Pediatric Mortality in a Rural Tertiary Care Center in Liberia

Abstract
:1. Introduction
2. Results
2.1. Overview
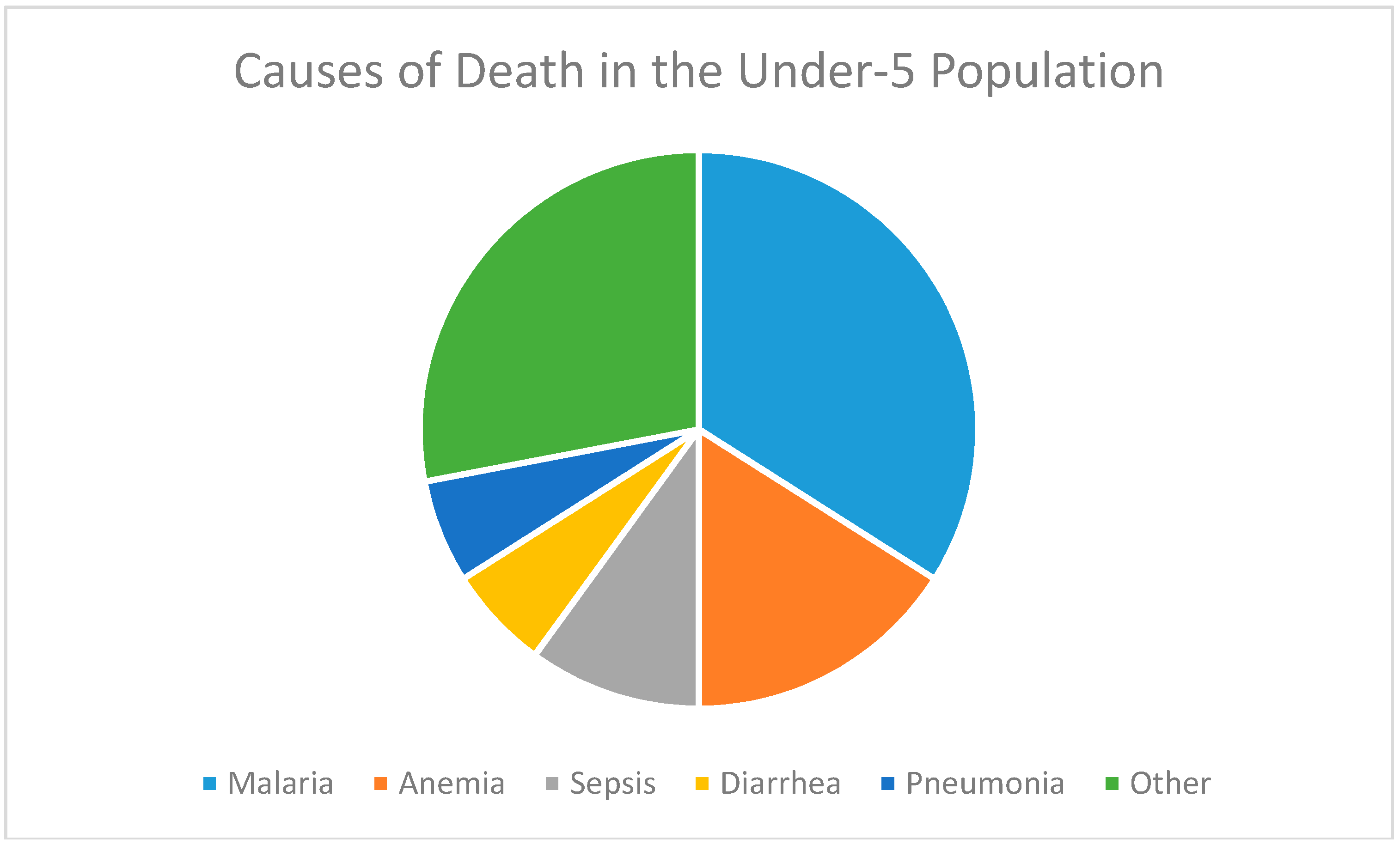
2.2. Causes of Mortality
3. Discussion
4. Materials and Methods
4.1. Study Setting
4.2. Study Design
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United Nations Economic Commission for Africa, African Union, African Development Bank and United Nations Development Programme. MDG Report 2015: Assessing Progress in Africa toward the Millennium Development Goals; ECA Documents Publishing Unit: Addis Ababa, Ethiopia, 2015. [Google Scholar]
- The World Bank. Mortality Rate, Under-5 (per 100). Available online: http://data.worldbank.org/indicator/SH.DYN.MORT (accessed on 25 February 2016).
- The World Bank. Immunization, Measles (% of Children Ages 12–23 Months). Available online: http://data.worldbank.org/indicator/SH.IMM.MEAS (accessed on 25 February 2016).
- Couto, T.B.; Farhat, S.C.; Reid, T.; Schvartasman, C. Mortality in a pediatric secondary-care hospital in post-conflict Liberia in 2009. Einstein (Sao Paulo) 2013, 11, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Huerga, H.; Vasset, B.; Prados, E. Adult and paediatric mortality patterns in a referral hospital in Liberia 1 year after the end of the war. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Embu, H.Y.; Yiltok, S.J.; Isamade, E.S.; Nuhu, S.I.; Oyeniran, O.O.; Uba, F.A. Paediatric admissions and outcome in a general intensive care unit. Afr. J. Pediatr. Surg. 2011, 8, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.D.; Sow, S.O.; Levine, M.M.; Kotloff, K.L. The causes of hospital admission and death among children in Bamako, Mali. J. Trop. Pediatr. 2004, 50, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Veirum, J.E.; Biai, S.; Jakobsen, M.; Sandstrom, A.; Hedegaard, K.; Kofoed, P.E.; Aaby, P.; Sodemann, M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Pediatr. 2007, 96, 1526–1530. [Google Scholar] [CrossRef] [PubMed]
- Sodemann, M.; Veirum, J.; Biai, S.; Nielsen, J.; Bale, C.; Skytte Jakobsen, M.; Gustafson, P.; Aaby, P. Reduced case fatality among hospitalized children during a war in Guinea-Bissau: A lesson in equity. Acta Paediatr. 2004, 93, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Kentoffio, K.; Kraemer, J.D.; Griffiths, T.; Kenny, A.; Panjabi, R.; Sechler, G.A.; Selinsky, S.; Siedner, M.J. Charting health system reconstruction in post-war Liberia: A comparison of rural vs. remote healthcare utilization. BMC Health Serv. Res. 2016, 16, 478. [Google Scholar] [CrossRef] [PubMed]
- Charles, N.C.; Chuku, A.; Anazodo, N.M. Childhood mortality in federal medical centre umuahia, South eastern Nigeria. Oman Med. J. 2014, 29, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Requejo, J.; Victora, C.; Bryce, J. Scientific Review Group of Countdown to 2015. Data Resource Profile: Countdown to 2015: Maternal, Newborn and Child Survival. Int. J. Epidemiol. 2014, 43, 586–596. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Liberia: Country Cooperation Strategy at a Glance. Available online: http://www.who.int/countryfocus/cooperation_strategy/ccsbrief_lbr_09_en.pdf?ua=1 (accessed on 25 February 2016).
- Centers for Disease Control and Prevention. Malaria: Insecticide-Treated Bed Nets. Available online: http://www.cdc.gov/malaria/malaria_worldwide/reduction/itn.html (accessed on 3 April 2016).
- World Bank Data. Use of Insecticide-Treated Bed Nets (% of Under-5 Population). Available online: http://data.worldbank.org/indicator/SH.MLR.NETS.ZS (accessed on 2 April 2016).
- UNICEF. At a Glance: Liberia, Statistics. 2016. Available online: http://www.unicef.org/infobycountry/liberia_statistics.html (accessed on 3 April 2016).
- Bawo, L.L.; Harries, A.D.; Reid, T.; Massaquoi, M.; Jallah-Macauley, R.; Jones, J.J.; Wesseh, C.S.; Enders, J.; Hinneh, L. Coverage and use of insecticide-treated bed nets in households with children aged under five years in Liberia. Public Health Action 2012, 2, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Roper, M.H.; Vandelaer, J.H.; Gasse, F.L. Maternal and neonatal tetanus. Lancet 2007, 370, 1947–1959. [Google Scholar] [CrossRef]
- UNICEF. State of the World’s Children 2015 Country Statistical Information. Available online: http://www.data.unicef.org/corecode/uploads/document6/uploaded_pdfs/corecode/SOWC_2015_all-countries-update_214.xlsx (accessed on 3 April 2016).
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000–13 with projections to inform post-2015 priorities: An updated systemic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- Biai, S.; Rodrigues, A.; Gomes, M.; Ribeiro, I.; Sodemann, M.; Alves, F.; Aaby, P. Reduced in-hospital mortality after improved management of children under 5 years admitted to hospital with malaria: Randomized trial. BMJ 2007, 335, 862. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.R.; Thornton, J.N.; Holder, W. Infant and child mortality estimates in two counties of Liberia: 1984. Int. J. Epidemiol. 1993, 22, S42–S49. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Number of Deaths (% of Total Deaths in Age Group) | |||||
|---|---|---|---|---|---|
| Cause of Death | Neonates (<1 Month) N = 9 | 1 Month to <1 Year, N = 9 | 1 Year to <5 Year, N = 23 | ≥5 Years, N = 9 | Total |
| Sepsis | 4 | 1 | 0 | 0 | 5 |
| Tetanus | 2 * | 1 | 0 | 1 | 4 |
| Meningitis | 2 | 0 | 0 | 0 | 2 |
| Pneumothorax | 1 | 0 | 0 | 0 | 1 |
| Malaria | 1 * | 4 | 16 | 2 | 23 |
| Pneumonia | 0 | 2 | 1 | 1 | 4 |
| Diarrhea | 0 | 1 | 2 | 1 | 4 |
| Caustic ingestion | 0 | 0 | 1 | 0 | 1 |
| Malnutrition | 0 | 0 | 1 | 0 | 1 |
| Perioperative complications | 0 | 0 | 1 | 0 | 1 |
| Anemia | 0 | 0 | 1 | 1 | 2 |
| Acute abdomen | 0 | 0 | 0 | 1 | 1 |
| Congestive heart failure | 0 | 0 | 0 | 1 | 1 |
| Abdominal mass | 0 | 0 | 0 | 1 | 1 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.; Walters, C.B.; Sampson, J.; Kateh, F.; Chang, M.P. Pediatric Mortality in a Rural Tertiary Care Center in Liberia. Children 2017, 4, 8. https://doi.org/10.3390/children4020008
Tsai C, Walters CB, Sampson J, Kateh F, Chang MP. Pediatric Mortality in a Rural Tertiary Care Center in Liberia. Children. 2017; 4(2):8. https://doi.org/10.3390/children4020008
Chicago/Turabian StyleTsai, Carmelle, Camila B. Walters, John Sampson, Francis Kateh, and Mary P. Chang. 2017. "Pediatric Mortality in a Rural Tertiary Care Center in Liberia" Children 4, no. 2: 8. https://doi.org/10.3390/children4020008
APA StyleTsai, C., Walters, C. B., Sampson, J., Kateh, F., & Chang, M. P. (2017). Pediatric Mortality in a Rural Tertiary Care Center in Liberia. Children, 4(2), 8. https://doi.org/10.3390/children4020008