
Rapid, Safe, and Tolerable Healing of Pediatric Skin Injuries with Blue Light Therapy: An Observational Case Series




Abstract
1. Introduction
2. Materials and Methods
Intervention
3. Results
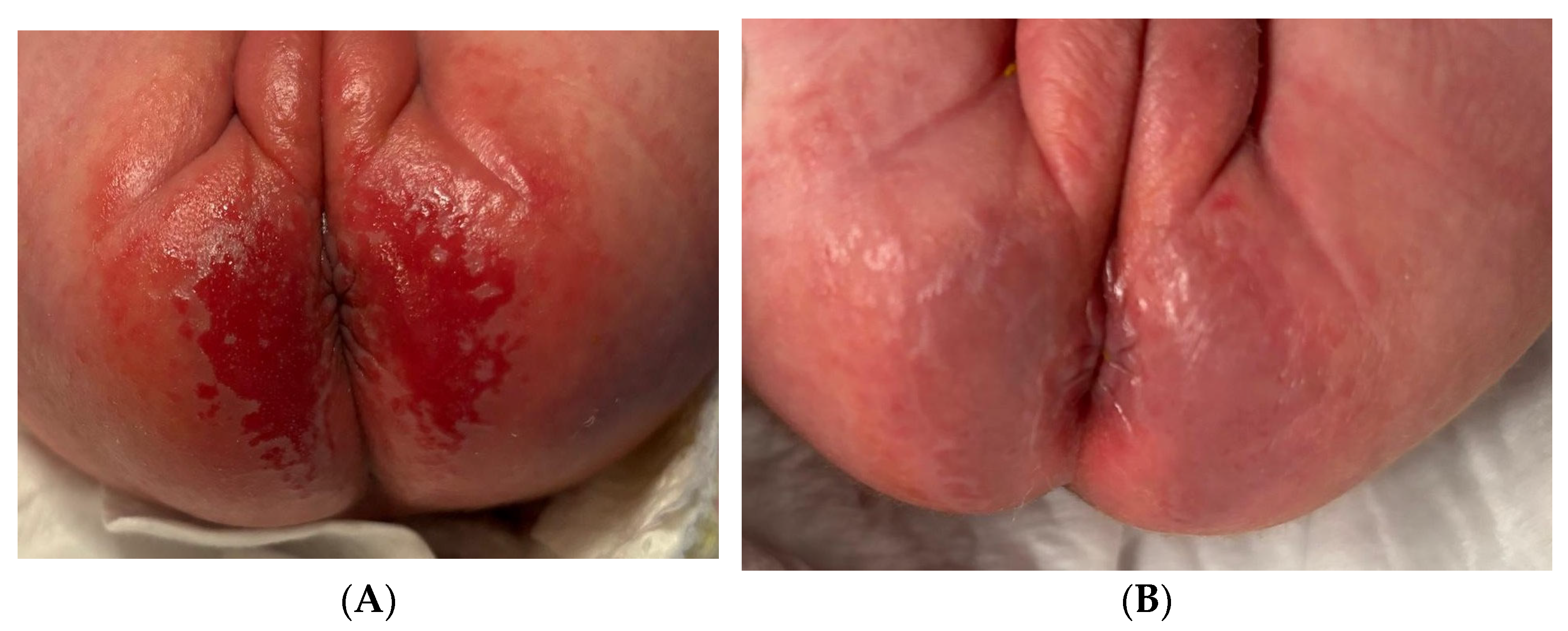
3.1. Case 1
3.2. Case 2
3.3. Case 3
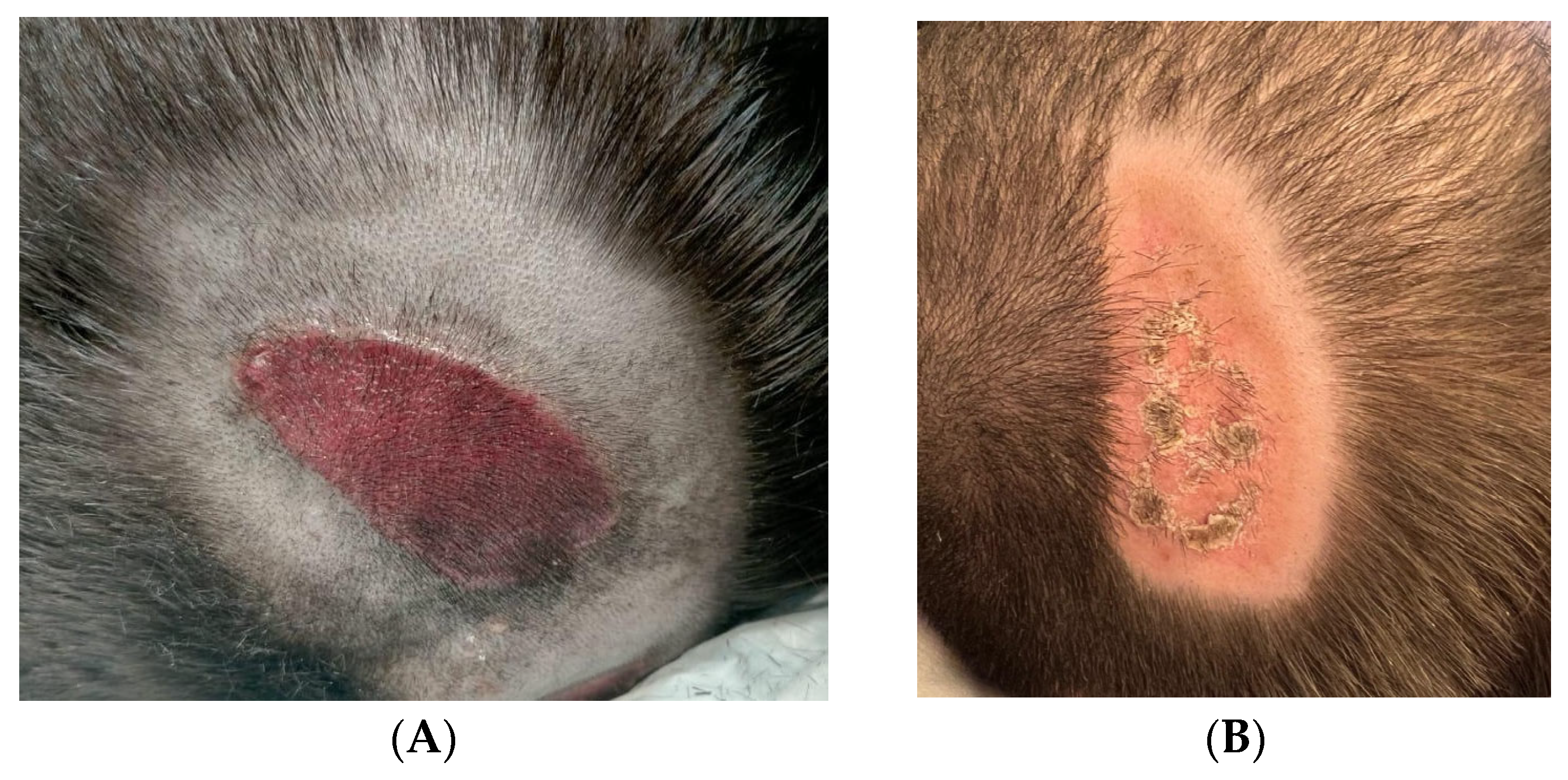
3.4. Case 4
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCord, S.S.; Levy, M.L. Practical guide to pediatric wound care. Semin. Plast. Surg. 2006, 20, 192–199. [Google Scholar] [CrossRef]
- Visscher, M.O.; Burkes, S.A.; Adams, D.M.; Hammill, A.M.; Wickett, R.R. Infant skin maturation: Preliminary outcomes for color and biomechanical properties. Skin Res. Technol. 2017, 23, 545–551. [Google Scholar] [CrossRef]
- Nie, A.M.; Johnson, D.; Reed, R.C. Neonatal Skin Structure: Pressure Injury Staging Challenges. Adv. Skin Wound Care 2022, 35, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Ciprandi, G. (Ed.) Neonatal and Pediatric Wound Care; Edizioni Minerva Medica: Torino, Italy, 2021. [Google Scholar]
- Nicolosi, B.; Parente, E.; Fontani, I.; Idrizaj, S.; Stringi, D.; Bamonte, C.; Longobucco, Y.; Buccione, E.; Maffeo, M.; Granai, V.; et al. Risk Factors for Skin Injuries in Hospitalized Children: A Retrospective Study. Inferm. J. 2024, 3, 277–285. [Google Scholar] [CrossRef]
- Smith, H.A.; Moore, Z.; Mong, H.T. Cohort study to determine the risk of pressure ulcers and developing a care bundle within a paediatric intensive care unit setting. Intensive Crit. Care Nurs. 2019, 53, 68–72. [Google Scholar] [CrossRef]
- Fraccalvieri, M.; Amadeo, G.; Bortolotti, P.; Ciliberti, M.; Garrubba, A.; Mosti, G.; Bianco, S.; Mangia, A.; Massa, M.; Hartwig, V.; et al. Effectiveness of Blue light photobiomodulation therapy in the treatment of chronic wounds. Results of the Blue Light for Ulcer Reduction (B.L.U.R.) Study. Ital. J. Dermatol. Venerol. 2022, 157, 187–194. [Google Scholar] [CrossRef]
- Dollaku, H.; Dalladonna, M.; Giuliano, M.; Rossi, M.; Barbetti, P.; Marcolongo, M.S.; Buccione, E.; Iovino, P.; Macchi, C. Randomized clinical trial of the efficacy of the EmoLED medical device in the treatment of stage 2 and stage 3 pressure ulcers: The RISE_UP study. J. Tissue Viability 2025, 34, 100895. [Google Scholar] [CrossRef]
- Ricci, E.; Pittarello, M. Blue light photobiomodulation for reactivation of healing in wounds not responding to standard therapy. J. Wound Care 2023, 32, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Spinella, A.; de Pinto, M.; Galluzzo, C.; Testoni, S.; Macripo, P.; Lumetti, F.; Parenti, L.; Magnani, L.; Sandri, G.; Bajocchi, G.; et al. Photobiomodulation Therapy: A New Light in the Treatment of Systemic Sclerosis Skin Ulcers. Rheumatol. Ther. 2022, 9, 891–905. [Google Scholar] [CrossRef]
- Nair, H.R.; Khalib, M.A.A.; Rashid, R.; Ng, M.L. Blue Light Empirical Shine Study (BLESS) trial: A pilot case series. Wounds APAC 2023, 6, 39–47. [Google Scholar]
- Magni, G.; Banchelli, M.; Cherchi, F.; Coppi, E.; Fraccalvieri, M.; Rossi, M.; Tatini, F.; Pugliese, A.M.; Rossi Degl’Innocenti, D.; Alfieri, D.; et al. Experimental Study on Blue Light Interaction with Human Keloid-Derived Fibroblasts. Biomedicines 2020, 8, 573. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Magni, G.; Tatini, F.; Banchelli, M.; Cherchi, F.; Rossi, M.; Coppi, E.; Pugliese, A.M.; Rossi Degl’Innocenti, D.; Alfieri, D.; et al. Photobiomodulation of Human Fibroblasts and Keratinocytes with Blue Light: Implications in Wound Healing. Biomedicines 2021, 9, 41. [Google Scholar] [CrossRef]
- Cicchi, R.; Rossi, F.; Alfieri, D.; Bacci, S.; Tatini, F.; De Siena, G.; Paroli, G.; Pini, R.; Pavone, F.S. Observation of an improved healing process in superficial skin wounds after irradiation with a blue-LED haemostatic device. J. Biophotonics 2016, 9, 645–655. [Google Scholar] [CrossRef]
- Beeckman, D.; Van den Bussche, K.; Alves, P.; Beele, H.; Ciprandi, G.; Coyer, F.; de Groot, T.; De Meyer, D.; Dunk, , A.M.; Fouri, A.; et al. The Ghent Global IAD Categorisation Tool (GLOBIAD). Ghent University. 2017. Available online: www.UCVVGent.be (accessed on 13 May 2025).
- Villa, G.; Crafa, A.; Denti, F.; Grilli, M.; Passafiume, S.; Sarritzu, G.; Spena, P.R.; Maculotti, D. SACS Evolution: A peristomal health tool for the prevention of peristomal skin disorders. Minerva Surg. 2021, 76, 423–428. [Google Scholar] [CrossRef]
- Woo, K.Y.; Sibbald, R.G. A cross-sectional validation study of using NERDS and STONEES to assess bacterial burden. Ostomy Wound Manag. 2009, 55, 40–48. [Google Scholar]
- European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline. Haesler E, editor. EPUAP/NPIAP/PPPIA; 2025. Available online: https://internationalguideline.com (accessed on 13 May 2025).
- Hillman, B.A.; Tabrizi, M.N.; Gauda, E.B.; Carson, K.A.; Aucott, S.W. The Neonatal Pain, Agitation and Sedation Scale and the bedside nurse’s assessment of neonates. J. Perinatol. 2015, 35, 128–131. [Google Scholar] [CrossRef]
- Crellin, D.J.; Harrison, D.; Santamaria, N.; Huque, H.; Babl, F.E. The Psychometric Properties of the FLACC Scale Used to Assess Procedural Pain. J. Pain 2018, 19, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.L.; Baker, C.M. Pain in children: Comparison of assessment scales. Pediatr. Nurs. 1988, 14, 9–17. [Google Scholar] [PubMed]
- Kleinpenning, M.M.; Smits, T.; Frunt, M.H.; van Erp, P.E.; van de Kerkhof, P.C.; Gerritsen, R.M. Clinical and histological effects of blue light on normal skin. Photodermatol. Photoimmunol. Photomed. 2010, 26, 16–21. [Google Scholar] [CrossRef]
- Aliquò, M.S.; Favuzza, L.; Priola, L.; Corrao, S. Clinical application of photobiomodulation with blue light on non-healing ulcers in diabetic patients: A case series study. Wounds Intern. 2021, 12, 5. [Google Scholar]
- Dini, V.; Romanelli, M.; Oranges, T.; Davini, G.; Janowska, A. Blue light emission in the management of hard to heal wounds: A case series. G Ital. Dermatol. Venereol. 2021, 156, 709–713. [Google Scholar] [CrossRef]
- Khoo, V.B.; Soon, S.; Yap, C.J.; Chng, S.P.; Tang, T.Y. Use of Blue Light in the Management of Chronic Venous Ulcer in Asian Patients: A Case Series. Cureus 2021, 13, e17703. [Google Scholar] [CrossRef]
- Nair, H.K.; Sulong, M.A.A.B.M. Effects of photobiomodulation with blue light on diabetic foot ulcers: A case series report. Wounds Asia 2021, 4, 6. [Google Scholar]
- Pezzuto, C.; Felisi, N.; Crispini, N.; Rosso, I. Use of photobiomodulation with blue light in the treatment of ulcers of various etiology in spinal cord injured patients: A case series. Ital. J. Wound Care 2023, 7. [Google Scholar] [CrossRef]
- Morgante, A.; Li Destri, A. Blue light therapy. An alternative approach for treatment of vascular skin ulcers. Ann. Ital. Chir. 2023, 93, 300–302. [Google Scholar] [PubMed]
- Conti, A.; Brilli, M.; Norgini, E.; Falini, S.; De Fina, L.; Spargi, G.; Gasperini, S. Blue light photobiomodulation: A therapy to reactivate the healing process of stagnant wounds of different aetiologies. Wound Int. 2023, 14, 41–45. [Google Scholar]
- Fletcher, J.; Beeckman, D.; Kottner, J. Best Practice Recommendations for Prevention and Management of Moisture-Associated Skin Damage (MASD); Wounds International: London, UK, 2020. [Google Scholar]
- Ministero della Salute. Decreto 30 Novembre 2021. Misure Volte a Facilitare e Sostenere la Realizzazione degli Studi Clinici di Medicinali Senza Scopo di Lucro e degli Studi Osservazionali. Gazzetta Ufficiale della Repubblica Italiana. 2022 Feb 19; Serie Generale n.42. Available online: https://www.gazzettaufficiale.it/eli/id/2022/02/19/22A01189/SG (accessed on 13 May 2025).
- Gefen, A.; Alves, P.; Ciprandi, G.; Clark, M.; Coyer, F.; Milne, C.T.; Ousey, K.; Patton, D.; Phillips, P.; Santamaria, N. Device-related pressure ulcers: SECURE prevention. Second edition. J. Wound Care 2022, 31, S1–S60. [Google Scholar] [CrossRef]
- Wounds UK. Best Practice Statement: Principles of Wound Management in Paediatric Patients (Second Edition). 2024. Available online: http://wounds-uk.com/best-practice-statements/principles-of-wound-management-in-paediatric-patients-second-edition (accessed on 13 May 2025).
- Woo, K.Y.; Beeckman, D.; Chakravarthy, D. Management of Moisture-Associated Skin Damage: A Scoping Review. Adv. Skin Wound Care 2017, 30, 494–501. [Google Scholar] [CrossRef]
- European Parliament and Council of the European Union. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data (General Data Protection Regulation). Off. J. Eur. Union 2016, L119, 1–88. Available online: https://eur-lex.europa.eu/legal-content/IT/TXT/PDF/?uri=CELEX%3A32016R0679 (accessed on 13 May 2025).
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). ICH Harmonised Guideline: Integrated Addendum to ICH E6(R3)—Guideline for Good Clinical Practice. 2024. Available online: https://database.ich.org/sites/default/files/ICH_E6%28R3%29_Step4_FinalGuideline_2025_0106.pdf (accessed on 13 May 2025).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age at Treatment | Sex | Stage | Localization | Applications Performed/ Duration | Healing Time (Days) | Outcome | Note |
|---|---|---|---|---|---|---|---|---|
| IAD | ||||||||
| Esophageal atresia in prematurity (Case 1) | 33 + 1 weeks GA | F | GLOBIAD 2A | Perineal | 2 After 3 days from 1st (60″) | 5 | H | |
| Myelomeningocele | 37 + 2 weeks GA | M | GLOBIAD 2A | Perineal | 1 (120″) | 4 | H | |
| Anorectal malformation (ARM) post-recanalization | 6 months | F | GLOBIAD 2B (Candida) | Perineal | 2 Every 3 days from 1st (120″) | 6 | H | 2nd dressing DACC |
| Anorectal malformation (ARM) post-recanalization | 7 months | F | GLOBIAD 1B | Perineal | 1 (120″) | 2 | H | 2nd dressing DACC |
| p-MASD | ||||||||
| Stoma in anorectal malformation (ARM) (Case 2) | 34 Weeks GA | M | SACS 2.0 T5-L3 with local infection and complicated surgical wound | Peristomal | 2 Every 3 days from 1st (60″) | 6 | PH | Dressing DACC |
| Stoma in anorectal malformation (ARM) | 36 + 2 weeks GA | M | SACS 2.0 T5-L2 | Peristomal | 1 (60″) | 3 | H | |
| Gastrostomy in short bowel syndrome (SBS) | 4 months | M | SACS T5-L2 | Abdomen | 1 (120″) | 3 | H | Thin foam |
| Crohn’s disease | 12 years | F | SACS T5-L2 | Peristomal | 2 After 3 days from 1st (120″) | 5 | H | |
| PIs and MDRPIs | ||||||||
| PI in spastic tetraparesis | 8 years | M | Suspected deep damage | Sacrum | 2 After 3 days from 1st (120″) | 5 | H | |
| MDRPI post-cast removing (Case 3) | 9 years | M | Outcome of unstageable injury | Heel | 4 Every 3 days from 1st (120″) | 13 | H | Dressing DACC |
| MDRPI (tracheostomy tube) in polytrauma | 11 years | M | 3rd EPUAP | Sternum handlebar | 3 Every 3 days from 1st (120″) | 8 | H | Gelling fiber |
| MDRPI (total face mask) in respiratory failure and infection (Case 4) | 12 years | M | 2nd EPUAP | Occiput | 2 Every 3 days from 1st (120″) | 5 | H | Silicon layer |
| N-PASS | ||||||
|---|---|---|---|---|---|---|
| GA (Weeks + Days) | Facial Expression | Cry Irritability | Extremities Tone | Behavior State | Vital Signs | Total Score |
| 33 + 1 | 0 | 1 | 1 | 1 | 0 | 3 |
| 34 | 0 | 1 | 1 | 0 | 0 | 2 |
| 36 + 2 | 0 | 1 | 0 | 1 | 1 | 3 |
| 37 + 2 | 0 | 0 | 0 | 0 | 0 | 0 |
| FLACC | ||||||
| Age (months) | Face | Legs | Activity | Cry | Consolability | Total Score |
| 4 | 1 | 0 | 1 | 0 | 0 | 2 |
| 6 | 0 | 1 | 1 | 0 | 0 | 2 |
| 7 | 0 | 1 | 0 | 1 | 0 | 2 |
| Wong–Baker FACES Pain Rating Scale | ||||||
| Age (years) | Face description | Wong-Baker score | ||||
| 8 | Smiling face, quiet, no signs of pain | 0—No Hurt | ||||
| 9 | Neutral face, quiet, only slight restlessness | 0—No Hurt | ||||
| 11 | Face relaxed, no signs of distress | 0—No Hurt | ||||
| 12 | Smiling face, slight agitation, but no signs of pain | 0—No Hurt | ||||
| 13 | Quiet face, slightly pensive, but no pain | 0—No Hurt | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolosi, B.; Bastarelli, E.; Gregorini, M.; Ciprandi, G. Rapid, Safe, and Tolerable Healing of Pediatric Skin Injuries with Blue Light Therapy: An Observational Case Series. Children 2025, 12, 801. https://doi.org/10.3390/children12060801
Nicolosi B, Bastarelli E, Gregorini M, Ciprandi G. Rapid, Safe, and Tolerable Healing of Pediatric Skin Injuries with Blue Light Therapy: An Observational Case Series. Children. 2025; 12(6):801. https://doi.org/10.3390/children12060801
Chicago/Turabian StyleNicolosi, Biagio, Eleonora Bastarelli, Mirco Gregorini, and Guido Ciprandi. 2025. "Rapid, Safe, and Tolerable Healing of Pediatric Skin Injuries with Blue Light Therapy: An Observational Case Series" Children 12, no. 6: 801. https://doi.org/10.3390/children12060801
APA StyleNicolosi, B., Bastarelli, E., Gregorini, M., & Ciprandi, G. (2025). Rapid, Safe, and Tolerable Healing of Pediatric Skin Injuries with Blue Light Therapy: An Observational Case Series. Children, 12(6), 801. https://doi.org/10.3390/children12060801