
At-School Telerehabilitation for Rett Syndrome: Support Teachers Driving Cognitive and Communication Progress in a Randomized Trial



Abstract
1. Introduction
1.1. Rett Syndrome
1.2. Inclusive Education in Italy
1.3. Telerehabilitation as a Tool for Cognitive Rehabilitation
1.4. Study Hypotheses
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Assessment and Measures
2.4. Procedure
- T0 (Baseline): Prior to intervention.
- T1 (Midpoint): After three months of training.
- T2 (Post-intervention): After six months of training.
- T3 (Follow-up): Three months after the end of the intervention, during a period with no rehabilitation activity (i.e., the summer school break).
2.5. Statistical Analysis
3. Results
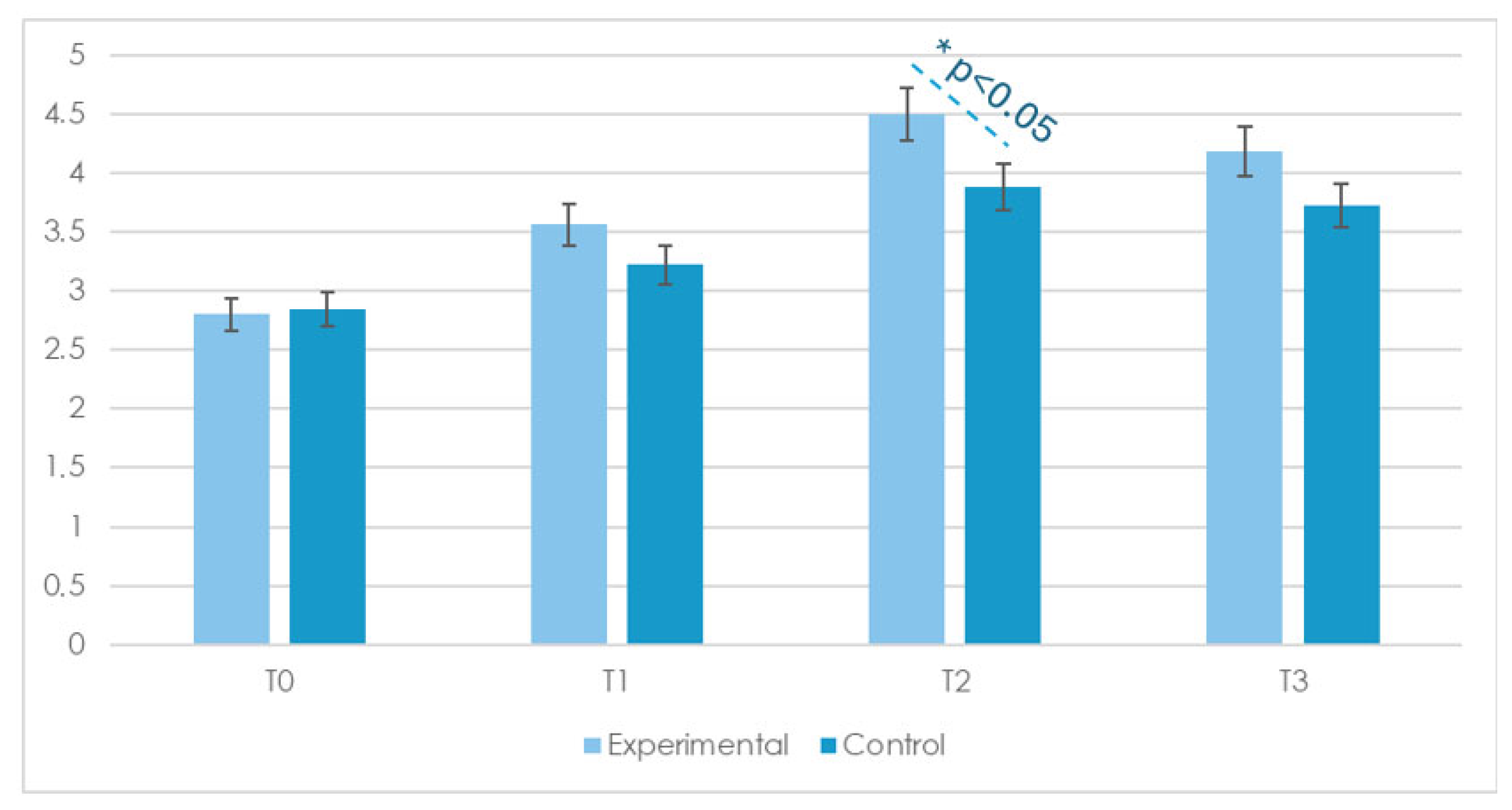
3.1. Basic Cognitive Abilities
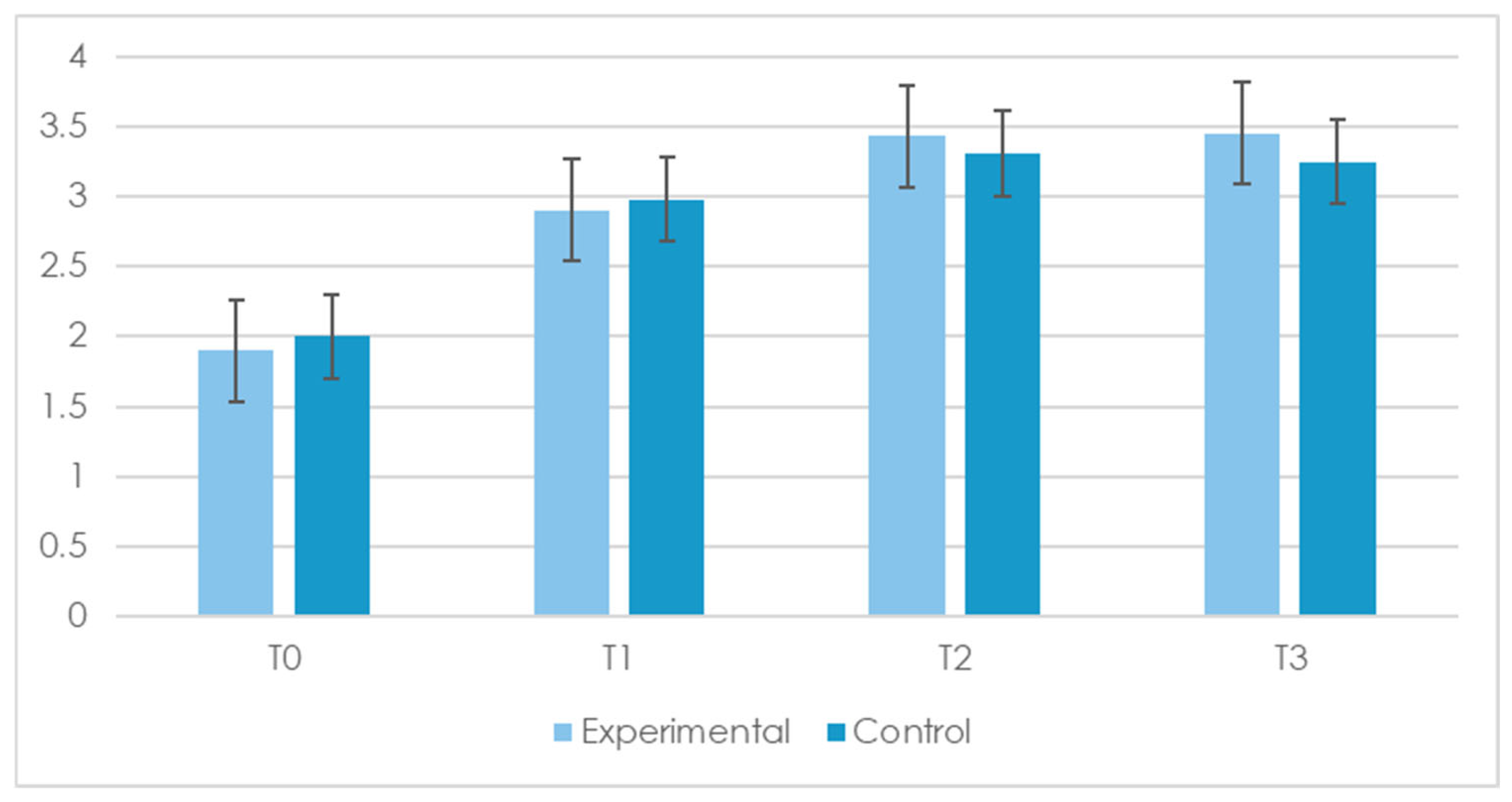
3.2. Communication Abilities
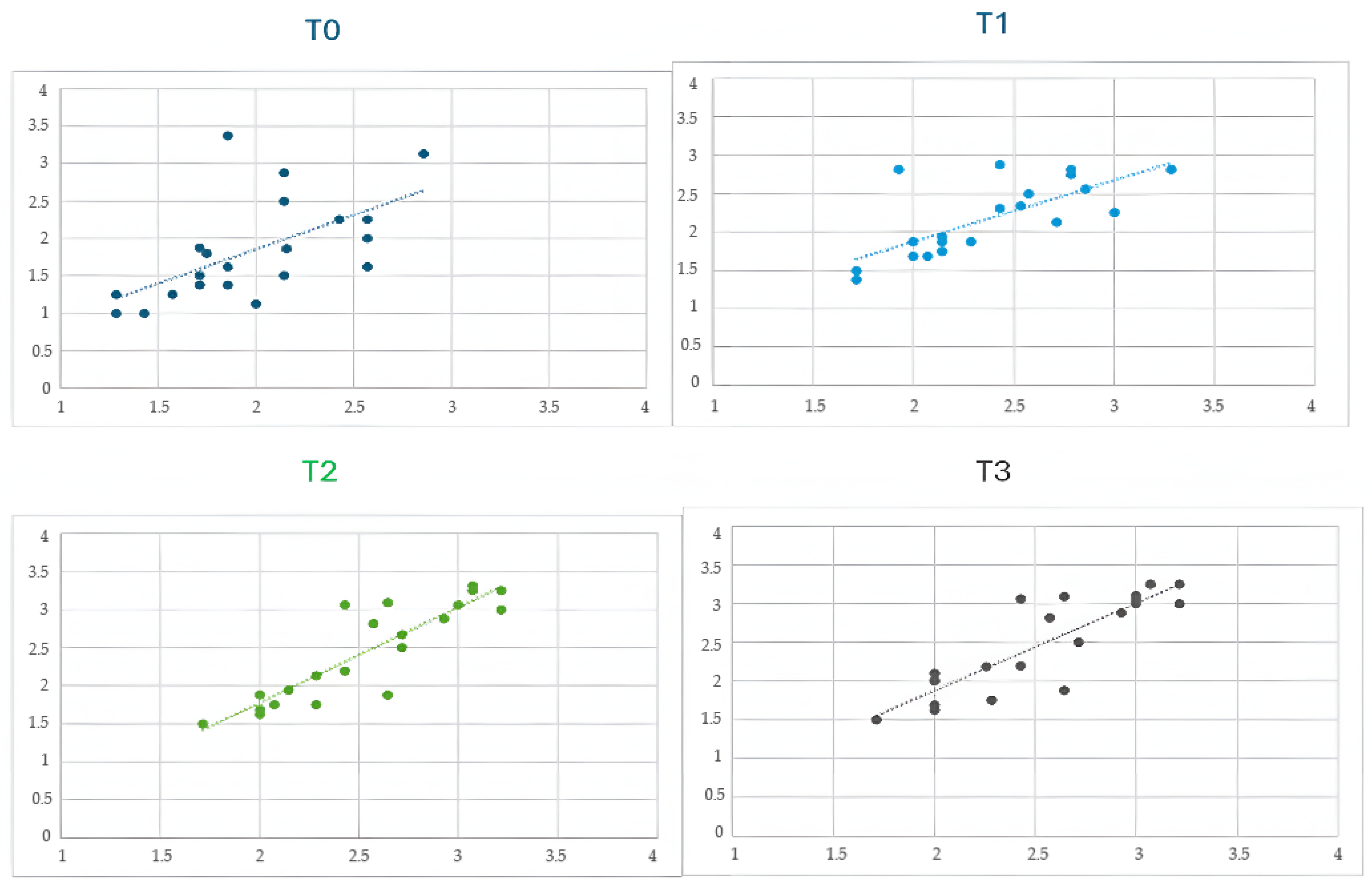
3.3. Correlation Between Cognitive and Communication Skills
4. Discussion
4.1. Cognitive and Communicative Improvements
4.2. The Interdependence of Cognitive and Communication Skills
4.3. Telerehabilitation as a Tool for Inclusive Education
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RTT | Rett Syndrome |
| TR | Telerehabilitation |
| VR | Virtual Reality |
| GAIRS | Global Assessment and Intervention Rating Scale |
| VABSs | Vineland Adaptive Behavior Scales |
| RARS | Rett Assessment Rating Scale |
Appendix A
| Ability | Assessment Procedure |
| Basic Cognitive Abilities | |
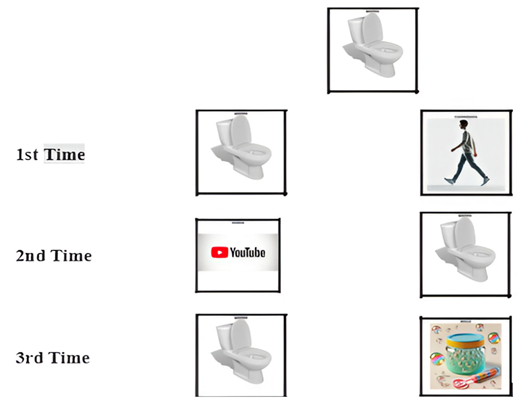
| Object recognition | The therapist prepares target stimuli with objects of daily use (e.g., a plate, a glass, a phone, or a bottle). The participant sits at a table and has the target on her right along with a distractor on her left. The participant is asked to look at them and to choose the target by looking at it and/or touching it. Then, the position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Object permanence recognition | The participant is seated at a table facing the therapist. A preferred object or food item is shown, then visibly hidden under a cup or tissue. The participant is encouraged to locate the hidden item by visually tracking it and, if motor abilities permit, by reaching for and retrieving it. The procedure is repeated three times, with the hiding location varied. |
| Color discrimination | The therapist prepares target stimuli with identical objects of different colors. The participant sits at a table and has the target (e.g., a red cube) on her right and a distractor (e.g., a cube of another color) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Geometric form discrimination | The therapist prepares target stimuli with geometric forms such as a circle, a square, a triangle, a rectangle, or a rhombus. The participant sits at a table and has the target (e.g., a circle) on her right and a distractor (e.g., a triangle) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Cause–effect relationship | The therapist prepares target stimuli with figures depicting a sequence of events: a cause and effect scene. The participant sits at a table and has the target (e.g., a girl falls off the bike) on her right and a distractor (e.g., the girl cries) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Anticipation of familiar events | The therapist selects a familiar and highly routinized activity for the participant (e.g., snack time or going to bed). The activity is always preceded by the same verbal or visual cue (e.g., showing a spoon before snack time). After several repetitions, the therapist presents only the anticipatory cue and asks the participant to select the activity related to it. The trial is repeated three times with different cues associated with distinct events. |
| Object-function matching | The therapist presents two or more everyday objects (e.g., a toothbrush, a spoon, or a hairbrush) and a corresponding picture or symbolic cue (e.g., an image of teeth, food, or hair). The participant is asked to match the object to its function by selecting or touching the correct object that corresponds to the presented cue. The trial is repeated with at least three different sets of objects and functions, with the position of the items randomized each time. |
| Quantity discrimination | The therapist prepares visual stimuli showing sets of objects in different quantities (e.g., two apples vs. five apples). The participant is asked to choose the larger or smaller quantity, either verbally or by pointing, touching, or looking at the correct image. The stimuli are presented in pairs, and the position of the larger/smaller group is alternated randomly. |
| Object categorization by function | The therapist presents an image of a familiar object along with two additional images: one representing the correct function of the object (e.g., eating for a spoon or personal care for a comb) and one unrelated distractor. The participant is asked to identify the correct function of the object by selecting the appropriate image, either through pointing or gaze fixation. |
| Understanding simple sequences | The therapist uses picture cards or object-based steps of a familiar routine (e.g., putting on socks or brushing teeth). The cards are initially presented in the correct order, and the participant is asked to observe the sequence. Then, the cards are presented in a scrambled order, and the participant is asked to rearrange or indicate the correct order (via gaze, pointing, or verbal cue). The task is repeated with at least two different routines. |
| Human body discrimination | The therapist prepares target stimuli with body parts. The participant sits at a table and has the target (e.g., belly) on her right and a distractor (e.g., foot) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Spatial concepts | The therapist prepares target stimuli with an object placed in 10 different ways: inside/out, above/below, front/behind, ear/far, and right/left. The participant sits at a table and has the target (e.g., inside) on her right and a distractor (e.g., out) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Measure concepts | The therapist prepares target stimuli with six objects, which are large and tight, high and low, and long and short. The participant sits at a table and has the target (e.g., large) on her right and a distractor (e.g., tight) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Time concepts | The therapist prepares target stimuli with images representing a sequence: before, after, and finally. The participant sits at a table and has the target (e.g., before) on her right and a distractor (e.g., after) on her left. She is asked to look at them and to choose the target by looking at it and/or touching it. The position of the stimuli is changed, and the whole procedure is repeated three times with the stimuli in a random order. |
| Communication Abilities | |
| Respond to name/verbal prompt | The therapist calls the participant’s name or gives a simple verbal cue (e.g., “Look here”). The participant is expected to respond by orienting her gaze, turning her head, or making another observable acknowledgment. The prompt is repeated several times with variations in intonation and distance to assess consistency. |
| Express need—non-verbal | In the assessment of this ability, the therapist observes the participant in different daily situations with the collaboration of caregivers and verifies if the participant communicates some basic needs, such as drink, eat, and go to the bathroom, with vocalization or facial expressions. |
| Express refusal—non-verbal | An undesired or non-preferred item or activity is presented (e.g., an object the participant usually refuses). The participant is encouraged to indicate refusal through non-verbal means such as turning away, pushing the object, shaking the head, or other body language indicating rejection. |
| Shared attention (gaze alternation) | The therapist presents an interesting object or event and then shifts their gaze between the object and the participant, encouraging the participant to do the same. Alternating their gaze between the object and the therapist is considered an indicator of shared attention. This is repeated across different contexts to assess intentionality. |
| Understanding gestures from others | The therapist uses simple, commonly understood gestures (e.g., waving goodbye, pointing to an object, or nodding for “yes”). The participant is expected to demonstrate understanding by responding appropriately—e.g., looking toward the pointed object, waving back, or acting accordingly. |
| Use context-based vocalizations | The participant is observed during structured interactions (e.g., snack time or play) for the use of intentional vocalizations that appear to be linked to the context (e.g., sounds indicating satisfaction, requests, or attention seeking). The therapist notes whether vocalizations are spontaneous and appropriately timed. |
| Participate in routine exchanges | The therapist engages the participant in familiar social routines (e.g., “peek-a-boo,” “give and take,” or turn-taking games). Participation may include gestures, vocalizations, gaze, or movement that aligns with the expected turn in the routine. Multiple routines are used to assess generalization. |
| Express need—picture | The participant is presented with pictures of preferred items. When motivated, she is encouraged to select the image corresponding to her need (e.g., water or toy) by pointing, touching, or looking at the picture. |
| Match need to picture | The therapist presents a real object or situation (e.g., a drink or the start of an activity) and asks the participant to select the corresponding picture among distractors. Correct matching demonstrates an understanding of symbolic representations of needs. |
| Express need—written word | The participant is presented with written words corresponding to preferred items (e.g., water or toy) alongside distractors. When motivated, she is encouraged to indicate the written word that represents her current need by pointing, touching, or looking at it. A correct selection demonstrates the ability to recognize basic written vocabulary related to personal needs. |
| Match need to written word | The therapist presents a real object or situation (e.g., offering a snack or initiating an activity) and asks the participant to select the corresponding written word among distractors. Correct matching indicates an understanding of the association between real-world needs and their written linguistic representations. |
Appendix B
| Example of material used for object recognition (e.g., table) | ||
 | ||
| 1st Time |  |  |
| 2nd Time |  |  |
| 3rd Time |  |  |
| Example of material used for color discrimination (e.g., red). | ||
 | ||
| 1st Time |  |  |
| 2nd Time |  |  |
| 3rd Time |  |  |
| Example of material used for time discrimination (e.g., before). | ||
 | ||
| 1st Time |  |  |
| 2nd Time |  |  |
| 3rd Time |  |  |
| Example of material used for spatial concepts discrimination (e.g., inside). | ||
 | ||
| 1st Time |  |  |
| 2nd Time |  |  |
| 3rd Time |  |  |
| An example of the cards used for the ability to recognize and express a basic need through pictures |
 |
Appendix C
| Skills | t (Exp) | p (Exp) | Cohen’s d (Exp) | 95% CI (Exp) | t (Ctrl) | p (Ctrl) | Cohen’s d (Ctrl) | 95% CI (Ctrl) |
| Object Recognition | 4.40 | <0.001 | 1.63 | [0.98, 2.27] | 2.40 | 0.025 | 0.77 | [0.29, 1.25] |
| Object Permanence Recognition | 5.30 | <0.001 | 2.10 | [1.35, 2.86] | 4.90 | <0.001 | 1.95 | [1.23, 2.67] |
| Color Discrimination | 4.80 | <0.001 | 1.76 | [1.08, 2.43] | 5.30 | <0.001 | 2.10 | [1.35, 2.86] |
| Geometric Form Discrimination | 1.60 | 0.12 | 0.50 | [0.06, 0.95] | 1.60 | 0.12 | 0.50 | [0.06, 0.95] |
| Cause–Effect Relationship | 4.90 | <0.001 | 1.89 | [1.18, 2.59] | 5.70 | <0.001 | 2.42 | [1.58, 3.26] |
| Anticipation of Familiar Events | 6.80 | <0.001 | 3.29 | [2.22, 4.36] | 7.90 | <0.001 | 3.93 | [2.68, 5.18] |
| Object-Function Matching | 1.90 | 0.07 | 0.65 | [0.19, 1.12] | 1.80 | 0.08 | 0.63 | [0.17, 1.10] |
| Quantity Discrimination | 2.60 | 0.016 | 0.87 | [0.38, 1.37] | 2.30 | 0.03 | 0.76 | [0.28, 1.23] |
| Object Categorization by Function | 0.30 | 0.77 | 0.11 | [−0.32, 0.53] | −0.35 | 0.73 | −0.12 | [−0.54, 0.30] |
| Understanding Simple Sequences | 1.70 | 0.10 | 0.56 | [0.10, 1.01] | 2.30 | 0.03 | 0.76 | [0.28, 1.24] |
| Human Body Discrimination | −0.70 | 0.48 | −0.23 | [−0.66, 0.20] | −0.90 | 0.38 | −0.30 | [−0.73, 0.13] |
| Spatial Concepts | 5.40 | <0.001 | 1.98 | [1.25, 2.71] | 1.70 | 0.10 | 0.60 | [0.14, 1.06] |
| Measure Concepts | −0.70 | 0.48 | −0.23 | [−0.66, 0.19] | −0.70 | 0.48 | −0.23 | [−0.66, 0.19] |
| Time Concepts | 1.70 | 0.10 | 0.55 | [0.09, 1.00] | 1.60 | 0.12 | 0.50 | [0.05, 0.94] |
| Compound Means Score on Basic Cognitive Skills | 4.11 | <0.001 | 0.84 | [0.37, 1.30] | 2.92 | 0.08 | 0.61 | [0.16, 1.06] |
| Note. Inferential results (from T0 to T2) are reported here for each cognitive ability and group, and complement the descriptive data shown in Table 3 of the main manuscript. | ||||||||
Appendix D
| Skill | t (Exp) | p (Exp) | d (Exp) | 95% CI (Exp) | t (Ctrl) | p (Ctrl) | d (Ctrl) | 95% CI (Ctrl) |
| Object Recognition | 5.26 | <0.001 | 1.63 | [0.98, 2.27] | 3.18 | 0.004 | 0.77 | [0.29, 1.25] |
| Object Permanence Recognition | 6.72 | <0.001 | 2.10 | [1.35, 2.86] | 6.25 | <0.001 | 1.95 | [1.23, 2.67] |
| Color Discrimination | 5.65 | <0.001 | 1.76 | [1.08, 2.43] | 6.72 | <0.001 | 2.10 | [1.35, 2.86] |
| Geometric Form Discrimination | 1.94 | 0.065 | 0.50 | [0.06, 0.95] | 1.94 | 0.065 | 0.50 | [0.06, 0.95] |
| Cause–Effect Relationship | 6.09 | <0.001 | 1.89 | [1.18, 2.59] | 7.83 | <0.001 | 2.42 | [1.58, 3.26] |
| Anticipation of Familiar Events | 9.72 | <0.001 | 3.29 | [2.22, 4.36] | 11.60 | <0.001 | 3.93 | [2.68, 5.18] |
| Object–Function Matching | 2.70 | 0.012 | 0.65 | [0.19, 1.12] | 2.60 | 0.015 | 0.63 | [0.17, 1.10] |
| Quantity Discrimination | 3.33 | 0.003 | 0.87 | [0.38, 1.37] | 2.96 | 0.007 | 0.76 | [0.28, 1.23] |
| Object Categorization by Function | 0.45 | 0.655 | 0.11 | [−0.32, 0.53] | −0.49 | 0.627 | −0.12 | [−0.54, 0.30] |
| Understanding Simple Sequences | 2.29 | 0.031 | 0.56 | [0.10, 1.01] | 2.98 | 0.007 | 0.76 | [0.28, 1.24] |
| Human Body Discrimination | −1.05 | 0.305 | −0.23 | [−0.66, 0.20] | −1.37 | 0.184 | −0.30 | [−0.73, 0.13] |
| Spatial Concepts | 6.31 | <0.001 | 1.98 | [1.25, 2.71] | 2.55 | 0.018 | 0.60 | [0.14, 1.06] |
| Measure Concepts | −1.04 | 0.309 | −0.23 | [−0.66, 0.19] | −1.04 | 0.309 | −0.23 | [−0.66, 0.19] |
| Time Concepts | 2.26 | 0.033 | 0.55 | [0.09, 1.00] | 2.13 | 0.044 | 0.50 | [0.05, 0.94] |
| Compound Means Score on Communication Skills | 5.32 | <0.001 | 1.64 | [0.96, 2.32] | 4.18 | <0.001 | 1.04 | [0.47, 1.61] |
| Note. Inferential results (from T0 to T2) are reported here for each cognitive ability and group, and complement the descriptive data shown in Table 4 of the main manuscript. | ||||||||
References
- Amir, R.E.; Van den Veyver, I.B.; Wan, M.; Tran, C.Q.; Francke, U.; Zoghbi, H.Y. Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat. Genet. 1999, 23, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Amir, R.E.; Zoghbi, H.Y. Rett syndrome: Methyl-CpG-binding protein 2 mutations and phenotype-genotype correlations. Am. J. Med. Genet. 2000, 97, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, S.; Lumsden, D.E. Rett syndrome as a movement and motor disorder—A narrative review. Eur. J. Paediatr. Neurol. 2020, 28, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Urbańska, S.; Witas, A.; Borowska-Łygan, M.; Pięta, J. Understanding Rett syndrome: Genetic, clinical and therapeutic perspectives—Literature review. J. Educ. Health Sport 2025, 77, 57074. [Google Scholar] [CrossRef]
- Ramirez, J.M.; Karlen-Amarante, M.; Wang, J.J.; Huff, A.; Burgraff, N. Breathing disturbances in Rett syndrome. Handb. Clin. Neurol. 2022, 189, 139–151. [Google Scholar]
- Singh, J.; Santosh, P. Key issues in Rett syndrome: Emotional, behavioural and autonomic dysregulation (EBAD)—A target for clinical trials. Orphanet J. Rare Dis. 2018, 13, 128. [Google Scholar] [CrossRef]
- Percy, A.K.; Ananth, A.; Neul, J.L. Rett Syndrome: The Emerging Landscape of Treatment Strategies. CNS Drugs 2024, 38, 851–867. [Google Scholar] [CrossRef]
- Fabio, R.A.; Giannatiempo, S.; Perina, M. Overcoming Challenges in Learning Prerequisites for Adaptive Functioning: Tele-Rehabilitation for Young Girls with Rett Syndrome. J. Pers. Med. 2025, 15, 250. [Google Scholar] [CrossRef]
- Fabio, R.A.; Gangemi, A.; Semino, M.; Vignoli, A.; Priori, A.; Canevini, M.P.; Di Rosa, G.; Caprì, T. Effects of combined transcranial direct current stimulation with cognitive training in girls with Rett syndrome. Brain Sci. 2020, 10, 276. [Google Scholar] [CrossRef]
- Fonzo, M.; Sirico, F.; Corrado, B. Evidence-Based Physical Therapy for Individuals with Rett Syndrome: A Systematic Review. Brain Sci. 2020, 10, 410. [Google Scholar] [CrossRef]
- Caprì, T.; Fabio, R.A.; Iannizzotto, G.; Nucita, A. The TCTRS Project: A Holistic Approach for Telerehabilitation in Rett Syndrome. Electronics 2020, 9, 491. [Google Scholar] [CrossRef]
- Øra, H.P.; Kirmess, M.; Brady, M.C.; Partee, I.; Hognestad, R.B.; Johannessen, B.B.; Thommessen, B.; Becker, F. The effect of augmented speech-language therapy delivered by telerehabilitation on poststroke aphasia—A pilot randomized controlled trial. Clin. Rehabil. 2020, 34, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Niknejad, N.; Ismail, W.; Bahari, M.; Nazari, B. Understanding telerehabilitation technology to evaluate stakeholders’ adoption of telerehabilitation services: A systematic literature review and directions for further research. Arch. Phys. Med. Rehabil. 2021, 102, 1390–1403. [Google Scholar] [CrossRef]
- Romano, A.; Rodocanachi Roidi, M.L.; Savini, M.N.; Viganò, I.; Dziubak, M.; Pietrogrande, L.; Moran, D.S.; Lotan, M. Effects of a Supervised-As-Needed Home Exercise Program on Scoliosis and Motor Function in Rett Syndrome: A Multiple-Baseline Study. J. Clin. Med. 2025, 14, 1873. [Google Scholar] [CrossRef]
- Kocyigit, B.F.; Assylbek, M.I.; Yessirkepov, M. Telerehabilitation: Lessons from the COVID-19 pandemic and future perspectives. Rheumatol. Int. 2024, 44, 577–582. [Google Scholar] [CrossRef]
- Moulaei, K.; Sheikhtaheri, A.; Nezhad, M.S.; Haghdoost, A.; Gheysari, M.; Bahaadinbeigy, K. Telerehabilitation for upper limb disabilities: A scoping review on functions, outcomes, and evaluation methods. Arch. Public Health 2022, 80, 196. [Google Scholar] [CrossRef]
- Franco, J.B.; Maximino, L.P.; Barretti Secchi, L.L.; Antonelli, B.C.; Blasca, W.Q. What Are the Barriers to Telerehabilitation in the Treatment of Musculoskeletal Diseases? Port. J. Public Health 2023, 42, 33–42. [Google Scholar] [CrossRef]
- Kucharska, B. Health educators as assistants for disabled people in universal teaching institutions in Poland. Pediatr. Endocrinol. Diabetes Metab. 2019, 25, 36–40. [Google Scholar] [CrossRef]
- Grigorenko, E.L.; Compton, D.L.; Fuchs, L.S.; Wagner, R.K.; Willcutt, E.G.; Fletcher, J.M. Understanding, Educating, and Supporting Children with Specific Learning Disabilities: 50 Years of Science and Practice. Am. Psychol. 2020, 75, 37. [Google Scholar] [CrossRef]
- Romano, A.; Caprì, T.; Semino, M.; Bizzego, I.; Di Rosa, G.; Fabio, R.A. Gross motor, physical activity and musculoskeletal disorder evaluation tools for rett syndrome: A systematic review. Dev. Neurorehabilit. 2020, 23, 485–501. [Google Scholar] [CrossRef]
- Del Lucchese, B.; Parravicini, S.; Filogna, S.; Mangani, G.; Beani, E.; Di Lieto, M.C.; Bardoni, A.; Bertamino, M.; Papini, M.; Tacchino, C.; et al. The wide world of technological telerehabilitation for pediatric neurologic and neurodevelopmental disorders—A systematic review. Front. Public Health 2024, 12, 1295273. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; He, K.; Sui, X.; Yi, J.; Yang, Z.; Wang, K.; Gao, Y.; Bian, L.; Jiang, J.; Zhao, L. The Effect of Web-Based Telerehabilitation Programs on Children and Adolescents With Brain Injury: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2023, 25, e46957. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.; Kim, D.Y.; Park, S.-W.; Lee, B.-S.; Han, H.-W.; Jeon, N.; Kim, M.; Kang, M.; Kim, S. A systematic review of cognitive telerehabilitation in patients with cognitive dysfunction. Front. Neurol. 2025, 15, 1450977. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; Baglio, F.; Arcuri, F.; Borgnis, F.; Contrada, M.; Diaz, M.D.M.; Leochico, C.F.; Neira, N.J.; Laratta, S.; Suchan, B.; et al. Cognitive telerehabilitation: An expert consensus paper on current evidence and future perspective. Front. Neurol. 2024, 15, 1338873. [Google Scholar] [CrossRef]
- Fabio, R.A.; Caprì, T.; Iannizzotto, G.; Nucita, A.; Mohammadhasani, N. Interactive avatar boosts the performances of children with attention deficit hyperactivity disorder in dynamic measures of intelligence. Cyberpsychology Behav. Soc. Netw. 2019, 22, 588–596. [Google Scholar] [CrossRef]
- Tost, A.; Bachiller, A.; Medina-Rivera, I.; Romero, S.; Serna, L.Y.; Rojas-Martínez, M.; García-Cazorla, Á.; Mañanas, M.Á. Repetitive active and passive cognitive stimulations induce EEG changes in patients with Rett syndrome. Pediatr. Res. 2025, 97, 751–762. [Google Scholar] [CrossRef]
- Tost, A.; Romero, S.; Alonso, J.F.; Bachiller, A.; Serna, L.Y.; Medina-Rivera, I.; Garcia-Cazorla, A.; Mañanas, M.Á. EEG connectivity patterns in response to gaming and learning-based cognitive stimulations in Rett syndrome. Res. Dev. Disabil. 2024, 150, 104751. [Google Scholar] [CrossRef]
- Casalini, C.; Pecini, C. Telerehabilitation of Developmental Dyslexia: Critical Considerations on Intervention Methods and Their Effectiveness. Brain Sci. 2024, 14, 793. [Google Scholar] [CrossRef]
- Iannizzotto, G.; Nucita, A.; Fabio, R.A.; Caprì, T.; Lo Bello, L. Remote eye-tracking for cognitive telerehabilitation and interactive school tasks in times of COVID-19. Information 2020, 11, 296. [Google Scholar] [CrossRef]
- Fabio, R.A.; Semino, M.; Giannatiempo, S. The GAIRS checklist: A useful global assessment tool in patients with rett syndrome. Orphanet J. Rare Dis. 2022, 17, 116. [Google Scholar] [CrossRef]
- Fabio, R.A.; Martinazzoli, C.; Antonietti, A. Development and standardization of the “r.a.r.s” (Rett assessment rating scale). Life Span Disabil. 2005, 8, 257–281. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland ABS; Giunti Editore: Florence, Italy, 2013. [Google Scholar]
- Fisher, R.A. Statistical Methods for Research Workers, 14th ed.; Hafner: New York, NY, USA, 1973. [Google Scholar]
- Ciarmoli, D.; Stasolla, F. New Technologies to Support People with Neurodevelopmental Disorders: A Selective Review. OBM Neurobiol. 2023, 7, 1–32. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | AGE | RARS | VABSs | GAIRS Basic Cognitive Abilities | GAIRS Communication Abilities |
|---|---|---|---|---|---|
| Experimental Group | |||||
| 1 | 4 | 75.5 | 75 | 1.63 | 2.57 |
| 2 | 10 | 75.5 | 75 | 2.00 | 2.57 |
| 3 | 3 | 46 | 100 | 2.25 | 2.43 |
| 4 | 21 | 58 | 84 | 1.63 | 1.86 |
| 5 | 24 | 71 | 71 | 1.38 | 1.71 |
| 6 | 17 | 69.5 | 109 | 1.50 | 1.71 |
| 7 | 24 | 64 | 136 | 1.50 | 2.14 |
| 8 | 24 | 62 | 91 | 2.50 | 2.14 |
| 9 | 13 | 64 | 111 | 1.13 | 2.00 |
| 10 | 6 | 65.5 | 104 | 1.88 | 1.71 |
| 11 | 14 | 72 | 151 | 3.13 | 2.86 |
| 12 | 9 | 70 | 77 | 1.86 | 2.15 |
| Control Group | |||||
| 1 | 12 | 81.5 | 85 | 1.25 | 1.29 |
| 2 | 4 | 60.5 | 128 | 3.38 | 1.86 |
| 3 | 23 | 63.5 | 74 | 2.88 | 2.14 |
| 4 | 11 | 64.5 | 84 | 2.25 | 2.57 |
| 5 | 7 | 67.5 | 78 | 1.25 | 1.57 |
| 6 | 10 | 54 | 70 | 1 | 1.43 |
| 7 | 6 | 66.5 | 69 | 1 | 1.29 |
| 8 | 12 | 58 | 80 | 1.38 | 1.86 |
| 9 | 13 | 65 | 125 | 1.8 | 2.5 |
| 10 | 18 | 66 | 110 | 1.43 | 2.43 |
| 11 | 23 | 71 | 124 | 1.5 | 1.9 |
| 12 | 23 | 77 | 132 | 1.88 | 2.1 |
| Description | |
|---|---|
| Basic Cognitive Concepts | |
| Object Recognition | Identifies familiar objects among distractors based on visual characteristics. |
| Object Permanence Recognition | Understands that objects continue to exist even when out of sight. |
| Color Discrimination | Distinguishes and selects objects based on color differences. |
| Geometric Form Discrimination | Recognizes and differentiates basic geometric shapes. |
| Cause–Effect Relationship | Understands that specific actions lead to predictable outcomes. |
| Anticipation of Familiar Events | Anticipates routine events based on contextual or visual cues. |
| Object-Function Matching | Matches objects with their appropriate use or function. |
| Quantity Discrimination | Compares sets of objects based on quantity or number. |
| Object Categorization by Function | Groups objects according to shared functional properties. |
| Understanding Simple Sequences | Orders steps in simple routines or sequences correctly. |
| Human Body Discrimination | Recognizes and identifies body parts on self or images. |
| Spatial Concepts | Understands basic spatial terms (e.g., above, below, or near). |
| Measure Concepts | Differentiates objects based on size, weight, or length. |
| Time Concepts | Understands simple temporal relations (e.g., before, after, or now). |
| Communication Abilities | |
| Respond to Name/Verbal Prompt | Reacts to being called or prompted by turning, looking, or acknowledging. |
| Express Need—Non-Verbal | Requests items or actions through gestures, gaze, or pointing. |
| Express Refusal—Non-Verbal | Indicates rejection using body language or facial expression. |
| Shared Attention (Gaze Alternation) | Alternates gaze between person and object to share focus. |
| Understanding Gestures from Others | Responds appropriately to familiar social gestures. |
| Use Context-Based Vocalizations | Produces contextually relevant sounds or vocal patterns. |
| Participate in Routine Exchanges | Engages in turn-taking or structured social interaction routines. |
| Express Need—Picture | Uses images to communicate wants or needs. |
| Match Need to Picture | Identifies images corresponding to presented needs or objects. |
| Express Need—Written words | Uses written words to communicate wants or needs. |
| Match Need to Written Word | Identifies written words corresponding to presented needs or objects. |
| Skills | Group | Baseline (T0) | 3 Months (T1) | 6 Months (T2) | 9-Month Follow-Up (T3) |
|---|---|---|---|---|---|
| Object recognition | Experimental | 2.80 (1.48) | 3.56 (1.33) | 4.80 (0.91) * | 4.18 (0.94) * |
| Control | 2.84 (1.21) | 3.22 (1.01) | 3.65 (0.88) | 3.72 (1.01) | |
| Object permanence recognition | Experimental | 1.80 (0.42) | 2.89 (1.45) | 3.33 (0.94) | 3.20 (0.91) |
| Control | 1.90 (0.43) | 3.00 (1.45) | 3.34 (0.95) | 3.10 (0.88) | |
| Color discrimination | Experimental | 1.73 (0.42) | 2.33 (1.45) | 3.01 (0.94) | 3.20 (0.66) |
| Control | 1.80 (0.42) | 2.22 (1.45) | 3.33 (0.94) | 3.19 (0.91) | |
| Geometric form discrimination | Experimental | 1.70 (1.33) | 2.00 (1.00) | 2.35 (1.25) | 2.21 (1.20) |
| Control | 1.70 (1.33) | 2.00 (1.00) | 2.35 (1.25) | 2.21 (1.20) | |
| Cause–effect relationship | Experimental | 1.00 (0.00) | 1.30 (0.22) | 1.88 (0.66) | 1.80 (0.65) |
| Control | 1.00 (0.00) | 1.20 (0.32) | 1.77 (0.45) | 1.70 (0.33) | |
| Anticipation of familiar events | Experimental | 1.00 (0.00) | 1.70 (0.27) | 2.00 (0.43) | 1.99 (0.41) |
| Control | 1.00 (0.00) | 1.63 (0.29) | 2.00 (0.36) | 1.87 (0.47) | |
| Object-function matching | Experimental | 1.60 (1.10) | 2.00 (1.00) | 2.30 (1.05) | 2.30 (1.03) |
| Control | 1.58 (1.22) | 1.99 (0.99) | 2.30 (1.05) | 2.32 (0.66) | |
| Quantity discrimination | Experimental | 1.40 (1.00) | 2.10 (0.90) | 2.25 (0.95) | 2.28 (0.91) |
| Control | 1.32 (0.89) | 1.77 (0.90) | 2.00 (0.91) | 2.11 (0.83) | |
| Object categorization by function | Experimental | 2.20 (0.95) | 2.40 (0.77) | 2.30 (0.93) | 2.05 (0.90) |
| Control | 2.10 (0.75) | 2.34 (0.90) | 2.00 (0.91) | 2.10 (0.77) | |
| Understanding simple sequences | Experimental | 2.30 (1.00) | 2.00 (0.95) | 2.85 (0.98) | 2.98 (0.95) |
| Control | 2.20 (0.91) | 1.80 (0.90) | 2.90 (0.93) | 2.95 (0.90) | |
| Human body discrimination | Experimental | 2.40 (1.07) | 1.89 (1.17) | 2.15 (1.12) | 2.20 (1.10) |
| Control | 2.33 (1.07) | 1.77 (0.89) | 2.00 (1.12) | 2.10 (0.88) | |
| Spatial concepts | Experimental | 1.50 (0.53) | 1.83 (0.50) | 2.53 (0.51) * | 2.45 (0.50) * |
| Control | 1.50 (0.53) | 1.73 (0.67) | 1.92 (0.83) | 2.00 (0.81) | |
| Measure concepts | Experimental | 2.40 (0.97) | 2.00 (0.50) | 2.20 (0.73) | 2.25 (0.75) |
| Control | 2.40 (0.97) | 2.00 (0.50) | 2.20 (0.73) | 2.25 (0.75) | |
| Time concepts | Experimental | 1.30 (0.48) | 1.44 (0.53) | 1.57 (0.51) | 1.40 (0.50) |
| Control | 1.22 (0.72) | 1.50 (0.72) | 1.53 (0.51) | 1.39 (0.77) |
| Skills/Groups | Baseline (T0) | 3 Months (T1) | 6 Months (T2) | 9-Month Follow-Up (T3) |
|---|---|---|---|---|
| 1. Respond to name/verbal prompt | ||||
| Experimental | 3.50 (0.80) | 3.70 (0.70) | 4.20 (0.70) | 4.10 (0.60) |
| Control | 3.20 (0.90) | 3.30 (0.90) | 3.80 (0.80) | 3.70 (0.80) |
| 2. Express need—non-verbal | ||||
| Experimental | 3.80 (0.63) | 4.10 (0.57) | 4.50 (1.08) | 4.20 (1.08) |
| Control | 3.25 (0.89) | 3.75 (0.89) | 4.17 (0.84) | 3.97 (0.84) |
| 3. Express refusal—non-verbal | ||||
| Experimental | 3.00 (0.90) | 3.30 (0.90) | 3.60 (0.80) | 3.50 (0.80) |
| Control | 2.70 (1.00) | 3.10 (1.00) | 3.50 (0.90) | 3.00 (0.90) |
| 4. Shared attention (gaze alternation) | ||||
| Experimental | 2.90 (1.00) | 3.10 (1.00) | 3.80 (0.90) | 3.90 (0.90) |
| Control | 2.50 (1.10) | 2.70 (1.10) | 3.20 (1.00) | 3.70 (1.00) |
| 5. Understanding gestures from others | ||||
| Experimental | 2.30 (0.90) | 3.50 (0.80) | 3.60 (0.70) | 3.70 (0.70) |
| Control | 2.20 (0.90) | 3.30 (0.90) | 3.40 (0.80) | 3.30 (0.80) |
| 6. Use context-based vocalizations | ||||
| Experimental | 2.10 (1.00) | 2.30 (0.90) | 2.40 (0.90) | 2.45 (0.80) |
| Control | 2.00 (1.00) | 2.10 (1.00) | 2.30 (0.90) | 2.10 (0.90) |
| 7. Participate in routine exchanges | ||||
| Experimental | 2.20 (0.90) | 2.40 (0.80) | 2.50 (0.80) | 2.60 (0.70) |
| Control | 2.30 (1.00) | 2.40 (0.90) | 2.50 (0.90) | 2.40 (0.90) |
| 8. Express need—picture | ||||
| Experimental | 1.50 (1.27) | 2.20 (1.03) | 2.50 (1.18) | 2.60 (1.15) |
| Control | 1.78 (1.36) | 2.05 (1.39) | 2.35 (1.55) | 2.40 (1.50) |
| 9. Match need to picture | ||||
| Experimental | 2.10 (1.10) | 2.40 (1.10) | 2.80 (1.23) | 2.90 (1.20) |
| Control | 1.90 (1.07) | 2.13 (1.25) | 2.63 (1.30) | 2.70 (1.25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabio, R.A.; Giannatiempo, S.; Perina, M. At-School Telerehabilitation for Rett Syndrome: Support Teachers Driving Cognitive and Communication Progress in a Randomized Trial. Children 2025, 12, 928. https://doi.org/10.3390/children12070928
Fabio RA, Giannatiempo S, Perina M. At-School Telerehabilitation for Rett Syndrome: Support Teachers Driving Cognitive and Communication Progress in a Randomized Trial. Children. 2025; 12(7):928. https://doi.org/10.3390/children12070928
Chicago/Turabian StyleFabio, Rosa Angela, Samantha Giannatiempo, and Michela Perina. 2025. "At-School Telerehabilitation for Rett Syndrome: Support Teachers Driving Cognitive and Communication Progress in a Randomized Trial" Children 12, no. 7: 928. https://doi.org/10.3390/children12070928
APA StyleFabio, R. A., Giannatiempo, S., & Perina, M. (2025). At-School Telerehabilitation for Rett Syndrome: Support Teachers Driving Cognitive and Communication Progress in a Randomized Trial. Children, 12(7), 928. https://doi.org/10.3390/children12070928