
Detecting Disordered Eating Behaviors in Greek Youth with Type 1 Diabetes Mellitus by Using the Diabetes Eating Problem Survey—Revised (DEPS-R): Associations with Insulin Restriction, Glycemic Control, and Anthropometric Parameters

 ,
,  ,
,  , , , , and
, , , , and 
Abstract

1. Introduction
2. Materials and Methods
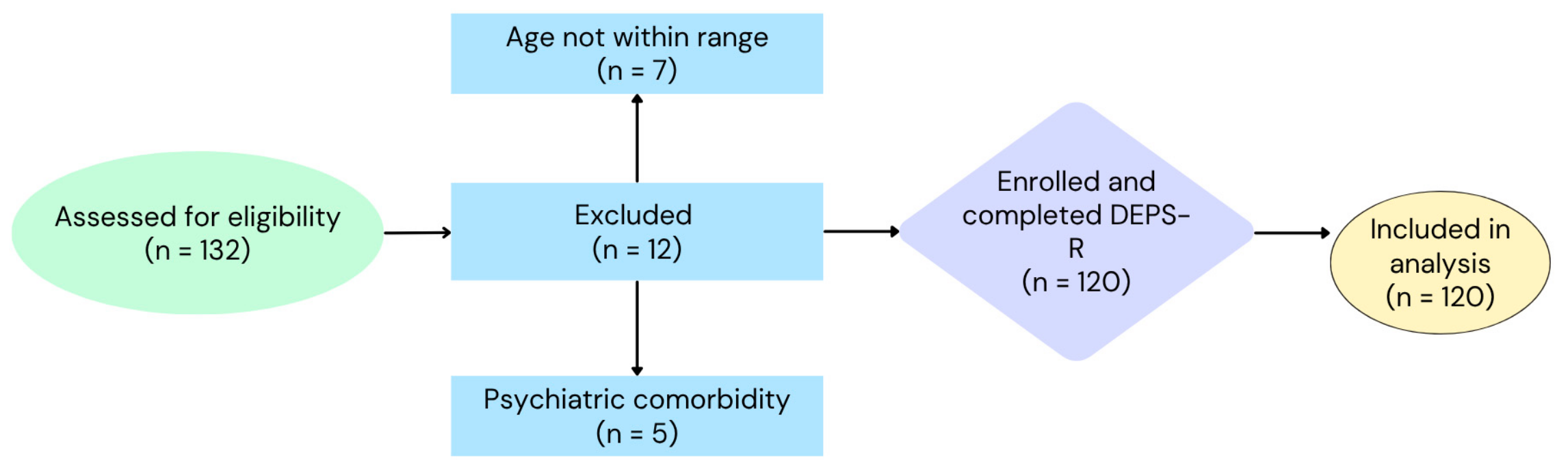
2.1. Study Population
2.2. Study Tools
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
DEPS-R Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CDC | Centers for Disease Control and Prevention |
| DEPS-R | Diabetes Eating Problem Survey—Revised |
| DEB | disordered eating behavior |
| ED | eating disorder |
| HbA1c | Glycated Hemoglobin |
| PCOS | Polycystic Ovary Syndrome |
| T1DM | Type 1 Diabetes Mellitus |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Boys | Girls | p | Total | |
|---|---|---|---|---|
| Total Score | 13.89 ± 8.62 | 20.56 ± 12.34 | 0.003 | 17.17 ± 11.09 |
| Losing weight is an important goal to me | 1.62 ± 1.60 | 2.61 ± 1.66 | <0.001 | 2.11 ± 1.70 |
| I skip main meals and/or snacks | 1.39 ± 1.14 | 1.80 ± 1.44 | 0.161 | 1.59 ± 1.31 |
| Other people have told me that my eating is out of control | 1.03 ± 1.33 | 1.42 ± 1.56 | 0.229 | 1.23 ± 1.45 |
| When I overeat, I don’t take enough insulin | 1.01 ± 1.18 | 1.22 ± 1.20 | 0.260 | 1.12 ± 1.19 |
| I eat more when I am alone than when I am with others | 1.23 ± 1.40 | 1.67 ± 1.46 | 0.071 | 1.45 ± 1.44 |
| I feel that it’s difficult to lose weight and control my diabetes at the same time | 0.72 ± 1.10 | 1.93 ± 1.80 | <0.001 | 1.32 ± 1.60 |
| Ι avoid checking my blood sugar when I feel it is out of range | 1.11 ± 1.34 | 0.98 ± 1.11 | 0.825 | 1.05 ± 1.23 |
| I make myself vomit | 0.07 ± 0.25 | 0.34 ± 0.82 | 0.036 | 0.20 ± 0.62 |
| I try to keep my blood sugar high so that I will lose weight | 0.46 ± 1.29 | 0.68 ± 1.23 | 0.126 | 0.57 ± 1.28 |
| I eat in a way to get ketones | 0.20 ± 0.65 | 0.17 ± 0.50 | 0.604 | 0.18 ± 0.58 |
| I feel fat when I take all of my insulin | 0.18 ± 0.62 | 0.54 ± 1.04 | 0.022 | 0.36 ± 0.87 |
| Other people tell me to take better care of my diabetes | 1.41 ± 1.53 | 1.98 ± 1.61 | 0.041 | 1.69 ± 1.59 |
| After I overeat, I skip my next insulin dose. | 0.61 ± 1.05 | 0.66 ± 0.94 | 0.451 | 0.63 ± 1.00 |
| I feel that my eating is out of control | 1.18 ± 1.19 | 1.61 ± 1.41 | 0.103 | 1.39 ± 1.32 |
| I alternate between eating very little and eating huge amounts | 1.13 ± 1.13 | 1.71 ± 1.53 | 0.060 | 1.42 ± 1.37 |
| I would rather be thin than to have good control of my diabetes | 0.52 ± 1.21 | 1.22 ± 1.78 | 0.042 | 0.87 ± 1.55 |
References
- Marks, B.E.; Wolfsdorf, J.I. Monitoring of pediatric type 1 diabetes. Front. Endocrinol. 2020, 11, 128. [Google Scholar] [CrossRef] [PubMed]
- Harjutsalo, V.; Sjöberg, L.; Tuomilehto, J. Time trends in the incidence of type 1 diabetes in Finnish children: A cohort study. Lancet 2008, 371, 1777–1782. [Google Scholar] [CrossRef] [PubMed]
- Neu, A.; Bürger-Büsing, J.; Danne, T.; Dost, A.; Holder, M.; Holl, R.W.; Holterhus, P.M.; Kapellen, T.; Karges, B.; Kordonouri, O.; et al. Diagnosis, therapy and follow-up of diabetes mellitus in children and adolescents. Exp. Clin. Endocrinol. Diabetes 2019, 127, 39–72. [Google Scholar] [CrossRef]
- Couper, J.J.; Haller, M.J.; Ziegler, A.G.; Knip, M.; Ludvigsson, J.; Craig, M.E. Phases of type 1 diabetes in children and adolescents. Pediatr. Diabetes 2014, 15, 18–25. [Google Scholar] [CrossRef]
- Ekman, I.; Vuorinen, T.; Knip, M.; Veijola, R.; Toppari, J.; Hyöty, H.; Kinnunen, T.; Ilonen, J.; Lempainen, J. Early childhood CMV infection may decelerate the progression to clinical type 1 diabetes. Pediatr. Diabetes 2019, 20, 73–77. [Google Scholar] [CrossRef]
- Awadalla, N.; Hegazy, A.; Abd El-Salam, M.; Elhady, M. Environmental factors associated with type 1 diabetes development: A case control study in Egypt. Int. J. Environ. Res. Public Health 2017, 14, 615. [Google Scholar] [CrossRef]
- King, P.S.; Berg, C.A.; Butner, J.; Butler, J.M.; Wiebe, D.J. Longitudinal trajectories of parental involvement in type 1 diabetes and adolescents’ adherence. Health Psychol. 2014, 33, 424–432. [Google Scholar] [CrossRef]
- Yancy, W.S.; Dunbar, S.A.; Boucher, J.L.; Cypress, M.; Evert, A.B.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Urbanski, P.; Verdi, C.L.; et al. Response to comments on Evert et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 2014, 37, 102–103. [Google Scholar] [CrossRef]
- Smart, C.; Aslander-van Vliet, E.; Waldron, S. Nutritional management in children and adolescents with diabetes. Pediatr. Diabetes 2009, 10, 100–117. [Google Scholar] [CrossRef]
- Cameron, F.J.; Garvey, K.; Hood, K.K.; Acerini, C.L.; Codner, E. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetes in adolescence. Pediatr. Diabetes 2018, 19, 250–261. [Google Scholar] [CrossRef]
- Schweizer, R.; Lösch-Binder, M.; Hayn, C.; Friz, S.; Uber, J.; Ziegler, J.; Liebrich, F.; Neu, A. Transition from childhood to adult care in patients with type 1 diabetes: 20 years of experience from the Tübinger Transition Study. Exp. Clin. Endocrinol. Diabetes 2023, 131, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Cecilia-Costa, R.; Volkening, L.K.; Laffel, L.M. Factors associated with disordered eating behaviours in adolescents with type 1 diabetes. Diabet. Med. 2019, 36, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Zarifsaniey, N.; Shirazi, M.O.; Mehrabi, M.; Bagheri, Z. Promoting self-management behaviors in adolescents with type 1 diabetes, using digital storytelling: A pilot randomized controlled trial. BMC Endocr. Disord. 2022, 22, 74. [Google Scholar] [CrossRef] [PubMed]
- Clements, M.A.; Foster, N.C.; Maahs, D.M.; Schatz, D.A.; Olson, B.A.; Tsalikian, E.; Lee, J.M.; Burtsolorzano, C.; Tamborlane, W.V.; Chen, V.; et al. Hemoglobin A1c (HbA1c) changes over time among adolescent and young adult participants in the T1D Exchange Clinic Registry. Pediatr. Diabetes 2016, 17, 327–336. [Google Scholar] [CrossRef]
- Kelsey, M.M.; Zeitler, P.S. Insulin Resistance of Puberty. Curr. Diab. Rep. 2016, 16, 64. [Google Scholar] [CrossRef]
- Frohlich-Reiterer, E.E.; Rosenbauer, J.; Bechtold-Dalla Pozza, S.; Hofer, S.E.; Schober, E.; Holl, R.W. Predictors of increasing BMI during the course of diabetes in children and adolescents with type 1 diabetes: Data from the German/Austrian DPV multicentre survey. Arch. Dis. Child. 2014, 99, 738–743. [Google Scholar] [CrossRef]
- Giustina, A.; Berardelli, R.; Gazzaruso, C.; Mazziotti, G. Insulin and GH–IGF-I axis: Endocrine pacer or endocrine disruptor? Acta Diabetol. 2015, 52, 433–443. [Google Scholar] [CrossRef]
- Wolosowicz, M.; Lukaszuk, B.; Chabowski, A. The causes of insulin resistance in type 1 diabetes mellitus: Is there a place for quaternary prevention? Int. J. Environ. Res. Public Health 2020, 17, 8651. [Google Scholar] [CrossRef]
- Young, V.; Eiser, C.; Johnson, B.; Brierley, S.; Epton, T.; Elliott, J.; Heller, S. Eating problems in adolescents with type 1 diabetes: A systematic review with meta-analysis. Diabet. Med. 2013, 30, 189–198. [Google Scholar] [CrossRef]
- Mannucci, E.; Rotella, F.; Ricca, V.; Moretti, S.; Placidi, G.F.; Rotella, C.M. Eating disorders in patients with type 1 diabetes: A meta-analysis. J. Endocrinol. Investig. 2005, 28, 417–419. [Google Scholar] [CrossRef]
- Colton, P.A.; Olmsted, M.P.; Daneman, D.; Farquhar, J.C.; Wong, H.; Muskat, S.; Rodin, G.M. Eating disorders in girls and women with type 1 diabetes: A longitudinal study of prevalence, onset, remission, and recurrence. Diabetes Care 2015, 38, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Broadley, M.M.; Zaremba, N.; Andrew, B.; Ismail, K.; Treasure, J.; White, M.J.; Stadler, M. 25 years of psychological research investigating disordered eating in people with diabetes: What have we learnt? Diabet. Med. 2020, 37, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Winston, A.P. Eating disorders and diabetes. Curr. Diab. Rep. 2020, 20, 32. [Google Scholar] [CrossRef] [PubMed]
- Olmsted, M.P.; Colton, P.A.; Daneman, D.; Rydall, A.C.; Rodin, G.M. Prediction of the onset of disturbed eating behavior in adolescent girls with type 1 diabetes. Diabetes Care 2008, 31, 1978–1982. [Google Scholar] [CrossRef]
- Toni, G.; Berioli, M.; Cerquiglini, L.; Ceccarini, G.; Grohmann, U.; Principi, N.; Esposito, S. Eating disorders and disordered eating symptoms in adolescents with type 1 diabetes. Nutrients 2017, 9, 906. [Google Scholar] [CrossRef]
- Hevelke, L.K.; Albrecht, C.; Busse-Widmann, P.; Kranz, J.; Lange, K.; Markowitz, J.T.; Marshall, L.F.; Meurs, S.; de Soye, I.H.; Saßmann, H. Prävalenz gestörten Essverhaltens bei Typ 1 Diabetes im Kindes- und Jugendalter: Erfassungsmöglichkeiten und Vergleich mit gesunden Gleichaltrigen—Ergebnisse einer multizentrischen Fragebogenstudie. Psychother. Psychosom. Med. Psychol. 2016, 66, 128–135. [Google Scholar] [CrossRef]
- Peveler, R.C.; Bryden, K.S.; Neil, H.A.W.; Fairburn, C.G.; Mayou, R.A.; Dunger, D.B.; Turner, H.M. The relationship of disordered eating habits and attitudes to clinical outcomes in young adult females with type 1 diabetes. Diabetes Care 2005, 28, 84–88. [Google Scholar] [CrossRef]
- Ehrmann, D.; Kulzer, B.; Roos, T.; Haak, T.; Al-Khatib, M.; Hermanns, N. Risk factors and prevention strategies for diabetic ketoacidosis in people with established type 1 diabetes. Lancet Diabetes Endocrinol. 2020, 8, 436–446. [Google Scholar] [CrossRef]
- Markowitz, J.T.; Butler, D.A.; Volkening, L.K.; Antisdel, J.E.; Anderson, B.J.; Laffel, L.M.B. Brief screening tool for disordered eating in diabetes: Internal consistency and external validity in a contemporary sample of pediatric patients with type 1 diabetes. Diabetes Care 2010, 33, 495–500. [Google Scholar] [CrossRef]
- Apergi, K.; Romanidou, M.; Abdelkhalek, H.; Tripsianis, G.; Gonidakis, F. Reliability and validity of the Diabetes Eating Problem Survey in Greek adults with type 1 diabetes mellitus. Psychiatriki 2020, 31, 310–320. [Google Scholar] [CrossRef]
- Karastogiannidou, C.; Giannoulaki, P.; Samaras, I.; Kotzakioulafi, E.; Didangelos, T.; Bocsan, I.C.; Vassilopoulou, E. The Diabetes Eating Problem Survey-Revised (DEPS-R) in a Greek adult population with type 1 diabetes mellitus: Model comparison supporting a single factor structure. Nutrients 2021, 13, 2375. [Google Scholar] [CrossRef] [PubMed]
- Altınok, Y.A.; Özgür, S.; Meseri, R.; Özen, S.; Darcan, Ş.; Gökşen, D. Reliability and validity of the Diabetes Eating Problem Survey in Turkish children and adolescents with type 1 diabetes mellitus. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Saßmann, H.; Albrecht, C.; Busse-Widmann, P.; Hevelke, L.K.; Kranz, J.; Markowitz, J.T.; Marshall, L.F.; Meurs, S.; de Soye, I.H.; Lange, K. Psychometric properties of the German version of the Diabetes Eating Problem Survey-Revised: Additional benefit of disease-specific screening in adolescents with type 1 diabetes. Diabet. Med. 2015, 32, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Hummadi, A.; Yafei, S.; Badedi, M.; Abutaleb, R.; Darraj, H.; Alhagawy, A.J.; Khawaji, A.; Solan, Y.; Alzughbi, T.; Hakami, M.; et al. Validation of the Arabic version of Diabetes Eating Problem Survey–Revised (DEPS-R) among adolescents with type 1 diabetes. Nutrients 2023, 15, 561. [Google Scholar] [CrossRef]
- Ogden, C.L.; Kuczmarski, R.J.; Flegal, K.M.; Mei, Z.; Guo, S.; Wei, R.; Grummer-Strawn, L.M.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. Centers for Disease Control and Prevention 2000 growth charts for the United States: Improvements to the 1977 National Center for Health Statistics version. Pediatrics 2002, 109, 45–60. [Google Scholar] [CrossRef]
- Ruiz-Molina, Y.G.; Herrera-Ávila, J.; Espinosa-Juárez, J.V.; Esquinca-Avilés, H.A.; Tejas-Juárez, J.G.; Flores-Guillén, E.; Morales-Martínez, L.A.; Briones-Aranda, A.; Jiménez-Ceballos, B.; Sierra-Ramírez, J.A.; et al. Association of Overweight and Obesity with Impaired Executive Functioning in Mexican Adolescents: The Importance of Inhibitory Control. Healthcare 2024, 12, 1368. [Google Scholar] [CrossRef]

| Variable | Boys | CI 95% | Std Error | Girls | CI 95% | Std Error | p | Total | CI 95% | Std Error |
|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 13.77 ± 2.45 | 13.14–14.40 | 0.31 | 13.60 ± 2.54 | 12.93–14.26 | 0.33 | 0.704 | 13.69 ± 2.50 | 13.24–14.14 | 0.23 |
| Disease duration (years) | 5.00 ± 3.24 | 4.16–5.82 | 0.42 | 5.89 ± 3.77 | 4.91–6.88 | 0.49 | 0.277 | 5.43 ± 3.53 | 4.80–6.07 | 0.32 |
| Weight (kg) | 58.04 ± 18.13 | 53.40–62.69 | 2.32 | 56.72 ± 17.92 | 52.05–61.39 | 2.33 | 0.689 | 57.39 ± 17.96 | 54.15–60.64 | 1.64 |
| Weight Z-score | 0.62 ± 1.06 | 0.35–0.90 | 0.14 | 0.76 ± 0.97 | 0.51–1.01 | 0.13 | 0.469 | 0.69 ± 1.02 | 0.51–0.87 | 0.09 |
| Height (cm) | 164.00 ± 15.17 | 160.00–167.77 | 1.94 | 157.86 ± 11.43 | 154.88–160.84 | 1.49 | 0.016 | 160.92 ± 13.74 | 158.44–163.40 | 1.26 |
| Height Z-score | 0.59 ± 1.14 | 0.30–0.88 | 0.15 | 0.49 ± 1.13 | 0.20–0.79 | 0.15 | 0.642 | 0.54 ± 1.13 | 0.34–0.75 | 0.10 |
| BMI (kg/m2) | 21.12 ± 3.67 | 20.17–22.06 | 0.47 | 22.28 ± 4.95 | 21.00–23.57 | 0.64 | 0.144 | 21.69 ± 4.37 | 20.90–22.48 | 0.40 |
| BMI Z-score | 0.47 ± 0.89 | 0.24–0.70 | 0.11 | 0.68 ± 0.92 | 0.44–0.92 | 0.12 | 0.181 | 0.57 ± 0.91 | 0.41–0.74 | 0.08 |
| HbA1c (%) | 7.21 ± 1.19 | 6.91–7.52 | 0.15 | 7.41 ± 1.13 | 7.11–7.70 | 0.15 | 0.226 | 7.31 ± 1.16 | 7.10–7.52 | 0.11 |
| WHtI (cm) | 0.47 ± 0.06 | 0.45–0.48 | 0.01 | 0.48 ± 0.06 | 0.46–0.49 | 0.01 | 0.600 | 0.47 ± 0.06 | 0.46–0.48 | 0.01 |
| Sex | DEPS-R < 20 n (%) | DEPS-R ≥ 20 n (%) | Total n (%) | p-Value |
|---|---|---|---|---|
| Males | 49 (80.3%) | 12 (19.7%) | 61 (50.8%) | <0.001 |
| Females | 29 (49.2%) | 30 (50.8%) | 59 (49.2%) | |
| Total | 78 (65.0%) | 42 (35.0%) | 120 (100.0%) |
| Parameter | Correlation with Total Questionnaire Score |
|---|---|
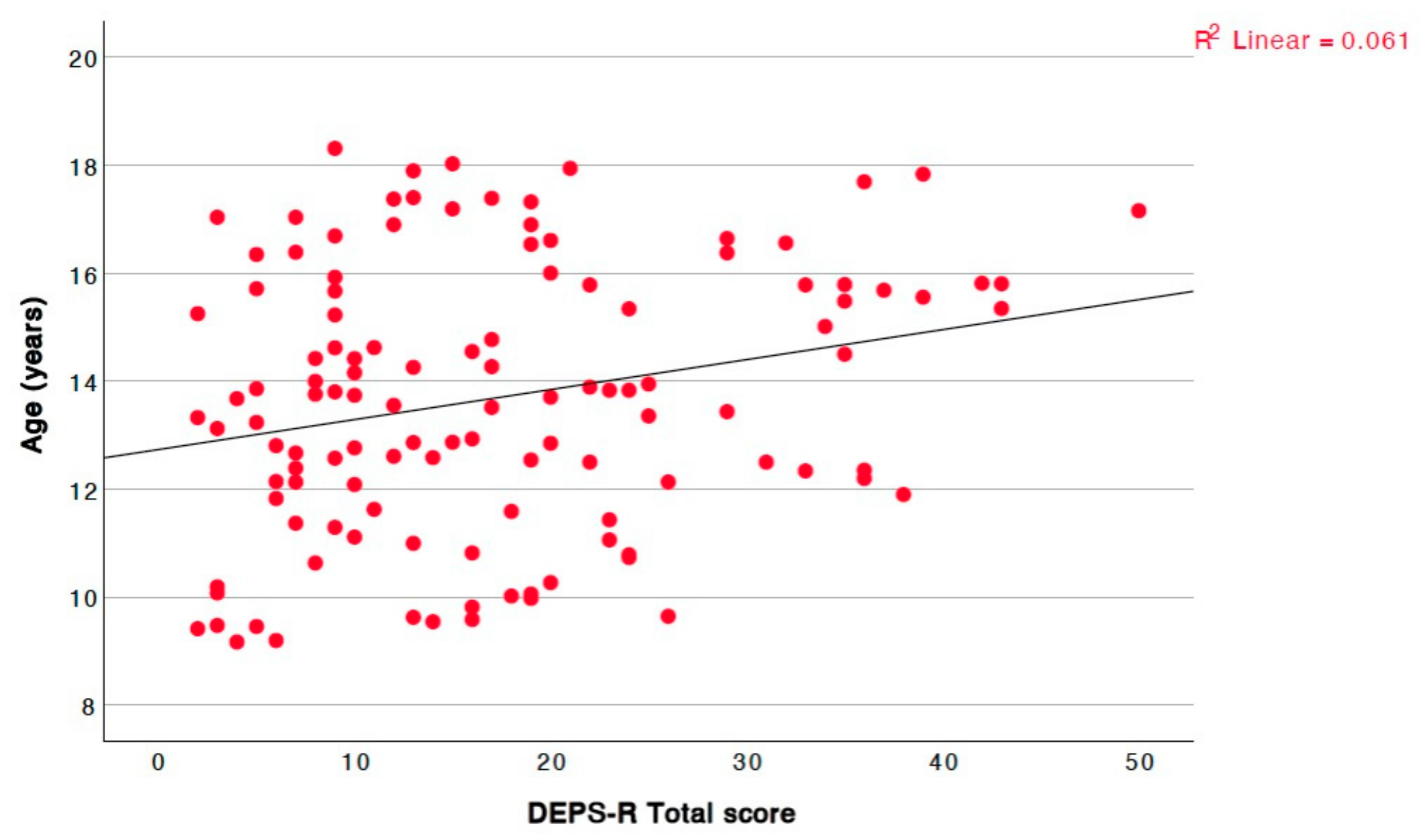
| Age | r = 0.212, p = 0.020, 95% CI = [0.03, 0.38] |
| Disease duration | r = 0.058, p = 0.531 |
| Weight | r = 0.319, p = <0.001, 95% CI = [0.15, 0.47] |
| Weight Z-score | r = 0.329, p = <0.001, 95% CI = [0.16, 0.48] |
| Height | r = 0.104, p = 0.260 |
| Height Z-score | r = −0.002, p = 0.979 |
| BMI | r = 0.419, p = <0.001, 95% CI = [0.26, 0.56] |
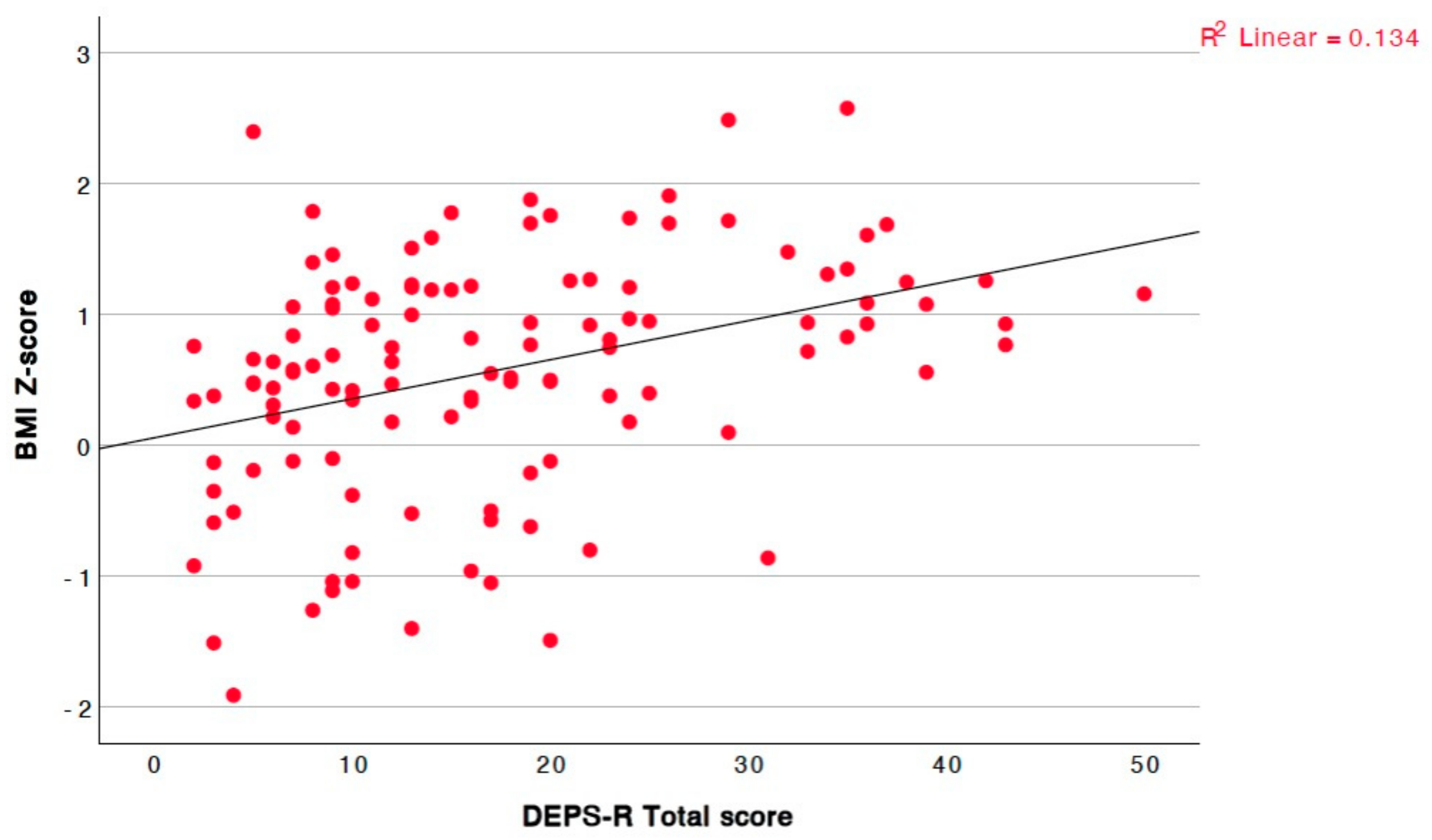
| BMI Z-score | r = 0.394, p = <0.001, 95% CI = [0.23, 0.54] |
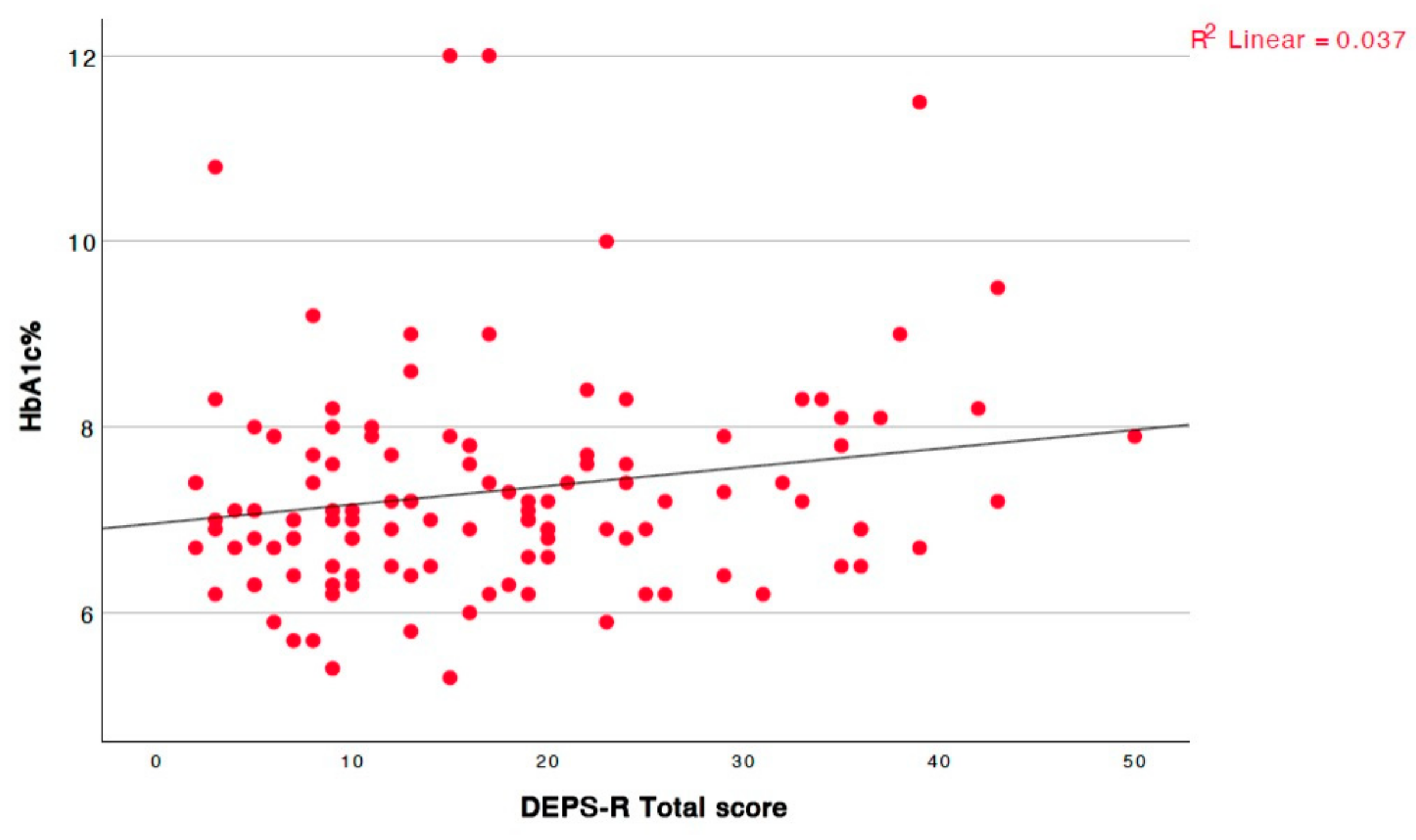
| HbA1c | r = 0.182, p = 0.047, 95% CI = [0.0, 0.35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oikonomou, A.; Christoforidis, A.; Kotanidou, E.P.; Giannopoulou, I.; Paschalidou, E.; Tsinopoulou, V.R.; Sotiriou, G.; Tsiroukidou, K.; Galli-Tsinopoulou, A. Detecting Disordered Eating Behaviors in Greek Youth with Type 1 Diabetes Mellitus by Using the Diabetes Eating Problem Survey—Revised (DEPS-R): Associations with Insulin Restriction, Glycemic Control, and Anthropometric Parameters. Children 2025, 12, 795. https://doi.org/10.3390/children12060795
Oikonomou A, Christoforidis A, Kotanidou EP, Giannopoulou I, Paschalidou E, Tsinopoulou VR, Sotiriou G, Tsiroukidou K, Galli-Tsinopoulou A. Detecting Disordered Eating Behaviors in Greek Youth with Type 1 Diabetes Mellitus by Using the Diabetes Eating Problem Survey—Revised (DEPS-R): Associations with Insulin Restriction, Glycemic Control, and Anthropometric Parameters. Children. 2025; 12(6):795. https://doi.org/10.3390/children12060795
Chicago/Turabian StyleOikonomou, Anastasia, Athanasios Christoforidis, Eleni P. Kotanidou, Ioanna Giannopoulou, Eleni Paschalidou, Vasiliki Rengina Tsinopoulou, Georgia Sotiriou, Kyriaki Tsiroukidou, and Assimina Galli-Tsinopoulou. 2025. "Detecting Disordered Eating Behaviors in Greek Youth with Type 1 Diabetes Mellitus by Using the Diabetes Eating Problem Survey—Revised (DEPS-R): Associations with Insulin Restriction, Glycemic Control, and Anthropometric Parameters" Children 12, no. 6: 795. https://doi.org/10.3390/children12060795
APA StyleOikonomou, A., Christoforidis, A., Kotanidou, E. P., Giannopoulou, I., Paschalidou, E., Tsinopoulou, V. R., Sotiriou, G., Tsiroukidou, K., & Galli-Tsinopoulou, A. (2025). Detecting Disordered Eating Behaviors in Greek Youth with Type 1 Diabetes Mellitus by Using the Diabetes Eating Problem Survey—Revised (DEPS-R): Associations with Insulin Restriction, Glycemic Control, and Anthropometric Parameters. Children, 12(6), 795. https://doi.org/10.3390/children12060795