Internalizing/Externalizing Problems and Sensory Processing Alteration in Children Referred to Child Mental Health Centers


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Achenbach, T.M.; Ivanova, M.Y.; Rescorla, L.A.; Turner, L.V.; Althoff, R.R. Internalizing/Externalizing Problems: Review and Recommendations for Clinical and Research Applications. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, A.; Nes, R.B.; Sanson, A.; Ystrom, E.; Karevold, E.B. Understanding trajectories of externalizing problems: Stability and emergence of risk factors from infancy to middle adolescence. Dev. Psychopathol. 2021, 33, 264–283. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Child Behavior Checklist for Ages 6-18. (Translation into Spanish by Unitat D’epidemiologia i de Diagnòstic Infantil, Facultat de Psicología. Universitat Autónoma de Barcelona); University of Vermont: Burlington, VT, USA, 2001. [Google Scholar]
- Forns, M.; Abad, J.; Kirchner, T. Internalizing and externalizing problems. In Encyclopedia of Adolescence; Levesque, R.J.R., Ed.; Springer: New York, NY, USA, 2011; pp. 1464–1469. Available online: http://link.springer.com/10.1007/978-1-4419-1695-2_261 (accessed on 22 April 2025).
- Vasileva, M.; Graf, R.K.; Reinelt, T.; Petermann, U.; Petermann, F. Research review: A meta-analysis of the international prevalence and comorbidity of mental disorders in children between 1 and 7 years. J. Child Psychol. Psychiatry 2021, 62, 372–381. [Google Scholar] [CrossRef]
- Oh, Y.; Greenberg, M.T.; Willoughby, M.T. Examining Longitudinal Associations between Externalizing and Internalizing Behavior Problems at Within- and Between-Child Levels. J. Abnorm. Child. Psychol. 2020, 48, 467–480. [Google Scholar] [CrossRef]
- Rapport, M.D.; Denney, C.B.; Chung, K.-M.; Hustace, K. Internalizing Behavior Problems and Scholastic Achievement in Children: Cognitive and Behavioral Pathways as Mediators of Outcome. J. Clin. Child Adolesc. Psychol. 2001, 30, 536–551. [Google Scholar] [CrossRef]
- Liu, J.; Chen, X.; Lewis, G. Childhood internalizing behaviour: Analysis and implications. Psychiatr. Ment. Health Nurs. 2011, 18, 884–894. [Google Scholar] [CrossRef]
- Gourley, L.; Wind, C.; Henninger, E.M.; Chinitz, S. Sensory Processing Difficulties, Behavioral Problems, and Parental Stress in a Clinical Population of Young Children. J. Child Fam. Stud. 2013, 22, 912–921. [Google Scholar] [CrossRef]
- Gouze, K.R.; Hopkins, J.; LeBailly, S.A.; Lavigne, J.V. Re-examining the Epidemiology of Sensory Regulation Dysfunction and Comorbid Psychopathology. J. Abnorm. Child Psychol. 2009, 37, 1077–1087. [Google Scholar] [CrossRef]
- Romero-Ayuso, D.; Ortiz-Rubio, A.; Vidal-Ramírez, C.; Pérez-Rodríguez, S.; Triviño-Juárez, J.M. Emotional Intelligence, Executive Functions and Sensory Processing in Daily Life in Children Aged Between 8 to 11 Years: A Pilot Study. Occup. Ther. Ment. Health 2023, 39, 137–155. [Google Scholar] [CrossRef]
- Dunn, W. Supporting Children to Participate Successfully in Everyday Life by Using Sensory Processing Knowledge. Infants Young Child. 2007, 20, 84–101. [Google Scholar] [CrossRef]
- Dunn, W. The Impact of Sensory Processing Abilities on the Daily Lives of Young Children and Their Families: A Conceptual Model. Infants Young Child. 1997, 9, 23–35. [Google Scholar] [CrossRef]
- Miller, L.; Nielsen, D.M.; Schoen, S.A.; Brett-green, B.A. Perspectives on sensory processing disorder: A call for translational research. Front. Integr. Neurosci. 2009, 3, 597. [Google Scholar] [CrossRef]
- Ahn, R.R.; Miller, L.J.; Milberger, S.; McIntosh, D.N. Prevalence of Parents’ Perceptions of Sensory Processing Disorders Among Kindergarten Children. Am. J. Occup. Ther. 2004, 58, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Galiana, A.; Flores-Ripoll, J.M.; Benito-Castellanos, P.J.; Villar-Rodriguez, C.; Vela-Romero, M. Prevalence and severity-based classification of sensory processing issues. An exploratory study with neuropsychological implications. Appl. Neuropsychol. Child 2022, 11, 850–862. [Google Scholar] [CrossRef]
- Ben-Sasson, A.; Soto, T.W.; Heberle, A.E.; Carter, A.S.; Briggs-Gowan, M.J. Early and Concurrent Features of ADHD and Sensory Over-Responsivity Symptom Clusters. J. Atten. Disord. 2017, 21, 835–845. [Google Scholar] [CrossRef]
- Galiana-Simal, A.; Vela-Romero, M.; Romero-Vela, V.M.; Oliver-Tercero, N.; García-Olmo, V.; Benito-Castellanos, P.J.; Muñoz-Martinez, V.; Beato-Fernandez, L. Sensory processing disorder: Key points of a frequent alteration in neurodevelopmental disorders. Cogent Med. 2020, 7, 1736829. [Google Scholar] [CrossRef]
- Harrison, L.A.; Kats, A.; Williams, M.E.; Aziz-Zadeh, L. The Importance of Sensory Processing in Mental Health: A Proposed Addition to the Research Domain Criteria (RDoC) and Suggestions for RDoC 2.0. Front. Psychol. 2019, 10, 103. [Google Scholar] [CrossRef]
- Serafini, G.; Gonda, X.; Canepa, G.; Pompili, M.; Rihmer, Z.; Amore, M.; Engel-Yeger, B. Extreme sensory processing patterns show a complex association with depression, and impulsivity, alexithymia, and hopelessness. J. Affect. Disord. 2017, 210, 249–257. [Google Scholar] [CrossRef]
- American Psyquiatric Association. Manual Diagnóstico y Estadístico de Los Trastornos Mentales; (5a ed.-TR.); Editorial Médica Panamericana: Madrid, Spain, 2022. [Google Scholar]
- Dellapiazza, F.; Michelon, C.; Vernhet, C.; Muratori, F.; Blanc, N.; Picot, M.-C.; Baghdadli, A. Sensory processing related to attention in children with ASD, ADHD, or typical development: Results from the ELENA cohort. Eur. Child Adolesc. Psychiatry 2021, 30, 283–291. [Google Scholar] [CrossRef]
- Critz, C.; Blake, K.; Nogueira, E. Sensory Processing Challenges in Children. J. Nurse Pract. 2015, 11, 710–716. [Google Scholar] [CrossRef]
- Lane, S.J.; Reynolds, S.; Dumenci, L. Sensory Overresponsivity and Anxiety in Typically Developing Children and Children With Autism and Attention Deficit Hyperactivity Disorder: Cause or Coexistence? Am. J. Occup. Ther. 2012, 66, 595–603. [Google Scholar] [CrossRef]
- Boterberg, S.; Warreyn, P. Making sense of it all: The impact of sensory processing sensitivity on daily functioning of children. Pers. Individ. Differ. 2016, 92, 80–86. [Google Scholar] [CrossRef]
- Dean, E.E.; Little, L.; Tomchek, S.; Dunn, W. Sensory Processing in the General Population: Adaptability, Resiliency, and Challenging Behavior. Am. J. Occup. Ther. 2018, 72, 7201195060p1–7201195060p8. [Google Scholar] [CrossRef]
- Diamant, R. Relationships Among Sensory Processing Behaviors, Executive Function, and Temperament Characteristics for Effortful Control in School-Age Children. Am. J. Occup. Ther. 2022, 76, 7610505101p1. [Google Scholar] [CrossRef]
- Dunn, W. Perfil Sensorial—2: Manual; Pearson Educación: Madrid, Spain, 2016. [Google Scholar]
- Achenbach, T.M. The ASEBA Manual for Assessing Progress & Outcomes of Problems & Strengths; An Integrated System of Multi-informant Assessment; ASEBA: Burlington, VT, USA, 2020. [Google Scholar]
- Sardinero, E.; Pedreira, J.L.; Muñiz, J. El cuestionario CBCL de Achenbach: Adaptación española y aplicaciones clínico-epidemiológicas. Clín. Y Salud 1997, 8, 447–480. [Google Scholar]
- Romero-Ayuso, D.; Labrador, C.; Pérez, C. Perfil Sensorial 2 de Winnie Dunn; Pearson: Madrid, Spain, 2016. [Google Scholar] [CrossRef]
- Mulligan, S.; Douglas, S.; Armstrong, C. Characteristics of Idiopathic Sensory Processing Disorder in Young Children. Front. Integr. Neurosci. 2021, 15, 647928. [Google Scholar] [CrossRef]
- Pfeiffer, B.; Daly, B.P.; Nicholls, E.G.; Gullo, D.F. Assessing Sensory Processing Problems in Children With and Without Attention Deficit Hyperactivity Disorder. Phys. Occup. Ther. Pediatr. 2015, 35, 1–12. [Google Scholar] [CrossRef]
- McMahon, K.; Anand, D.; Morris-Jones, M.; Rosenthal, M.Z. A Path From Childhood Sensory Processing Disorder to Anxiety Disorders: The Mediating Role of Emotion Dysregulation and Adult Sensory Processing Disorder Symptoms. Front. Integr. Neurosci. 2019, 13, 22. [Google Scholar] [CrossRef]
- Delgado-Lobete, L.; Pértega-Díaz, S.; Santos-del-Riego, S.; Montes-Montes, R. Sensory processing patterns in developmental coordination disorder, attention deficit hyperactivity disorder and typical development. Res. Dev. Disabil. 2020, 100, 103608. [Google Scholar] [CrossRef]
- Anquetil, M.; Roche-Labarbe, N.; Rossi, S. Tactile sensory processing as a precursor of executive attention: Toward early detection of attention impairments and neurodevelopmental disorders. Wiley Interdiscip. Rev. Cogn. Sci. 2023, 14, e1640. [Google Scholar] [CrossRef]
- Nesayan, A.; Asadi Gandomani, R.; Movallali, G.; Dunn, W. The relationship between sensory processing patterns and behavioral patterns in children. J. Occup. Ther. Sch. Early Interv. 2018, 11, 124–132. [Google Scholar] [CrossRef]
- Williams, K.L.; Kirby, A.V.; Watson, L.R.; Sideris, J.; Bulluck, J.; Baranek, G.T. Sensory features as predictors of adaptive behaviors: A comparative longitudinal study of children with autism spectrum disorder and other developmental disabilities. Res. Dev. Disabil. 2018, 81, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W.; Little, L.; Dean, E.; Robertson, S.; Evans, B. The State of the Science on Sensory Factors and Their Impact on Daily Life for Children: A Scoping Review. OTJR Occup. Ther. J. Res. 2016, 36, 3S–26S. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Petroski, G.F. Sleep problems in children with autism spectrum disorder: Examining the contributions of sensory over-responsivity and anxiety. Sleep Med. 2015, 16, 270–279. [Google Scholar] [CrossRef]
- Blanken, L.M.E.; White, T.; Mous, S.E.; Basten, M.; Muetzel, R.L.; Jaddoe, V.W.V.; Wals, M.; Van Der Ende, J.; Verhulst, F.C.; Tiemeier, H. Cognitive functioning in children with internalising, externalising and dysregulation problems: A population-based study. Eur. Child Adolesc. Psychiatry 2017, 26, 445–456. [Google Scholar] [CrossRef]
- Zero to Three. DC: 0-5: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood; Zero to Three: Washington, DC, USA, 2016; p. 212. [Google Scholar]
- Dunn, W.; Cox, J.; Foster, L.; Mische-Lawson, L.; Tanquary, J. Impact of a Contextual Intervention on Child Participation and Parent Competence Among Children With Autism Spectrum Disorders: A Pretest–Posttest Repeated-Measures Design. Am. J. Occup. Ther. 2012, 66, 520–528. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | ||||
|---|---|---|---|---|
| CBCL | Total (n = 63) M (SD) | Male (n = 43) M (SD) | Female (n = 20) M (SD) | t (p) |
| Syndrome Scale | ||||
| Anxious/Depressed | 64.73 (10.27) | 63.44 (10.10) | 67.50 (10.41) | −1.47 (0.15) |
| Withdrawn/Depressed | 61.03 (9.54) | 60.42 (9.73) | 62.35 (9.20) | −0.75 (0.46) |
| Somatic Complaints | 60.35 (8.12) | 60.02 (8.44) | 61.05 (7.55) | −0.46 (0.64) |
| Rule-Breaking Behavior | 58.30 (7.00) | 57.95 (7.50) | 59.05 (5.86) | −0.58 (0.57) |
| Aggressive Behavior | 63.05 (9.04) | 63.42 (9.54) | 62.25 (8.01) | 0.48 (0.64) |
| Attention Problems | 66.49 (11.17) | 65.67 (11.54) | 68.25 (10.36) | −0.85 (0.39) |
| Social Problems | 62.24 (7.72) | 61.40 (6.43) | 64.05 (9.89) | −1.28 (0.21) |
| Thought Problems | 61.89 (8.80) | 61.33 (8.91) | 63.10 (8.65) | −0.74 (0.46) |
| Composite and Total Scales | ||||
| Internalizing Problems | 63.90 (9.11) | 62.72 (8.95) | 66.45 (9.12) | −1.53 (0.13) |
| Externalizing Problems | 60.63 (9.95) | 60.40 (10.73) | 61.15 (8.22) | −0.28 (0.78) |
| Total Problems | 63.87 (9.04) | 63.98 (9.22) | 63.65 (16.04) | 0.10 (0.92) |
| Level of Sensory Processing Alteration | ||||||
|---|---|---|---|---|---|---|
| A. No Alteration (n = 27) | B. Mild (n = 11) | C. Moderate (n = 6) | D. Severe (n = 19) | |||
| CBCL | M (SD) | M (SD) | M (SD) | M (SD) | F(3, 59) | Post hoc/d |
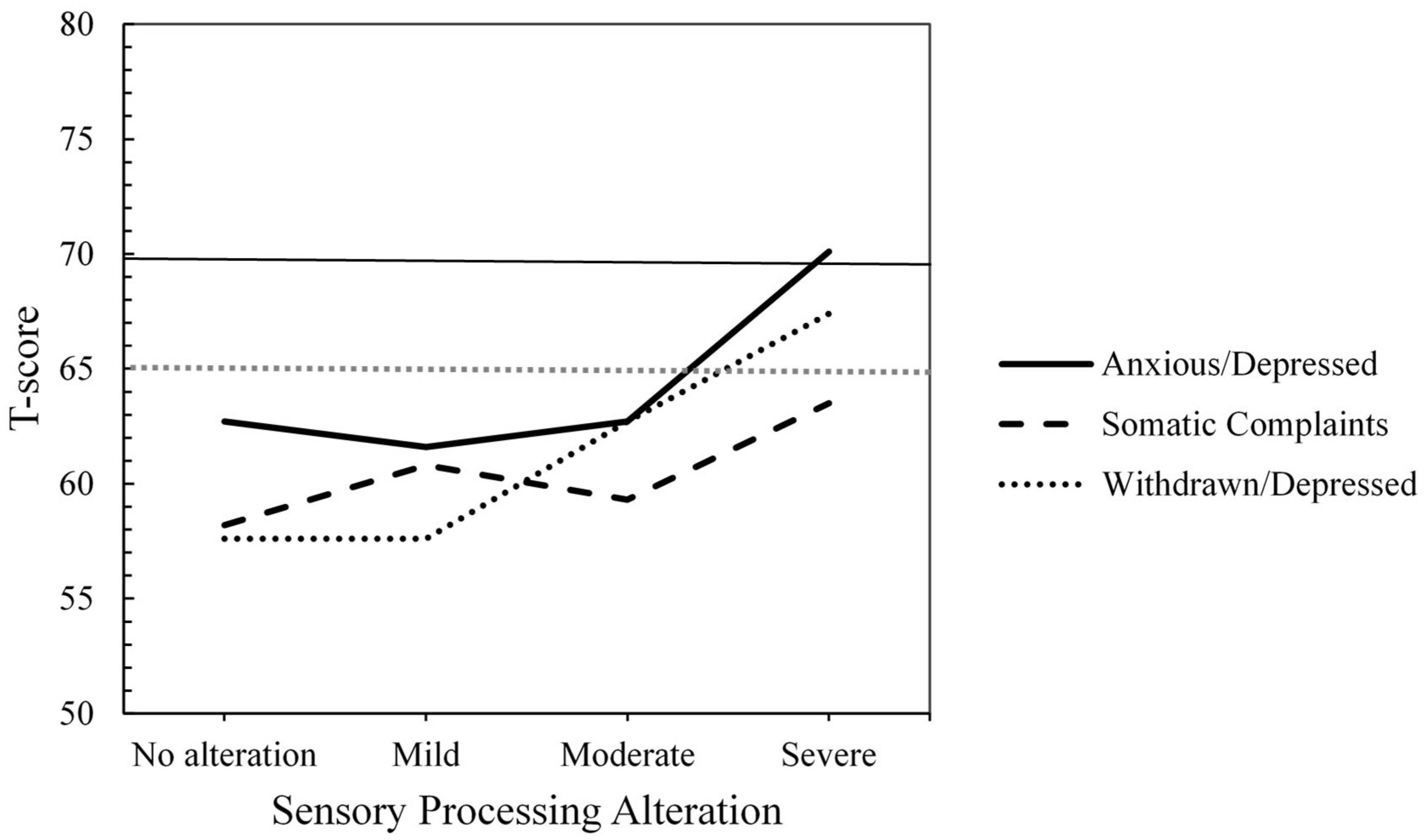
| Anxious/Depressed | 62.74 (9.61) | 61.55 (10.95) | 62.67 (7.31) | 70.05 (10.34) | 2.66 | |
| Withdrawn/Depressed | 57.59 (8.20) | 57.64 (6.25) | 62.67 (13.62) | 67.37 (8.66) | 5.46 ** | A < D */−1.15 |
| Somatic Complaints | 58.15 (6.40) | 60.82 (6.42) | 59.33 (5.72) | 63.53 (10.86) | 1.73 | |
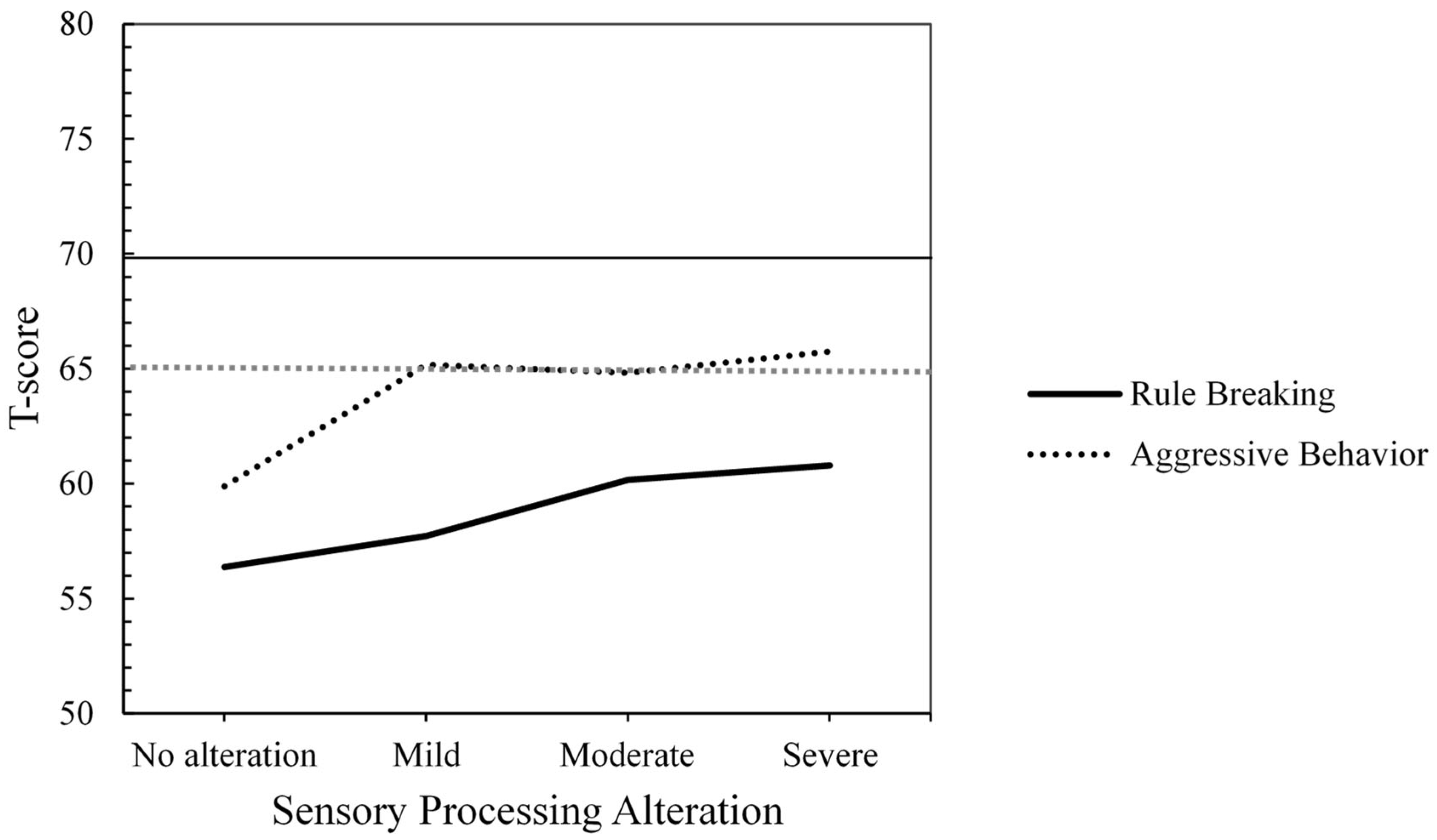
| Rule-Breaking Behavior | 56.37 (7.08) | 57.73 (5.68) | 60.17 (8.50) | 60.79 (6.70) | 1.71 | |
| Aggressive Behavior | 59.89 (8.75) | 65.18 (11.34) | 64.83 (5.19) | 65.74 (8.08) | 2.04 | |
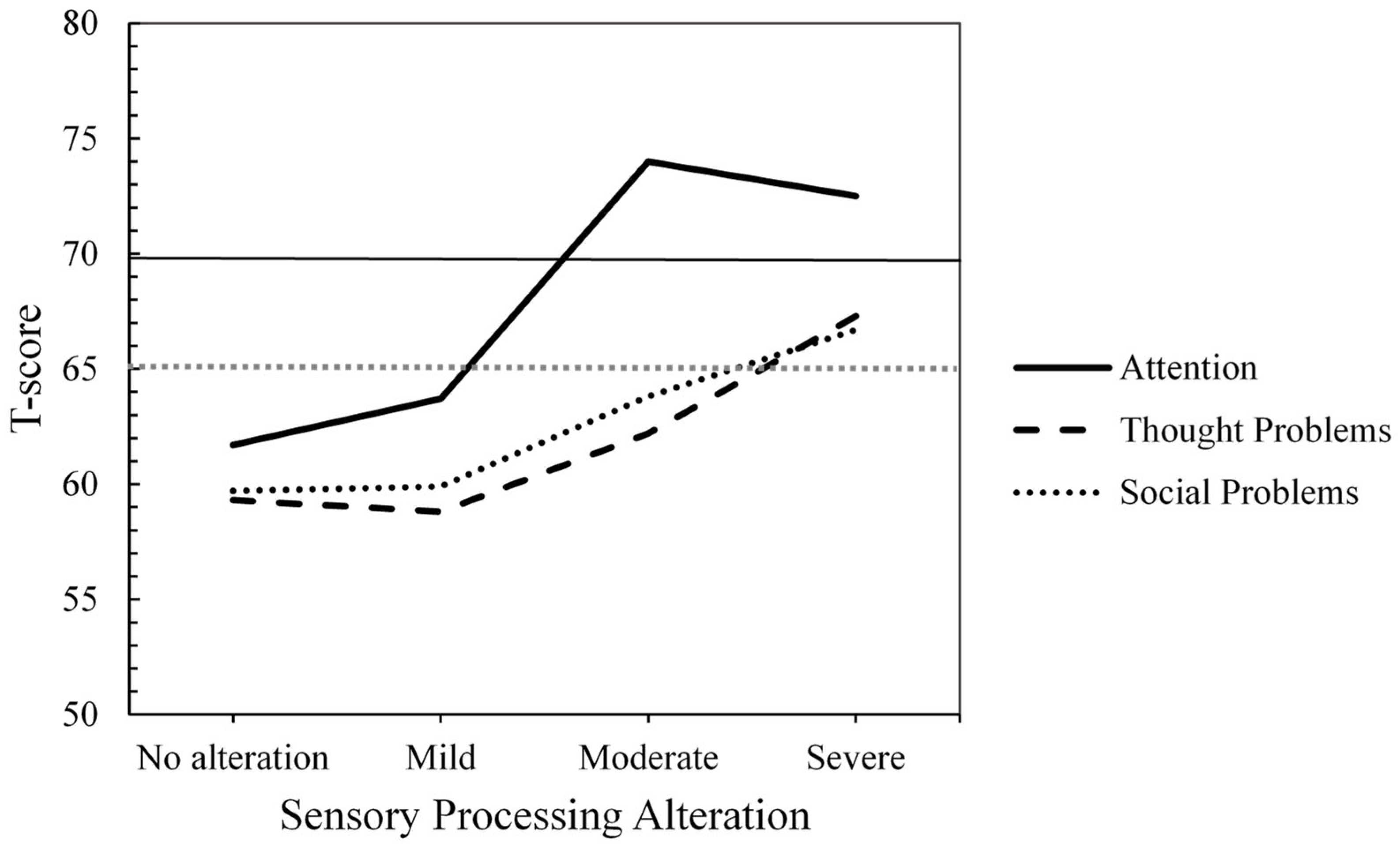
| Attention Problems | 61.70 (9.18) | 63.73 (8.49) | 74.00 (12.70) | 72.53 (11.25) | 5.68 ** | A < D */−1.05 |
| Social Problems | 59.67 (5.11) | 59.91 (10.22) | 63.83 (7.00) | 66.74 (7.78) | 4.10 | |
| Thought Problems | 59.26 (7.40) | 58.82 (9.08) | 62.17 (7.78) | 67.32 (8.83) | 4.23 | |
| Level of Sensory Processing Alteration | ||||||
|---|---|---|---|---|---|---|
| A. No Alteration (n = 27) | B. Mild (n = 11) | C. Moderate (n = 6) | D. Severe (n = 19) | |||
| CBCL | M (SD) | M (SD) | M (SD) | M (SD) | F(3, 59) | Post Hoc/d |
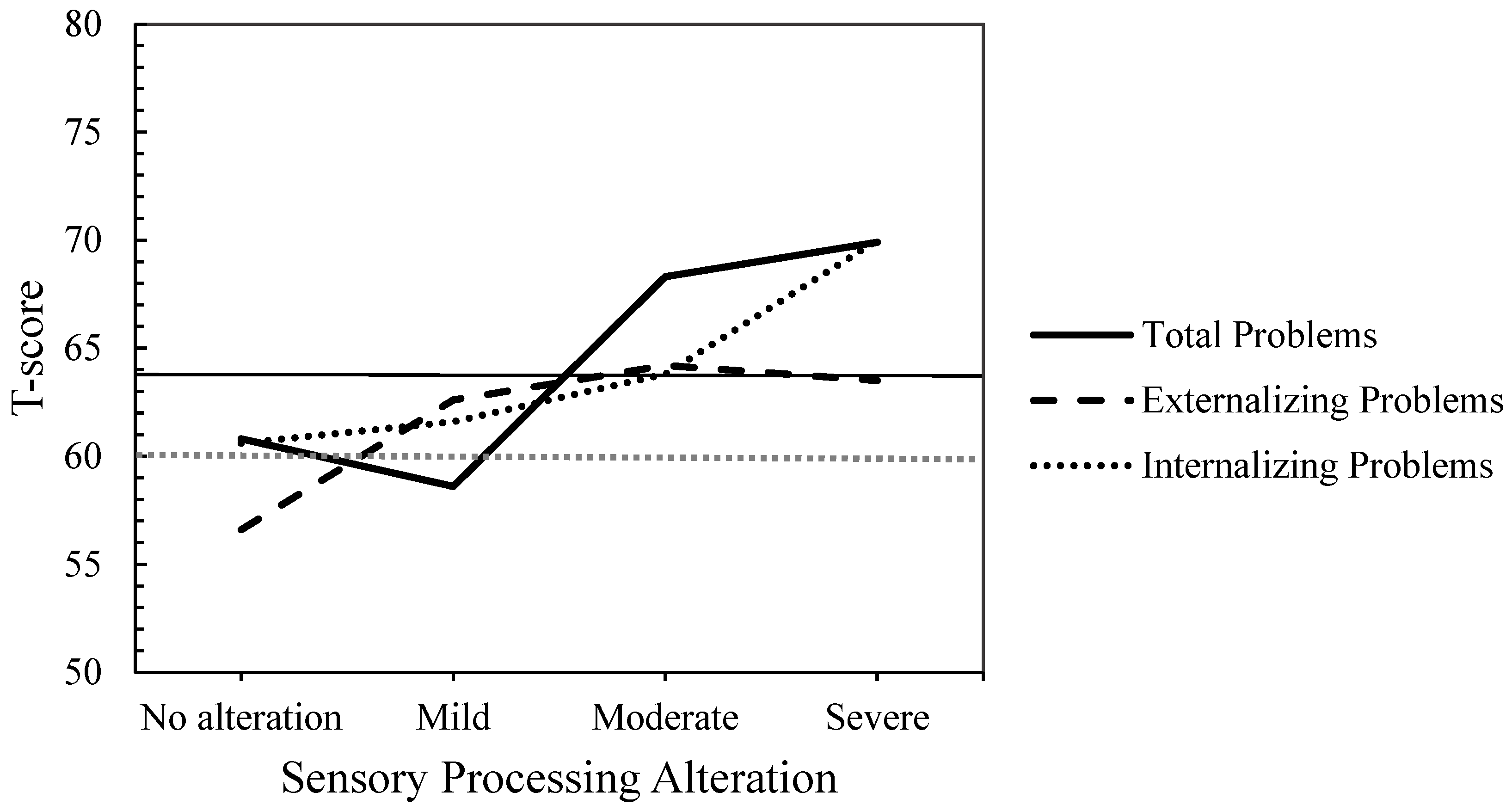
| Internalizing Problems | 60.56 (8.21) | 61.64 (9.21) | 63.83 (7.22) | 70.00 (8.23) | 5.14 * | A < D **/−1.14 |
| Externalizing Problems | 56.59 (10.96) | 62.64 (9.22) | 64.17 (6.80) | 64.11 (7.96) | 2.90 | |
| Total Problems | 60.78 (8.84) | 58.64 (20.94) | 68.33 (4.76) | 69.89 (5.59) | 3.79 * | A < D +/−1.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valencia, M.; D’Ocon, A.; Plata, R.; Simó, S.; Cantero, M.J. Internalizing/Externalizing Problems and Sensory Processing Alteration in Children Referred to Child Mental Health Centers. Children 2025, 12, 664. https://doi.org/10.3390/children12060664
Valencia M, D’Ocon A, Plata R, Simó S, Cantero MJ. Internalizing/Externalizing Problems and Sensory Processing Alteration in Children Referred to Child Mental Health Centers. Children. 2025; 12(6):664. https://doi.org/10.3390/children12060664
Chicago/Turabian StyleValencia, Macarena, Ana D’Ocon, Raquel Plata, Sandra Simó, and María José Cantero. 2025. "Internalizing/Externalizing Problems and Sensory Processing Alteration in Children Referred to Child Mental Health Centers" Children 12, no. 6: 664. https://doi.org/10.3390/children12060664
APA StyleValencia, M., D’Ocon, A., Plata, R., Simó, S., & Cantero, M. J. (2025). Internalizing/Externalizing Problems and Sensory Processing Alteration in Children Referred to Child Mental Health Centers. Children, 12(6), 664. https://doi.org/10.3390/children12060664