A Group Parenting Intervention for Depressed Fathers (LTP + Dads): A Feasibility Study from Pakistan



 ,
,
Abstract
1. Introduction
2. Methods
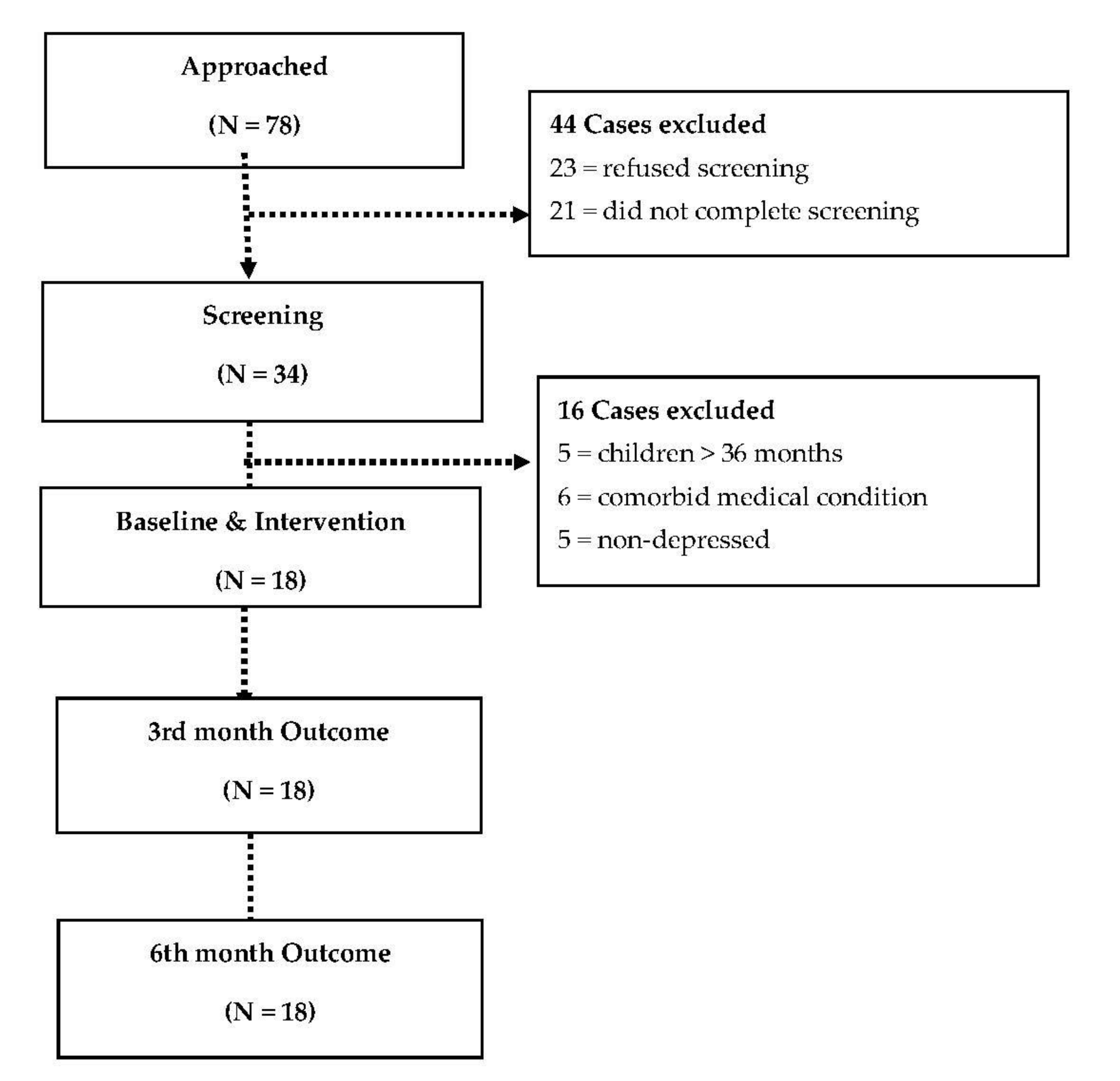
2.1. Participants
2.2. Intervention: Learning through Play+ Dads (LTP+ Dads)
2.3. Primary Feasibility Measures
3. Measures
4. Analysis
5. Ethical Approval
6. Results
7. Discussion
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Friedrich, M.J. Depression is the leading cause of disability around the world. JAMA 2017, 317, 1517. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Depression & Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerlands, 2017. [Google Scholar]
- Lovejoy, M.C.; Graczyk, P.A.; O’Hare, E.; Neuman, G. Maternal depression and parenting behavior: A meta-analytic review. Clin. Psychol. Rev. 2000, 20, 561–592. [Google Scholar] [CrossRef]
- Jeong, J.; Pitchik, H.O.; Yousafzai, A.K. Stimulation interventions and parenting in low-and middle-income countries: A meta-analysis. Pediatrics 2018, 141, e20173510. [Google Scholar] [CrossRef]
- Husain, N.; Zulqernain, F.; Carter, L.A.; Chaudhry, I.B.; Fatima, B.; Kiran, T.; Haq, S.U. Treatment of maternal depression in urban slums of Karachi, Pakistan: A randomized controlled trial (RCT) of an integrated maternal psychological and early child development intervention. Asian J. Psychiatry 2017, 29, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Gadit, A.A.M.; Mugford, G. Prevalence of depression among households in three capital cities of Pakistan: Need to revise the mental health policy. PLoS ONE 2007, 2, e209. [Google Scholar] [CrossRef]
- Husain, N. Depressive disorder and social stress in Pakistan compared to people of Pakistani origin in the UK. Soc. Psychiatry Psychiat. Epidemiol. 2011, 46, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Husain, N.; Parveen, A.; Husain, M.; Saeed, Q.; Jafri, F.; Rahman, R.; Tomenson, B.; Chaudhry, I.B. Prevalence and psychosocial correlates of perinatal depression: A cohort study from urban Pakistan. Arch. Womens Ment. Health 2011, 14, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Habib, C. Paternal perinatal depression: An overview and suggestions towards an intervention model. J. Fam. Stud. 2012, 18, 4–16. [Google Scholar] [CrossRef]
- Iqbal, M.; Fatmi, Z. Prevalence of emotional and physical intimate partner violence among married women in Pakistan. J. Int. Viol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychnol. 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.; Pelosi, A.J.; Araya, R.; Dunn, G. Measuring psychiatric disorder in the community: A standardized assessment for use by lay interviewers. Psychol. Med. 1992, 22, 465–486. [Google Scholar] [CrossRef] [PubMed]
- Ashem, B. The Learning through Play Calendar: Training Manual; The Hincks Dellcrest Centre: Toronto, ON, Canada, 2002. [Google Scholar]
- Muñoz, F.; Miranda, J. Group Therapy Manual for Cognitive-Behavioral Treatment of Depression; RAND Corporation: Santa Monica, CA, USA, 2000; Volume 1194. [Google Scholar]
- Bader, E.; Cooper, N. Focus on Father, a Management Skills Program for Fathers of Children from Birth to Six Years of Age, 2nd ed.; Family Transitions Consultants: Toronto, ON, Canada, 2003. [Google Scholar]
- Husain, N.; Afsar, S.; Ara, J.; Fayyaz, H.; ur Rahman, R.; Tomenson, B.; Hamirani, M.; Chaudhry, N.; Fatima, B.; Husain, M.; et al. Brief psychological intervention after self-harm: Randomised controlled trial from Pakistan. Br. J. Psychiatry 2014, 204, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Lovell, K.; Lunat, F.; Masood, Y.; Shah, S.; Tomenson, B.; Husain, N. Culturally-adapted cognitive behavioural therapy based intervention for maternal depression: A mixed-methods feasibility study. BMC Womens Health 2019, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Edmondson, O.J.H.; Psychogiou, L.; Vlachos, H.; Netsi, E.; Ramchandani, P.G. Depression in fathers in the postnatal period: Assessment of the Edinburgh Postnatal Depression Scale as a screening measure. J. Affect. Disord. 2010, 125, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Haskett, M.E.; Ahern, L.S.; Ward, C.S.; Allaire, J.C. Factor structure and validity of the parenting stress index-short form. J. Clin. Child Adolesc. Psychol. 2006, 35, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Von Korff, M.; Ustun, T.B.; Ormel, J.; Kaplan, I.; Simon, G.E. Self-report disability in an international primary care study of psychological illness. J. Clin. Epidemiol. 1996, 49, 297–303. [Google Scholar] [CrossRef]
- Brooks, R.; EuroQol Group. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]


{kind=link}
| Personal and Household Characteristics | |
|---|---|
| Mean (SD) | |
| Father age | 33.11 (8.49) |
| Monthly income (Pakistani rupees) | 9083.33 (5018.35) |
| Number of children | 3.61 (2.23) |
| Frequency (%) | |
| Household members | |
| Nuclear family | 8 (44.44%) |
| Extended family (three or more generations in the same household) | 10 (55.56%) |
| Educational level Below primary (Less than 5 years) | 9 (50.00) |
| Primary to metric (up to 10 years of education) | 7 (38.89) |
| Above metric (more than 10 years of education) | 2 (11.11) |
| Current employment | 5 (27.78) |
| Loss of a child | 7 (38.89) |
| Financial debt | 8 (44.44) |
| Outcome | Baseline (0 Month) | Post-Intervention (3 Months) | Follow-Up (6 Months) |
|---|---|---|---|
| Mean [SD] | Mean [SD] | Mean [SD] | |
| EPDS | 14.17 [2.18] | 7.00 [3.51] | 6.06 [2.13] |
| HAM-D | 16.44 [2.66] | 11.33 [3.66] | 9.89 [3.79] |
| PSI | 91.17 [15.03] | 79.67 [10.54] | 73.61 [8.58] |
| KAP: Sense of Self | 21.06 [3.21] | 22.28 [1.67] | 23.53 [1.94] a |
| KAP: Physical Development | 19.28 [1.41] | 19.17 [1.58] | 20.76 [1.75] a |
| KAP: Relationships | 21.06 [1.30] | 21.11 [1.41] | 22.76 [1.09] a |
| KAP: Understanding of the World | 16.83 [2.62] | 18.22 [1.22] | 19.41 [1.28] a |
| KAP Communication | 16.83 [1.62] | 17.61 [1.20] | 18.18 [1.07] a |
| SES | 18.33 [3.03] | 19.78 [1.73] | 20.28 [2.30] |
| MSPSS | 34.28 [11.67] | 56.89 [14.00] | 55.00 [7.67] |
| BDQ | 9.67 [4.42] | 4.78 [2.65] | 3.89 [1.45] |
| EQ-5D VAS score | 40.28 [14.89] | 59.17 [8.45] | 59.44 [4.50] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husain, M.I.; Chaudhry, I.B.; Khoso, A.B.; Wan, M.W.; Kiran, T.; Shiri, T.; Chaudhry, N.; Mehmood, N.; Jafri, S.F.; Naeem, F.; et al. A Group Parenting Intervention for Depressed Fathers (LTP + Dads): A Feasibility Study from Pakistan. Children 2021, 8, 26. https://doi.org/10.3390/children8010026
Husain MI, Chaudhry IB, Khoso AB, Wan MW, Kiran T, Shiri T, Chaudhry N, Mehmood N, Jafri SF, Naeem F, et al. A Group Parenting Intervention for Depressed Fathers (LTP + Dads): A Feasibility Study from Pakistan. Children. 2021; 8(1):26. https://doi.org/10.3390/children8010026
Chicago/Turabian StyleHusain, Muhammad I., Imran B. Chaudhry, Ameer B. Khoso, Ming W. Wan, Tayyeba Kiran, Tinevimbo Shiri, Nasim Chaudhry, Nasir Mehmood, Syed F. Jafri, Farooq Naeem, and et al. 2021. "A Group Parenting Intervention for Depressed Fathers (LTP + Dads): A Feasibility Study from Pakistan" Children 8, no. 1: 26. https://doi.org/10.3390/children8010026
APA StyleHusain, M. I., Chaudhry, I. B., Khoso, A. B., Wan, M. W., Kiran, T., Shiri, T., Chaudhry, N., Mehmood, N., Jafri, S. F., Naeem, F., & Husain, N. (2021). A Group Parenting Intervention for Depressed Fathers (LTP + Dads): A Feasibility Study from Pakistan. Children, 8(1), 26. https://doi.org/10.3390/children8010026