Characterization of Pediatric Seizures in the Commonwealth of the Northern Mariana Islands


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Febrile Seizures
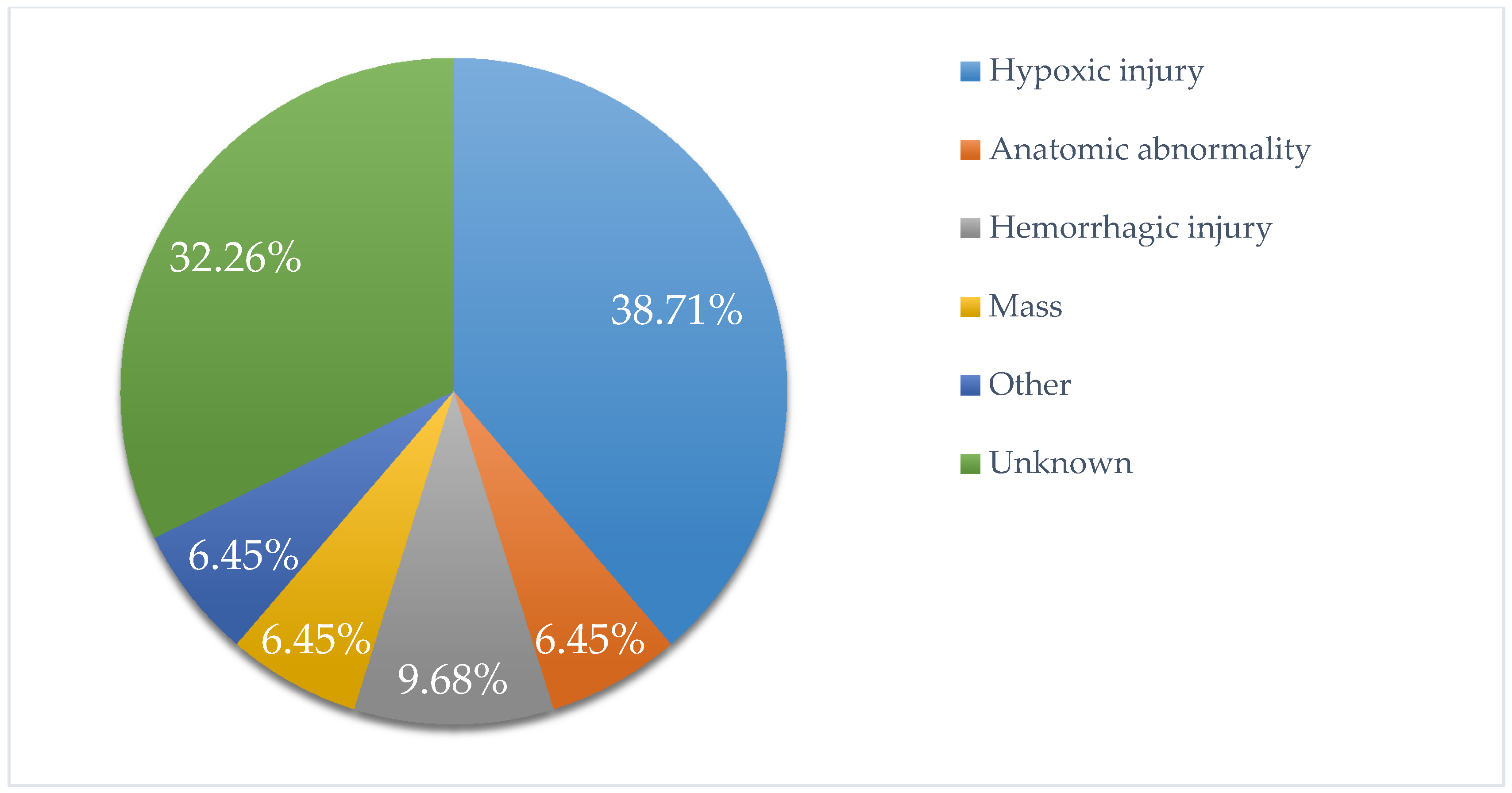
3.2. Non-Febrile Seizures
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Central Intelligence Agency. Available online: https://www.cia.gov/library/publications/the-world-factbook/geos/print_cq.html (accessed on 2 March 2019).
- Stanhope, J.M.; Brody, J.A.; Brink, E. Convulsions amongst the Chamorro People of Guam, Mariana Islands: I. Seizure Disorders. Am. J. Epidemiol. 1972, 95, 292–298. [Google Scholar] [CrossRef]
- World Health Organization, Regional Office for the Western Pacific. Epilepsy in the Western Pacific Region: A Call to Action: Global Campaign against Epilepsy; WHO Regional Office for the Western Pacific: Manila, Phillipines, 2004; pp. 9–10. [Google Scholar]
- Steering Committee on Quality Improvement and Management, Subcommittee on Febrile Seizures. Febrile Seizures: Clinical Practice Guideline for the Long-term Management of the Child with Simple Febrile Seizures. Pediatrics 2008, 121, 1281–1286. [Google Scholar] [CrossRef]
- International League against Epilepsy. Available online: https://www.ilae.org/guidelines/definition-and-classification/the-2014-definition-of-epilepsy-a-perspective-for-patients-and-caregivers (accessed on 13 March 2019).
- Leung, A.K.; Hon, K.L.; Leung, T.N. Febrile Seizures: An overview. Drugs Context 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, A.; Fujinami, R.S.; White, H.S.; Preux, P.M.; Blümcke, I.; Sander, J.W.; Löscher, W. Infections, inflammation and epilepsy. Acta Neuropathol. 2016, 131, 211–234. [Google Scholar] [CrossRef]
- Camfield, P.; Camfield, C. Incidence, prevalence and aetiology of seizures and epilepsy in children. Epileptic Disord. 2015, 117, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Cowan, L.D. The epidemiology of the epilepsies in children. Ment. Retard. Dev. Disabil. Res. Rev. 2002, 8, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Tekgul, H.; Gauvreau, K.; Soul, J.; Mursphy, L.; Robertson, R.; Stewart, J.; Volpe, J.; Bourgeois, B.; du Plessis, A.J. The Current Etiologic Profile and Neurodevelopmental Outcome of Seizures in Term Newborn Infants. Pediatrics 2006, 117, 1270–1280. [Google Scholar] [CrossRef]
- De Bittencourt, P.R.M.; Adamolekum, B.; Bharucha, N.; Carpio, A.; Cossío, O.H.; Danesi, M.A.; Dumas, M.; Meinardi, H.; Ordinario, A.; Senanayake, N.; et al. Epilepsy in the Tropics: I. Epidemiology, Socioeconomic Risk Factors, and Etiology. Epilepsia 1996, 37, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Hirtz, D.; Ashwal, S.; Berg, A.; Bettis, D.; Camfield, C.; Camfield, P.; Crumrine, P.; Elterman, R.; Schneider, S.; Shinnar, S. Practice parameter: Evaluating a first nonfebrile seizure in children: Report of the Quality Standards Subcommittee of the American Academy of Neurology, the Child Neurology Society, and the American Epilepsy Society. Neurology 2000, 55, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Shellhaas, R.A.; Chang, T.; Tsuchida, T.; Scher, M.S.; Riviello, J.J.; Abend, N.S.; Nguyen, S.; Wusthoff, C.J.; Clancy, R.R. The American Clinical Neurophysiology Society’s Guideline on Continuous Electroencephalography Monitoring in Neonates. J. Clin. Neurophysiol. 2011, 28, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, W.D.; Chiron, C.; Cross, J.H.; Harvey, A.S.; Kuzniecky, R.; Hertz-Pannier, L.; Vezina, L.G. Guidelines for imaging infants and children with recent-onset epilepsy. Epilepsia 2009, 50, 2147–2153. [Google Scholar] [CrossRef] [PubMed]
- Lenkov, D.N.; Volnova, A.B.; Pope, A.R.; Tsytsarev, V. Advantages and limitations of brain imaging methods in the research of absence epilepsy in humans and animal models. J. Neurosci. Methods 2013, 212, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, L.A.; Patel, A.D.; Slaughter, J.L. Pharmacological treatment of neonatal seizures: A systematic review. J. Child Neurol. 2013, 28, 351–364. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on Neonatal Seizures; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Bittigau, P.; Sifringer, M.; Ikonomidou, C. Antiepileptic drugs and apoptosis in the developing brain. Ann. N.Y. Acad. Sci. 2003, 993, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Sulzbacher, S.; Farwell, J.R.; Temkin, N.; Lu, A.S.; Hirtz, D.G. Late cognitive effects of early treatment with phenobarbital. Clin. Pediatr. (Phila) 1999, 38, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Shellhaas, R.A.; Chang, T.; Wusthoff, C.J.; Soul, J.S.; Massey, S.L.; Chu, C.J.; Cilio, M.R.; Bonifacio, S.L.; Abend, N.S.; Tsuchida, T.N.; et al. Treatment Duration After Acute Symptomatic Seizures in Neonates: A Multicenter Cohort Study. J. Pediatr. 2017, 181, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, N.; Beatty, C.W.; Gust, J.; Hamiwka, L. Provider Practices of Phenobarbital Discontinuation in Neonatal Seizures. J. Child Neurol. 2018, 33, 153–157. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with Febrile Seizures (FS) | Patients with Non-Febrile Seizures (NFS) |
|---|---|---|
| Total, n | 101 | 31 |
| Male, n (%) | 62 (61) | 18 (58) |
| Female, n (%) | 39 (39) | 13 (42) |
| Native ethnicity or other Pacific Islander, n (%) | ||
| 41 (41) | 14 (45) | |
| Asian ethnicity, n (%) | 30 (30) | 8 (26) |
| Delivered at term, n (%) | 62 (61) | 17 (55) |
| Not delivered at term, n (%) | 13 (13) | 11 (36) |
| Categorized as simple FS, n (%) | 97 (96) | n/a |
| Categorized as complex FS, n (%) | 4 (4) | n/a |
| Modality, N (%) | Patients with Non-Febrile Seizures |
|---|---|
| EEG, n (%) | 31 (72) |
| CT, n (%) | 24 (56) |
| HUS, n (%) | 27 (38) |
| MRI, n (%) | 13 (30) |
| LP, n (%) | 7 (16) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yogesh, A.; Taylor, M.; Chang, M.P. Characterization of Pediatric Seizures in the Commonwealth of the Northern Mariana Islands. Children 2020, 7, 26. https://doi.org/10.3390/children7040026
Yogesh A, Taylor M, Chang MP. Characterization of Pediatric Seizures in the Commonwealth of the Northern Mariana Islands. Children. 2020; 7(4):26. https://doi.org/10.3390/children7040026
Chicago/Turabian StyleYogesh, Ahana, Michael Taylor, and Mary P. Chang. 2020. "Characterization of Pediatric Seizures in the Commonwealth of the Northern Mariana Islands" Children 7, no. 4: 26. https://doi.org/10.3390/children7040026
APA StyleYogesh, A., Taylor, M., & Chang, M. P. (2020). Characterization of Pediatric Seizures in the Commonwealth of the Northern Mariana Islands. Children, 7(4), 26. https://doi.org/10.3390/children7040026