
| 14 | Brennan S | 2005 | Evaluation of the correlation of inflammation and infection detected in BAL fluid with lung function including oscillometry | Zrs after applying a broadband forcing signal 0.5–20 Hz. |
| 15 | Ramsey K | 2015 | Assessment of the association between inflammation, infection and structural lung disease with oscillometry values | Rrs and Xrs at 8 Hz. |
References
- Szczesniak, R.; Heltshe, S.L.; Stanojevic, S.; Mayer-Hamblett, N. Use of FEV(1) in cystic fibrosis epidemiologic studies and clinical trials: A statistical perspective for the clinical researcher. J. Cystic Fibrosis Off. J. Eur. Cystic Fibrosis Soc. 2017, 16, 318–326. [Google Scholar] [CrossRef]
- Breuer, O.; Caudri, D.; Stick, S.; Turkovic, L. Predicting disease progression in cystic fibrosis. Expert Rev. Respir. Med. 2018, 12, 905–917. [Google Scholar] [CrossRef]
- Skylogianni, E.; Douros, K.; Anthracopoulos, M.B.; Fouzas, S. The Forced Oscillation Technique in Paediatric Respiratory Practice. Paediatr. Respir. Rev. 2016, 18, 46–51. [Google Scholar] [CrossRef]
- Fretzayas, A.; Douros, K.; Moustaki, M.; Loukou, I. Applications of lung clearance index in monitoring children with cystic fibrosis. World J. Clin. Pediatr. 2019, 8, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Sachdev, A.; Gupta, D. Oscillometry-A reasonable option to monitor lung functions in the era of COVID-19 pandemic. Pediatr. Pulmonol. 2021, 56, 14–15. [Google Scholar] [CrossRef] [PubMed]
- Dubois, A.B.; Brody, A.W.; Lewis, D.H.; Burgess, B.F., Jr. Oscillation mechanics of lungs and chest in man. J. Appl. Physiol. 1956, 8, 587–594. [Google Scholar] [CrossRef] [PubMed]
- King, G.G.; Bates, J.; Berger, K.I.; Calverley, P.; de Melo, P.L.; Dellacà, R.L.; Farré, R.; Hall, G.L.; Ioan, I.; Irvin, C.G.; et al. Technical standards for respiratory oscillometry. Eur. Respir. J. 2020, 55, 1900753. [Google Scholar] [CrossRef]
- Bickel, S.; Popler, J.; Lesnick, B.; Eid, N. Impulse oscillometry: Interpretation and practical applications. Chest 2014, 146, 841–847. [Google Scholar] [CrossRef]
- de Oliveira Jorge, P.P.; de Lima, J.H.P.; Chong, E.S.D.C.; Medeiros, D.; Solé, D.; Wandalsen, G.F. Impulse oscillometry in the assessment of children’s lung function. Allergol. Immunopathol. 2019, 47, 295–302. [Google Scholar] [CrossRef]
- Hall, G.L.; Sly, P.D.; Fukushima, T.; Kusel, M.M.; Franklin, P.J.; Horak, F., Jr.; Patterson, H.; Gangell, C.; Stick, S.M. Respiratory function in healthy young children using forced oscillations. Thorax 2007, 62, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Kerby, G.S.; Rosenfeld, M.; Ren, C.L.; Mayer, O.H.; Brumback, L.; Castile, R.; Hart, M.A.; Hiatt, P.; Kloster, M.; Johnson, R.; et al. Lung function distinguishes preschool children with CF from healthy controls in a multi-center setting. Pediatr. Pulmonol. 2012, 47, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Wamosy, R.M.G.; Assumpção, M.S.; Parazzi, P.L.F.; Ribeiro, J.D.; Roesler, H.; Schivinski, C.I.S. Reliability of impulse oscillometry parameters in healthy children and in children with cystic fibrosis. Int. J. Clin. Pract. 2021, 75, e13715. [Google Scholar] [CrossRef] [PubMed]
- Gangell, C.L.; Horak, F., Jr.; Patterson, H.J.; Sly, P.D.; Stick, S.M.; Hall, G.L. Respiratory impedance in children with cystic fibrosis using forced oscillations in clinic. Eur. Respir. J. 2007, 30, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Lebecque, P.; Stănescu, D. Respiratory resistance by the forced oscillation technique in asthmatic children and cystic fibrosis patients. Eur. Respir. J. 1997, 10, 891–895. [Google Scholar]
- Nielsen, K.G.; Pressler, T.; Klug, B.; Koch, C.; Bisgaard, H. Serial lung function and responsiveness in cystic fibrosis during early childhood. Am. J. Respir. Crit. Care Med. 2004, 169, 1209–1216. [Google Scholar] [CrossRef]
- Moreau, L.; Crenesse, D.; Berthier, F.; Albertini, M. Relationship between impulse oscillometry and spirometric indices in cystic fibrosis children. Acta Paediatr. 2009, 98, 1019–1023. [Google Scholar] [CrossRef]
- Raj, D.; Sharma, G.K.; Lodha, R.; Kabra, S.K. Correlation between impulse oscillometry and spirometry parameters in Indian patients with cystic fibrosis. Chron. Respir. Dis. 2014, 11, 139–149. [Google Scholar] [CrossRef]
- Zannin, E.; Nyilas, S.; Ramsey, K.A.; Latzin, P.; Dellaca, R.L. Within-breath changes in respiratory system impedance in children with cystic fibrosis. Pediatr. Pulmonol. 2019, 54, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Kartal Öztürk, G.; Eşki, A.; Gülen, F.; Demir, E. Is Impulse Oscillometry System a Useful Method for the Evaluation and Follow-Up of Patients with Cystic Fibrosis? Pediatr. Allergy Immunol. Pulmonol. 2021, 34, 15–22. [Google Scholar] [CrossRef]
- Cogswell, J.J. Forced oscillation technique for determination of resistance to breathing in children. Arch. Dis. Child. 1973, 48, 259–266. [Google Scholar] [CrossRef][Green Version]
- Solymar, L.; Aronsson, P.H.; Sixt, R. The forced oscillation technique in children with respiratory disease. Pediatr. Pulmonol. 1985, 1, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.L.; Brucker, J.L.; Rovitelli, A.K.; Bordeaux, K.A. Changes in lung function measured by spirometry and the forced oscillation technique in cystic fibrosis patients undergoing treatment for respiratory tract exacerbation. Pediatr. Pulmonol. 2006, 41, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Buchs, C.; Coutier, L.; Vrielynck, S.; Jubin, V.; Mainguy, C.; Reix, P. An impulse oscillometry system is less efficient than spirometry in tracking lung function improvements after intravenous antibiotic therapy in pediatric patients with cystic fibrosis. Pediatr. Pulmonol. 2015, 50, 1073–1081. [Google Scholar] [CrossRef]
- Brennan, S.; Hall, G.L.; Horak, F.; Moeller, A.; Pitrez, P.M.; Franzmann, A.; Turner, S.; de Klerk, N.; Franklin, P.; Winfield, K.R.; et al. Correlation of forced oscillation technique in preschool children with cystic fibrosis with pulmonary inflammation. Thorax 2005, 60, 159–163. [Google Scholar] [CrossRef]
- Ramsey, K.A.; Ranganathan, S.C.; Gangell, C.L.; Turkovic, L.; Park, J.; Skoric, B.; Stick, S.M.; Sly, P.D.; Hall, G.L. Impact of lung disease on respiratory impedance in young children with cystic fibrosis. Eur. Respir. J. 2015, 46, 1672–1679. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loukou, I.; Moustaki, M.; Deligianni, A.; Sardeli, O.; Douros, K. Forced Oscillation Technique for Monitoring the Respiratory Status of Children with Cystic Fibrosis: A Systematic Review. Children 2021, 8, 857. https://doi.org/10.3390/children8100857
Loukou I, Moustaki M, Deligianni A, Sardeli O, Douros K. Forced Oscillation Technique for Monitoring the Respiratory Status of Children with Cystic Fibrosis: A Systematic Review. Children. 2021; 8(10):857. https://doi.org/10.3390/children8100857
Chicago/Turabian StyleLoukou, Ioanna, Maria Moustaki, Agni Deligianni, Olympia Sardeli, and Konstantinos Douros. 2021. "Forced Oscillation Technique for Monitoring the Respiratory Status of Children with Cystic Fibrosis: A Systematic Review" Children 8, no. 10: 857. https://doi.org/10.3390/children8100857
APA StyleLoukou, I., Moustaki, M., Deligianni, A., Sardeli, O., & Douros, K. (2021). Forced Oscillation Technique for Monitoring the Respiratory Status of Children with Cystic Fibrosis: A Systematic Review. Children, 8(10), 857. https://doi.org/10.3390/children8100857