
Readhesion of Tongue-Tie Following Neonatal Frenotomy: Incidence and Impact of Postoperative Exercises in a Prospective Observational Study
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
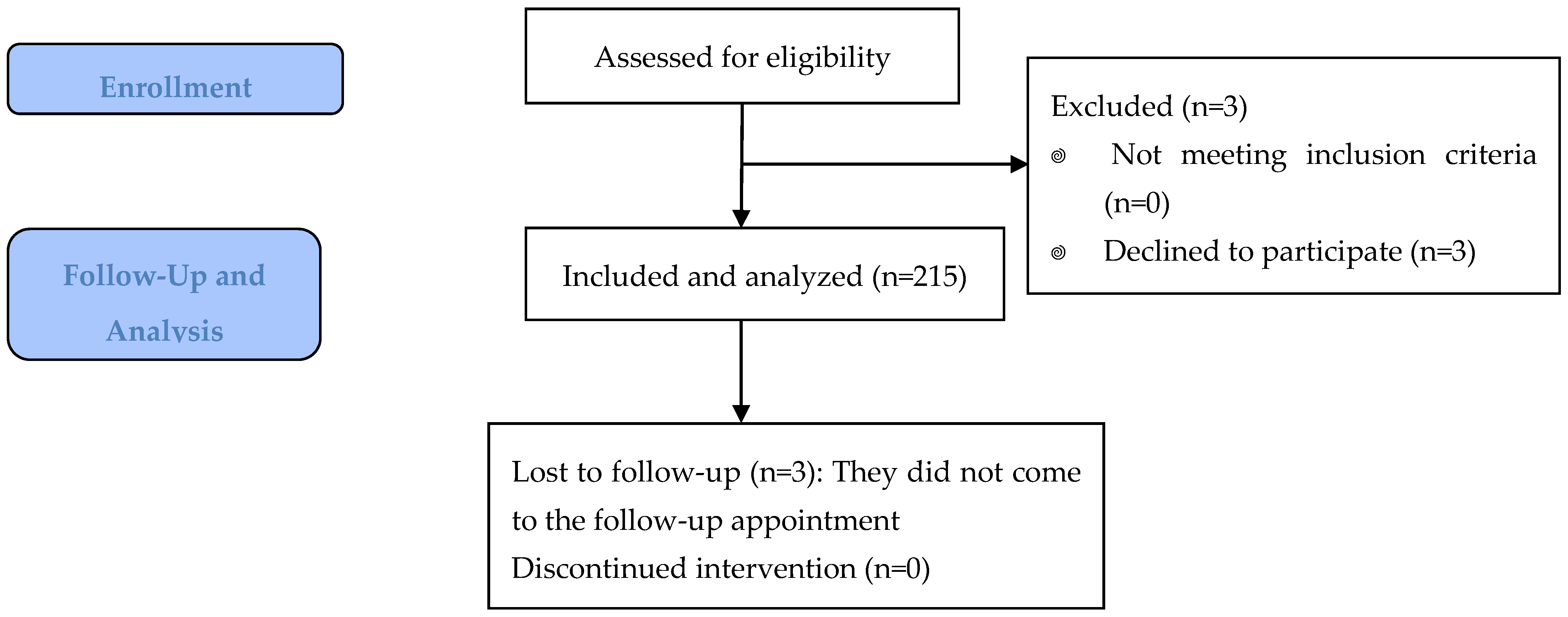
3.1. Description of Our Population
3.2. Feeding
3.3. Hazelbaker Scores
3.4. Readhesion
- -
- Female patients: global readhesion risk = 0.236 (95%CI 0.155–0.344); symptomatic readhesion risk = 0.105 (95%CI 0.543–0.194)
- -
- Male patients: global readhesion risk = 0.390 (95%CI 0.312–0.474); symptomatic readhesion risk = 0.183 (95%CI 0.128–0.257)
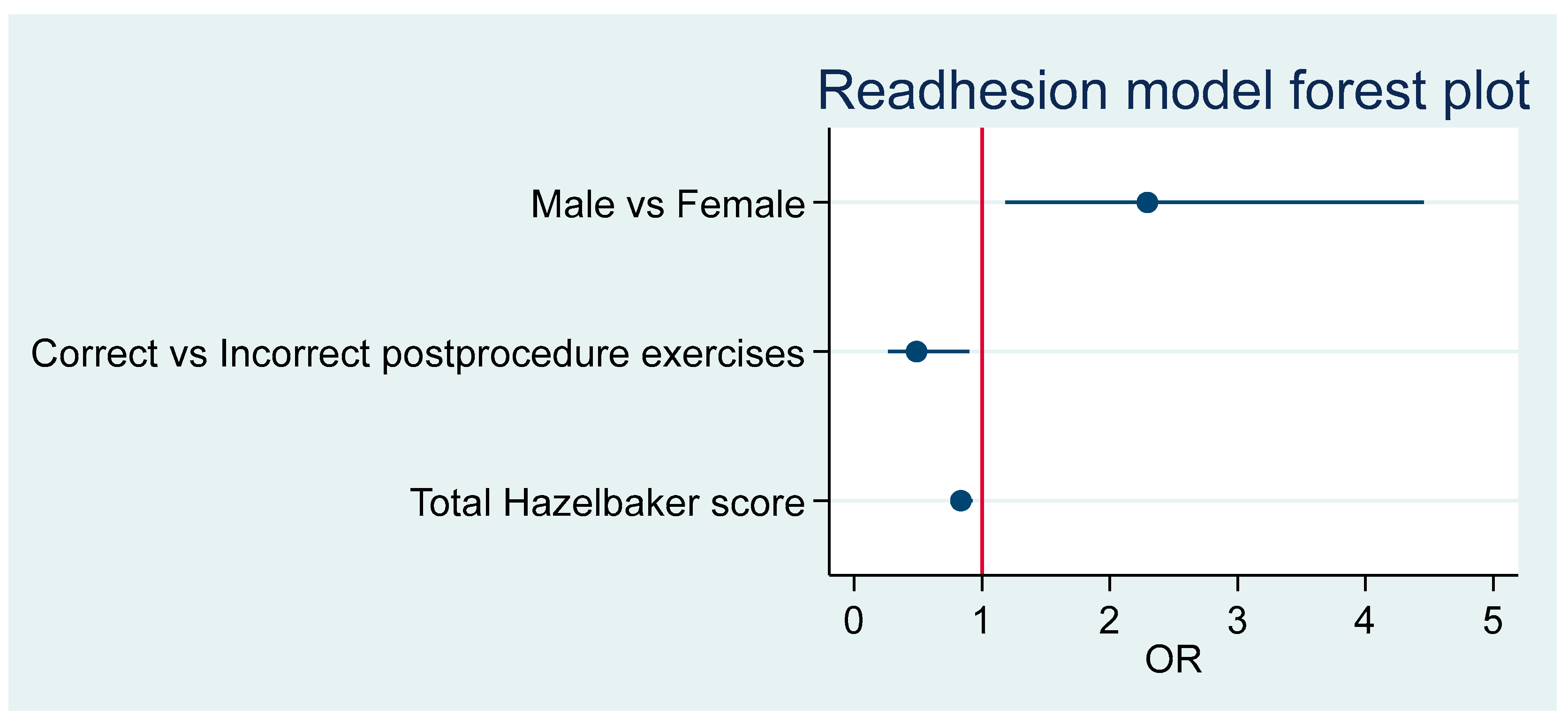
3.5. Patients at Risk for Readhesion
3.6. Symptomatic Readhesion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIC | Akaike information criterion |
| AUC | Area under the curve |
| CI | Confidence interval |
| IQR | Interquartile range |
| OR | Odds ratio |
| ROC | Receiver Operating Characteristic |
| RR | Relative risk |
| SD | Standard deviation |
| TT | Tongue-tie |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLLF) | |||
|---|---|---|---|
| Appearance items | Score | Function items | Score |
| Appearance of tongue when lifted | Lateralization | ||
| Round or square | 2 | Complete | 2 |
| Slight cleft in tip apparent | 1 | Body of tongue but not tongue tip | 1 |
| Heart-shaped | 0 | None | 0 |
| Elasticity of frenulum | Lift of tongue | ||
| Very elastic (excellent) | 2 | Tip to mid-mouth | 2 |
| Moderately elastic | 1 | Only edges to mid-mouth | 1 |
| Little or no elasticity | 0 | Tip stays at alveolar ridge or rises to mid-mouth only with jaw closure | 0 |
| Length of lingual frenulum when tongue lifted | Extension of tongue | ||
| More than 1 cm or embedded in tongue | 2 | Tip over lower lip | 2 |
| 1 cm | 1 | Tip over lower gum only | 1 |
| Less than 1 cm | 0 | Neither of above, or anterior or midtongue humps | 0 |
| Attachment of lingual frenulum to tongue | Spread of anterior tongue | ||
| Posterior to tip | 2 | Complete | 2 |
| At tip | 1 | Moderate or partial | 1 |
| Notched tip | 0 | Little or none | 0 |
| Attachment of lingual frenulum to inferior alveolar ridge | Cupping | ||
| Attached to floor of mouth or well below ridge | 2 | Entire edge, firm cup | 2 |
| Attached just below ridge | 1 | Side edges only, moderate cup | 1 |
| Attached at ridge | 0 | Poor or no cup | 0 |
| Total appearance score | Peristalsis | ||
Function items score
Frenotomy necessary if Appearance item score is <8. | Complete, anterior to posterior (originates at the tip) | 2 | |
| Partial: originating posterior to tip | 1 | ||
| None or reverse | 0 | ||
| Snapback | |||
| None | 2 | ||
| Periodic | 1 | ||
| Frequent or with each suck | 0 | ||
| Total function score | |||
References
- Berry, J.; Griffiths, M.; Westcott, C. A double-blind, randomized, controlled trial of tongue-tie division and its immediate effect on breastfeeding. Breastfeed Med. 2012, 7, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.; Johnson, D.; Copeland, M.; Churchill, C.; Taylor, H.; Emond, A. The development of a tongue assessment tool to assist with tongue-tie identification. ADC Fetal Neonatal Ed. 2015, 100, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Ricke, L.A.; Baker, N.J.; Madlon-Kay, D.J.; DeFor, T.A. Newborn tongue-tie: Prevalence and effect on breast-feeding. J. Am. Board Fam. Pract. 2005, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bhandarkar, K.P.; Dar, T.; Karia, L.; Upadhyaya, M. Post Frenotomy Massage for Ankyloglossia in Infants-Does It Improve Breastfeeding and Reduce Recurrence? Matern. Child Health J. 2022, 26, 1727–1731. [Google Scholar] [CrossRef] [PubMed]
- Narsat, M.A.; Beygirci, A.; Özdönmez, G.T.; Yıldız, E. Grouping of Ankyloglossia According to Coryllos Anatomical Classification and Follow-Up Results for Breastfeeding: Single-Center, Cross-Sectional Study. Children 2022, 9, 1860. [Google Scholar] [CrossRef] [PubMed]
- Maya-Enero, S.; Pérez-Pérez, M.; Ruiz-Guzmán, L.; Duran-Jordà, X.; López-Vílchez, M.Á. Prevalence of neonatal ankyloglossia in a tertiary care hospital in Spain: Atransversal cross-sectional study. Eur. J. Pediatr. 2021, 180, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Ferrés-Amat, E.; Pastor-Vera, T.; Ferrés-Amat, E.; Mareque-Bueno, J.; Prats-Armengol, J.; Ferrés-Padró, E. Multidisciplinary management of ankyloglossia in childhood. Treatment of 101 cases. A protocol. Med. Oral. Patol. Oral. Cir. Bucal. 2016, 21, e39–e47. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.E.; Gilliland, A.M.; LeFort, Y. Complications and misdiagnoses associated with infant frenotomy: Results of a healthcare professional survey. Int. Breastfeed J. 2022, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Hale, M.; Mills, N.; Edmonds, L.; Dawes, P.; Dickson, N.; Barker, D.; Wheeler, B.J. Complications following frenotomy for ankyloglossia: A 24-month prospective New Zealand Paediatric Surveillance Unit study. J. Paediatr. Child Health 2020, 56, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Francis, D.O.; Chinnadurai, S.; Morad, A.; A Epstein, R.; Kohanim, S.; Krishnaswami, S.; A Sathe, N.; McPheeters, M.L. Treatments for Ankyloglossia and Ankyloglossia with Concomitant Lip-Tie; Report No.: 15-EHC011-EF; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. [Google Scholar]
- O’Shea, J.E.; Foster, J.P.; O’Donnell, C.P.; Breathnach, D.; E Jacobs, S.; A Todd, D.; Davis, P.G. Frenotomy for tongue-tie in newborn infants. Cochrane Database Syst. Rev. 2017, 3, CD011065. [Google Scholar] [CrossRef] [PubMed]
- Brookes, A.; Bowley, D.M. Tongue tie: The evidence for frenotomy. Early Hum. Dev. 2014, 90, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Hong, P.; Lago, D.; Seargeant, J.; Pellman, L.; Magit, A.E.; Pransky, S.M. Defining ankyloglossia: A case series of anterior and posterior tongue ties. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 1003–1006. [Google Scholar] [CrossRef] [PubMed]
- Argiris, K.; Vasani, S.; Wong, G.; Stimpson, P.; Gunning, E.; Caulfield, H. Audit of tongue-tie division in neonates with breastfeeding difficulties: How we do it. Clin. Otolaryngol. 2011, 36, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Klockars, T.; Pitkäranta, A. Pediatric tongue-tie division: Indications, techniques and patient satisfaction. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1399–1401. [Google Scholar] [CrossRef] [PubMed]
- Steehler, M.W.; Steehler, M.K.; Harley, E.H. A retrospective review of frenotomy in neonates and infants with feeding difficulties. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1236–1240. [Google Scholar] [CrossRef] [PubMed]
- Messner, A.H.; Walsh, J.; Rosenfeld, R.M.; Schwartz, S.R.; Ishman, S.L.; Baldassari, C.; Brietzke, S.E.; Darrow, D.H.; Goldstein, N.; Levi, J.; et al. Clinical Consensus Statement: Ankyloglossia in Children. Otolaryngol. Head Neck Surg. 2020, 162, 597–611. [Google Scholar] [CrossRef] [PubMed]
- Dhir, S.; Landau, B.P.; Edemobi, S.; Meyer, A.K.; Durr, M.L. Survey of Pediatric Otolaryngology Frenotomy Practice Patterns. Laryngoscope 2022, 132, 2505–2512. [Google Scholar] [CrossRef] [PubMed]
- Ghaheri, B.A.; Cole, M.; Fausel, S.C.; Chuop, M.; Mace, J.C. Breastfeeding improvement following tongue-tie and lip-tie release: A prospective cohort study. Laryngoscope 2017, 127, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.; Al Khoury, A.; Puzhko, S.; Dobrich, C.; Stern, M.; Mitnick, H.; Goldfarb, L. Frenotomy in Infants with Tongue-Tie and Breastfeeding Problems. J. Hum. Lact. 2019, 35, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Tomara, E.; Dagla, M.; Antoniou, E.; Iatrakis, G. Ankyloglossia as a Barrier to Breastfeeding: A Literature Review. Children 2023, 10, 1902. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.E.; Chung, H.R.; Marshall, C.R.; Wilhalme, H.M.; West, A.N. Outcomes of stretching exercises after lingual frenotomy in infants: A prospective, interventional study. Int. J. Pediatr. Otorhinolaryngol. 2025, 191, 112280. [Google Scholar] [CrossRef] [PubMed]
- Murias, I.; Grzech-Leśniak, K.; Murias, A.; Walicka-Cupryś, K.; Dominiak, M.; Deeb, J.G.; Matys, J. Efficacy of various laser wavelengths in the surgical treatment of Ankyloglossia: A systematic review. Life 2022, 12, 558. [Google Scholar] [CrossRef] [PubMed]
- Amir, L.H.; James, J.P.; Donath, S.M. Reliability of the hazelbaker assessment tool for lingual frenulum function. Int. Breastfeed J. 2006, 1, 3. [Google Scholar] [CrossRef] [PubMed]
- Drazin, P. The Assessment Tool for Lingual Frenulum Function (ATLFF): Use in a Lactation Consultant Private Practice. J. Hum. Lact. 1994, 10, 54. [Google Scholar] [CrossRef]
- Billington, J.; Yardley, I.; Upadhyaya, M. Long-term efficacy of a tongue tie service in improving breast feeding rates: A prospective study. J. Pediatr. Surg. 2018, 53, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Braccio, S.; Chadderton, U.M. Tongue-tie division: Is it worth it? Br. J. Midwifery 2016, 24, 317–321. [Google Scholar] [CrossRef]
- Callen, J.; Pinelli, J. Incidence and duration of breastfeeding for term infants in Canada, United States, Europe, and Australia: A literature review. Birth 2004, 31, 285–292. [Google Scholar] [CrossRef]
- Smart, S.; Grant, H.; Tseng, R.J. Beyond surgery: Pre- and post-operative care in children with ankyloglossia. Int. J. Paediatr. Dent. 2025, 35, 318–338. [Google Scholar] [CrossRef] [PubMed]
- Frezza, A.; Ezeddine, F.; Zuccon, A.; Gracco, A.; Bruno, G.; De Stefani, A. Treatment of Ankyloglossia: A Review. Children 2023, 10, 1808. [Google Scholar] [CrossRef] [PubMed]
- Alabama Tongue-Tie Center Website. Infant Aftercare Stretching Video. Available online: https://tonguetie.com/videos/ (accessed on 27 May 2025).
- Baxter, R.; Merkel-Walsh, R.; Baxter, B.S.; Lashley, A.; Rendell, N.R. Functional improvements of speech, feeding, and sleep after lingual frenectomy tongue-tie release: A prospective cohort study. Clin. Pediatr. 2020, 9, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Hand, P.; Olivi, G.; Lajolo, C.; Gioco, G.; Marigo, L.; Castagnola, R.; Cordaro, M. Short lingual frenum in infants, children and adolescents. Part 1: Breastfeeding and gastroesophageal reflux disease improvement after tethered oral tissues release. Eur. J. Paediatr. Dent. 2020, 21, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Jaikaria, A.; Pahuja, S.K.; Thakur, S.; Negi, P. Treatment of partial ankyloglossia using Hazelbaker assessment tool for lingual frenulum function (HATLFF): A case report with 6-month follow-up. Natl. J. Maxillofac. Surg. 2021, 12, 280–283. [Google Scholar] [CrossRef] [PubMed]



| Readhesion n = 71 (33.5%) | No Readhesion n = 141 (66.5%) | p-Value | |
|---|---|---|---|
| Male newborn (n, %) | 53 (39.0) | 83 (61.0) | 0.033 a |
| Birth weight (grams), mean (SD) (range) | 3252.6 (482.2) (1284–4175) | 3221.1 (560.8) (1640–4650) | 0.70 b |
| Gestational age (weeks), mean (SD) (range) | 391/7 (16/7) 300/7–420/7 | 392/7 (16/7) 305/7–422/7 | 0.92 b |
| Age at frenotomy (hours) median (IQR) (range) | 50 (308) (5–1440) | 61 (176) (15–1152) | 0.40 b |
| Exclusive Breastfeeding | Partial Breastfeeding | p-Value a | |
|---|---|---|---|
| No readhesion (n, %) | 92 (64.79) | 43 (30.28) | 0.07 |
| Asymptomatic readhesion (n, %) | 31 (83.78) | 4 (10.81) | |
| Symptomatic readhesion (n, %) | 19 (55.88) | 14 (41.18) | |
| Total | 142 (66.67) | 61 (28.64) |
| Readhesion n = 71 (33.5%) | No Readhesion n = 141 (66.5%) | p-Value | |
|---|---|---|---|
| Symptoms | |||
| Yes (n, %) | 33 (46.5) | 0 (0) | - |
| No (n, %) | 38 (53.5) | 0 (0) | |
| Hazelbaker score for appearance pre-frenotomy | |||
| median (IQR) | 6 (3) | 7 (2) | <0.001 a |
| (range) | (1–10) | (0–10) | |
| Hazelbaker score for appearance post-frenotomy | |||
| median (IQR) | 8 (2) | 10 (1) | <0.001 a |
| (range) | (4–10) | (8–10) | |
| Increase in Hazelbaker score for appearance pre- vs. post-frenotomy, mean (SD) | 2.3 (2.0) | 2.7 (1.6) | 0.106 b |
| Hazelbaker score for function pre-frenotomy | |||
| median (IQR) | 9 (28) | 10 (3) | 0.005 a |
| (range) | (4–12) | (5–14) | |
| Hazelbaker score for function post-frenotomy | |||
| median (IQR) | 11 (3) | 13 (2) | <0.001 a |
| (range) | (7–14) | (10–14) | |
| Increase in Hazelbaker score for function pre- vs. post-frenotomy, mean (SD) | 2.3 (2.4) | 3.7 (1.9) | <0.001 b |
| Readhesion n = 71 (33.5%) | No Readhesion n = 141 (66.5%) | p-Value a | |
|---|---|---|---|
| No exercises (n, %) | 8 (72.7) | 3 (27.3) | 0.017 |
| Exercises incorrectly done (n, %) | 28 (36.8) | 48 (63.2) | |
| Exercises correctly done (n, %) | 35 (28.0) | 90 (72.0) |
| OR | 95%CI | p-Value | |
|---|---|---|---|
| Sex a | 2.207 | 0.869–5.606 | 0.096 |
| Age at frenotomy (hours) | 1.002 | 1.001–1.004 | 0.000 |
| Total Hazelbaker score | 0.807 | 0.706–0.923 | 0.002 |
| Exercices b | 0.443 | 0.190–1.030 | 0.059 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valle-Del Barrio, B.; Maya-Enero, S.; Prat-Ortells, J.; López-Vílchez, M.Á.; Candel-Pau, J. Readhesion of Tongue-Tie Following Neonatal Frenotomy: Incidence and Impact of Postoperative Exercises in a Prospective Observational Study. Children 2025, 12, 971. https://doi.org/10.3390/children12080971
Valle-Del Barrio B, Maya-Enero S, Prat-Ortells J, López-Vílchez MÁ, Candel-Pau J. Readhesion of Tongue-Tie Following Neonatal Frenotomy: Incidence and Impact of Postoperative Exercises in a Prospective Observational Study. Children. 2025; 12(8):971. https://doi.org/10.3390/children12080971
Chicago/Turabian StyleValle-Del Barrio, Beatriz, Silvia Maya-Enero, Jordi Prat-Ortells, María Ángeles López-Vílchez, and Júlia Candel-Pau. 2025. "Readhesion of Tongue-Tie Following Neonatal Frenotomy: Incidence and Impact of Postoperative Exercises in a Prospective Observational Study" Children 12, no. 8: 971. https://doi.org/10.3390/children12080971
APA StyleValle-Del Barrio, B., Maya-Enero, S., Prat-Ortells, J., López-Vílchez, M. Á., & Candel-Pau, J. (2025). Readhesion of Tongue-Tie Following Neonatal Frenotomy: Incidence and Impact of Postoperative Exercises in a Prospective Observational Study. Children, 12(8), 971. https://doi.org/10.3390/children12080971