


Resiliency in Child–Caregiver Dyads and the Impact on Health Outcomes in Sickle Cell Disease


Abstract
1. Introduction
2. Materials and Methods
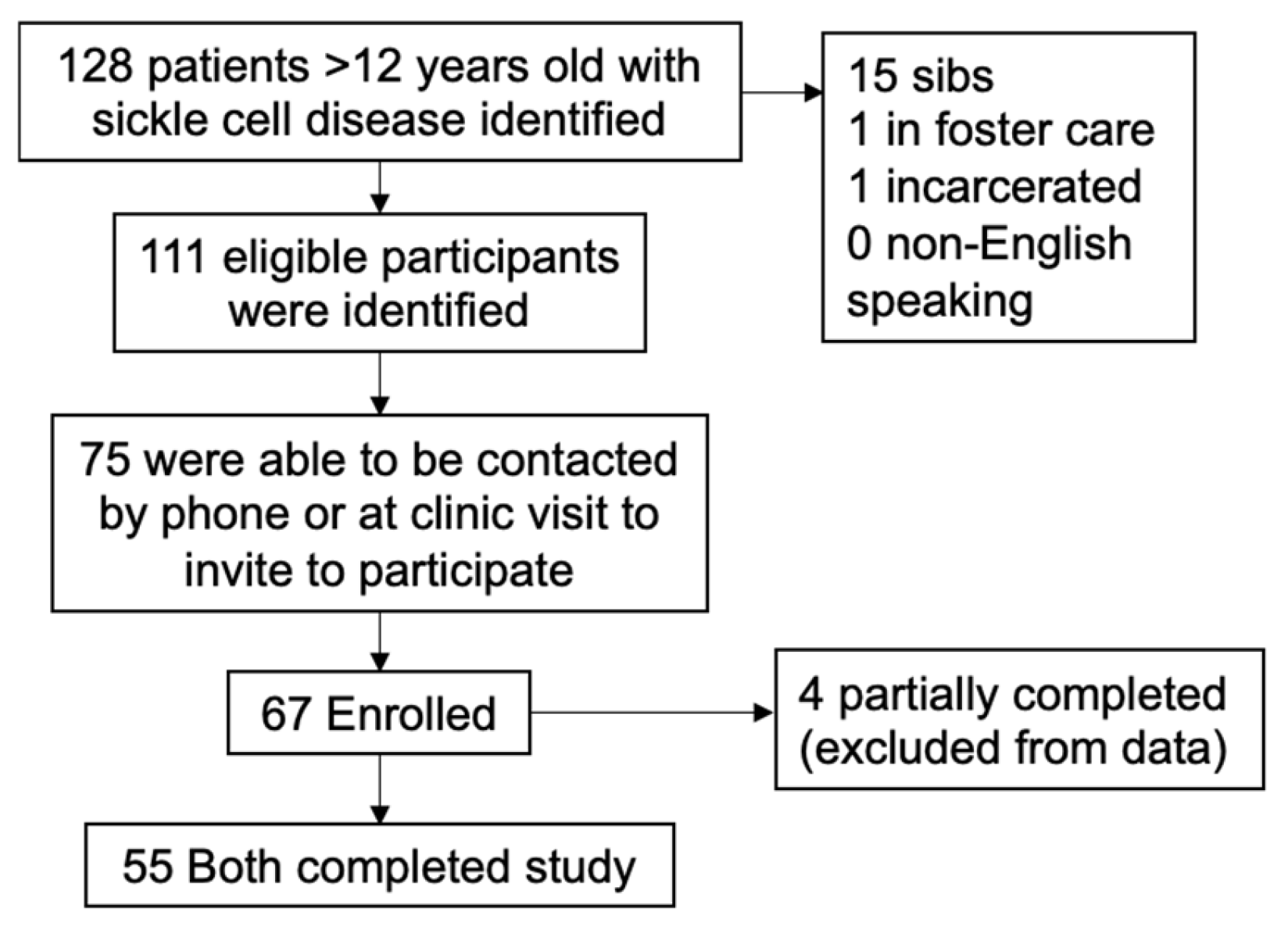
2.1. Participants
2.2. Study Participation
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Distribution of Resiliency and Stress Scores
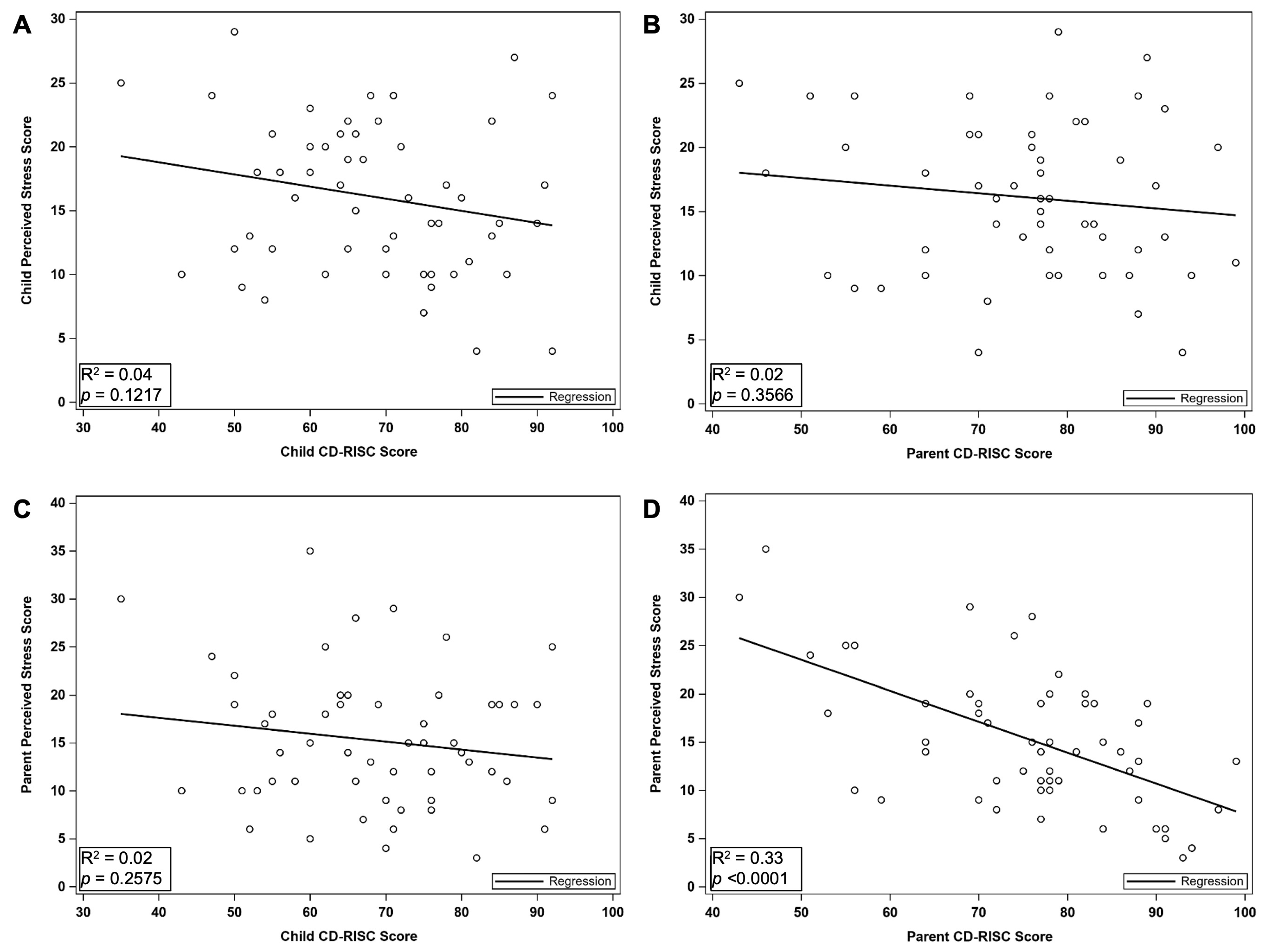
3.2. Associations Between Stress and Resiliency
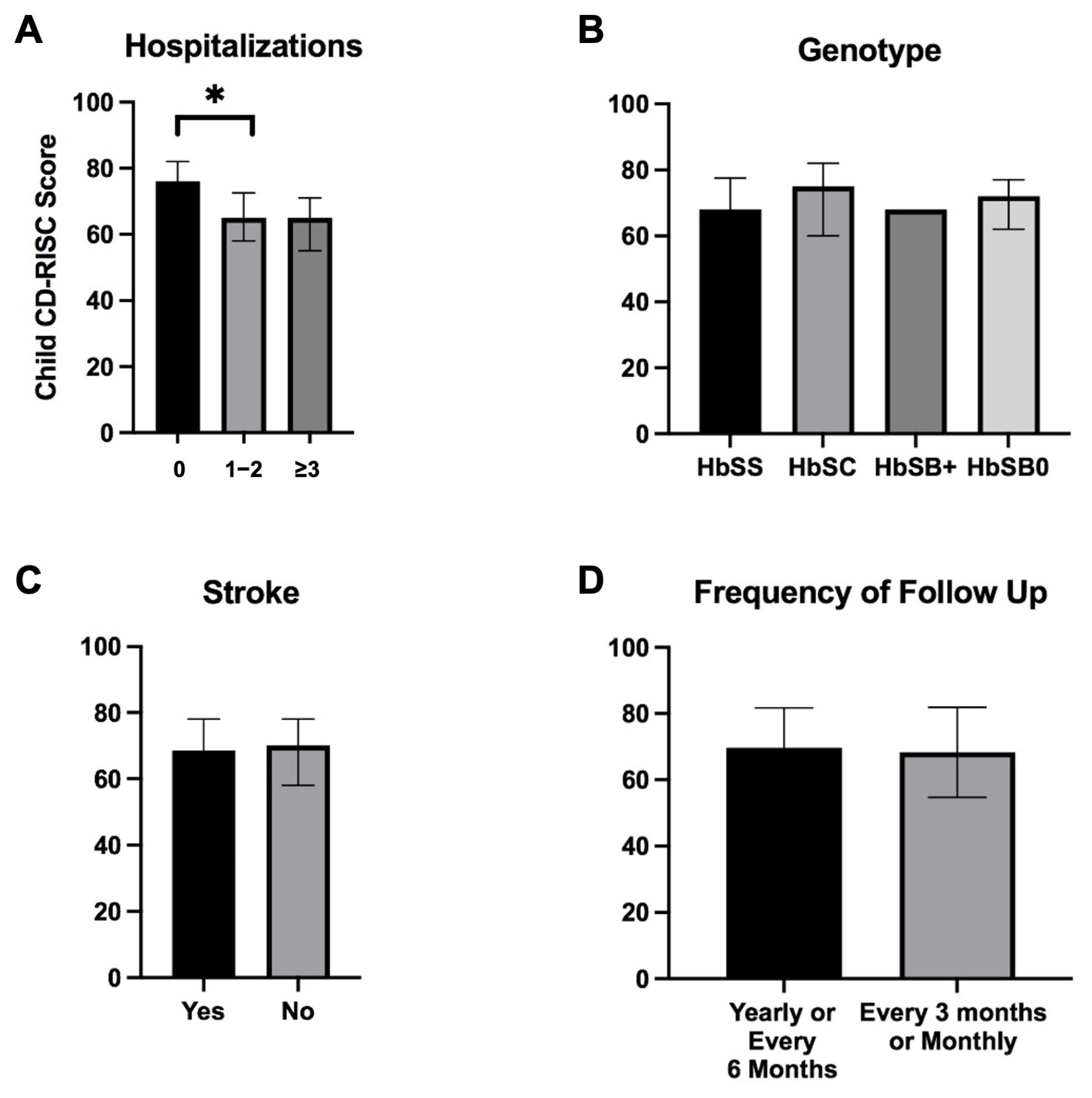
3.3. Lower Resiliency Scores Are Associated with Increased Hospitalizations, but Not with Other Markers of Severe Clinical Disease
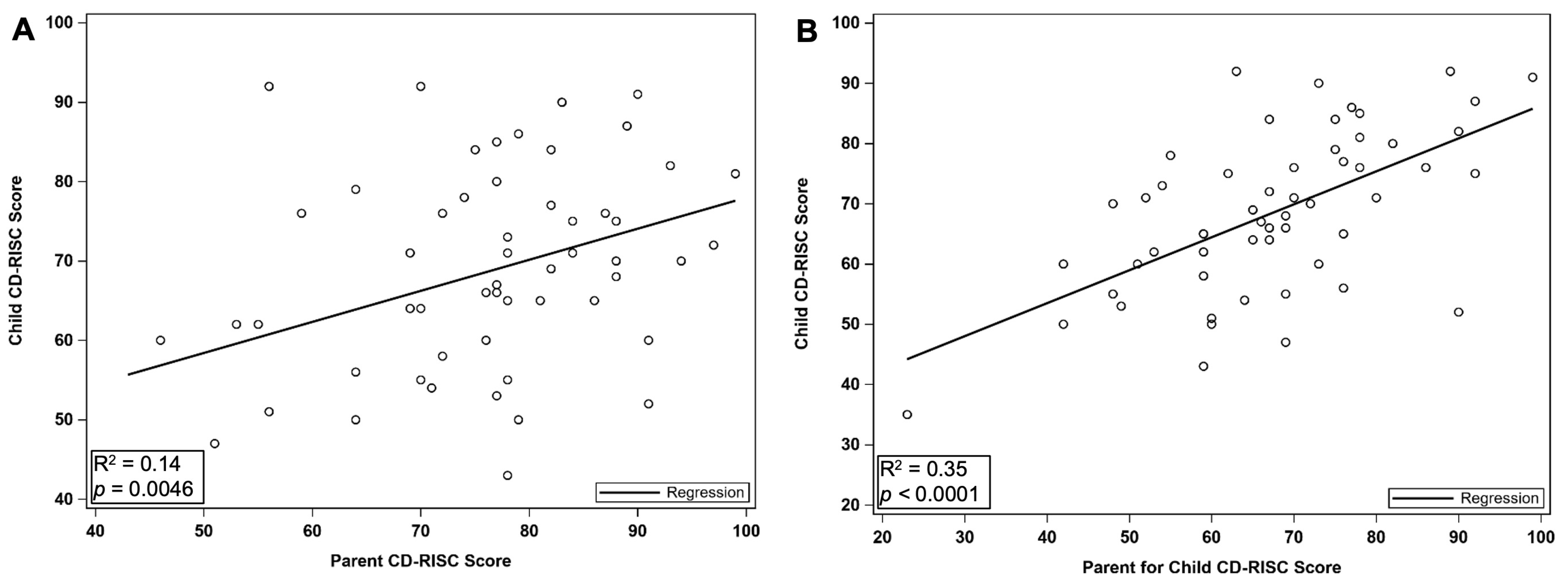
3.4. Child Resiliency Correlates with Caregiver Resiliency Scores and Can Be Accurately Assessed by Caregiver
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE | Adverse childhood experiences |
| SCD | Sickle cell disease |
| ER | Emergency room |
| PSS-10 | Perceived stress scale |
| CD-RISC | Connor Davidson-Resiliency Scale |
| PROMIS | Patient-Reported Outcome Measurement Information System |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Child Stressors | N (%) | Caregiver Stressors | N (%) |
|---|---|---|---|
| Financial difficulties | Financial difficulties | ||
| Never | 28 (50.91%) | Never | 4 (7.27%) |
| Almost Never | 11 (20%) | Almost Never | 9 (16.36%) |
| Sometimes | 12 (21.82%) | Sometimes | 26 (47.27%) |
| Fairly Often | 2 (3.64%) | Fairly Often | 9 (16.36%) |
| Very Often | 2 (3.64%) | Very Often | 7 (12.73%) |
| Difficulty with parent | Difficulty with child | ||
| Never | 31 (56.36%) | Never | 19 (34.55%) |
| Almost Never | 11 (20%) | Almost Never | 15 (27.27%) |
| Sometimes | 10 (18.18%) | Sometimes | 17 (30.91%) |
| Fairly Often | 0 (0%) | Fairly Often | 2 (3.64%) |
| Very Often | 3 (5.45%) | Very Often | 2 (3.64%) |
| Difficulty between my children | |||
| Never | 24 (43.64%) | ||
| Almost Never | 13 (23.64%) | ||
| Sometimes | 14 (25.45%) | ||
| Fairly Often | 3 (5.45%) | ||
| Very Often | 1 (1.82%) | ||
| Difficulty with my extended family a | Difficulty with my extended family | ||
| Never | 14 (25.45%) | Never | 19 (34.55%) |
| Almost Never | 11 (20.37%) | Almost Never | 20 (36.36%) |
| Sometimes | 8 (14.81%) | Sometimes | 10 (18.18%) |
| Fairly Often | 1 (1.85%) | Fairly Often | 5 (9.09%) |
| Very Often | 1 (1.85%) | Very Often | 1 (1.82%) |
| Difficulty with my school work | Difficulty with work or school work | ||
| Never | 28 (50.91%) | Never | 28 (50.91%) |
| Almost Never | 15 (27.27%) | Almost Never | 13 (23.64%) |
| Sometimes | 18 (32.73%) | Sometimes | 12 (2%) |
| Fairly Often | 5 (9.09%) | Fairly Often | 2 (3.64%) |
| Very Often | 3 (5.45%) | Very Often | 0 (0%) |
| Concern for my physical safety | Concern for my physical safety of myself or my Children | ||
| Never | 36 (65.45%) | Never | 29 (52.73%) |
| Almost Never | 10 (18.18%) | Almost Never | 11 (20%) |
| Sometimes | 9 (16.36%) | Sometimes | 10 (18.18%) |
| Fairly Often | 0 (0%) | Fairly Often | 5 (9.09%) |
| Very Often | 0 (0%) | Very Often | 0 (0%) |
| Concern about getting sick from COVID-19 | Concern about getting sick from COVID-19 | ||
| Never | 13 (23.64%) | Never | 4 (7.27%) |
| Almost Never | 8 (14.55%) | Almost Never | 7 (12.73%) |
| Sometimes | 20 (36.36%) | Sometimes | 18 (32.73%) |
| Fairly Often | 7 (12.73%) | Fairly Often | 9 (16.36%) |
| Very Often | 7 (12.73%) | Very Often | 17 (30.91%) |
| Concern about getting others sick | Concern about getting others sick | ||
| Never | 27 (49.09%) | Never | 15 (27.27%) |
| Almost Never | 10 (18.18%) | Almost Never | 9 (16.36%) |
| Sometimes | 13 (23.64%) | Sometimes | 12 (21.82%) |
| Fairly Often | 2 (3.64%) | Fairly Often | 11 (20%) |
| Very Often | 3 (5.45%) | Very Often | 8 (14.55%) |
| Concern about caring for someone who is sick | |||
| Never | 15 (27.27%) | ||
| Almost Never | 12 (21.82%) | ||
| Sometimes | 15 (27.27%) | ||
| Fairly Often | 7 (12.73%) | ||
| Very Often | 6 (10.91%) | ||
| Concern about other health issues | Concern about other health issues | ||
| Never | 17 (30.91%) | Never | 10 (18.18%) |
| Almost Never | 11 (20%) | Almost Never | 10 (18.18%) |
| Sometimes | 15 (27.27%) | Sometimes | 25 (45.45%) |
| Fairly Often | 7 (12.73%) | Fairly Often | 4 (7.27%) |
| Very Often | 5 (9.09%) | Very Often | 6 (10.91%) |
| Concern about sickle cell disease | Concern about my child’s sickle cell disease | ||
| Never | 13 (23.64%) | Never | 2 (3.64%) |
| Almost Never | 7 (12.73%) | Almost Never | 8 (14.55%) |
| Sometimes | 18 (32.73%) | Sometimes | 15 (27.27%) |
| Fairly Often | 10 (18.18%) | Fairly Often | 15 (27.27%) |
| Very Often | 7 (12.73%) | Very Often | 15 (27.27%) |
References
- Gartland, D.; Riggs, E.; Muyeen, S.; Giallo, R.; Afifi, T.O.; MacMillan, H.; Herrman, H.; Bulford, E.; Brown, S.J. What factors are associated with resilient outcomes in children exposed to social adversity? A systematic review. BMJ Open 2019, 9, e024870. [Google Scholar] [CrossRef]
- Bucci, M.; Marques, S.S.; Oh, D.; Harris, N.B. Toxic Stress in Children and Adolescents. Adv. Pediatr. 2016, 63, 403–428. [Google Scholar] [CrossRef] [PubMed]
- Bethell, C.D.; Newacheck, P.; Hawes, E.; Halfon, N. Adverse childhood experiences: Assessing the impact on health and school engagement and the mitigating role of resilience. Health Aff. 2014, 33, 2106–2115. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, L.K.; Breiding, M.J.; Merrick, M.T.; Thompson, W.W.; Ford, D.C.; Dhingra, S.S.; Parks, S.E. Childhood adversity and adult chronic disease: An update from ten states and the District of Columbia, 2010. Am. J. Prev. Med. 2015, 48, 345–349. [Google Scholar] [CrossRef]
- Merrick, M.T.; Ports, K.A.; Ford, D.C.; Afifi, T.O.; Gershoff, E.T.; Grogan-Kaylor, A. Unpacking the impact of adverse childhood experiences on adult mental health. Child Abus. Negl. 2017, 69, 10–19. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Exley, D.; Norman, A.; Hyland, M. Adverse childhood experience and asthma onset: A systematic review. Eur. Respir. Rev. 2015, 24, 299–305. [Google Scholar] [CrossRef]
- Hackworth, N.J.; Matthews, J.; Burke, K.; Petrovic, Z.; Klein, B.; Northam, E.A.; Kyrios, M.; Chiechomski, L.; Cameron, F.J. Improving mental health of adolescents with Type 1 diabetes: Protocol for a randomized controlled trial of the Nothing Ventured Nothing Gained online adolescent and parenting support intervention. BMC Public Health 2013, 13, 1185. [Google Scholar] [CrossRef]
- Vesco, A.T.; Feldman, M.A.; Evans, M.A.; Weissberg-Benchell, J. Parent-adolescent dyadic diabetes distress: Associations with A1c and diabetes-related strengths. Fam. Syst. Health 2018, 36, 357–367. [Google Scholar] [CrossRef]
- Lubeck, D.; Agodoa, I.; Bhakta, N.; Danese, M.; Pappu, K.; Howard, R.; Gleeson, M.; Halperin, M.; Lanzkron, S. Estimated Life Expectancy and Income of Patients with Sickle Cell Disease Compared with Those Without Sickle Cell Disease. JAMA Netw. Open 2019, 2, e1915374. [Google Scholar] [CrossRef]
- King, A.A.; Rodeghier, M.J.; Panepinto, J.A.; Strouse, J.J.; Casella, J.F.; Quinn, C.T.; Dowling, M.M.; Sarnaik, S.A.; Thompson, A.A.; Woods, G.M.; et al. Silent cerebral infarction, income, and grade retention among students with sickle cell anemia. Am. J. Hematol. 2014, 89, E188–E192. [Google Scholar] [CrossRef] [PubMed]
- Pernell, B.; Nagalapuram, V.; Lebensburger, J.; Lin, C.P.; Baskin, M.L.; Pachter, L.M. Adverse childhood experiences in children and adolescents with sickle cell disease: A retrospective cohort study. Pediatr. Blood Cancer 2022, 69, e29494. [Google Scholar] [CrossRef]
- Ladd, R.J.; Valrie, C.R.; Walcott, C.M. Risk and resilience factors for grade retention in youth with sickle cell disease. Pediatr. Blood Cancer 2014, 61, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Verma, T.; Rohan, J. Examination of Transition Readiness, Medication Adherence, and Resilience in Pediatric Chronic Illness Populations: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 1905. [Google Scholar] [CrossRef]
- Karlson, C.W.; Leist-Haynes, S.; Smith, M.; Faith, M.A.; Elkin, T.D.; Megason, G. Examination of risk and resiliency in a pediatric sickle cell disease population using the psychosocial assessment tool 2.0. J. Pediatr. Psychol. 2012, 37, 1031–1040. [Google Scholar] [CrossRef]
- Lau, N.; Yi-Frazier, J.P.; Bona, K.; Baker, K.S.; McCauley, E.; Rosenberg, A.R. Distress and resilience among adolescents and young adults with cancer and their mothers: An exploratory analysis. J. Psychosoc. Oncol. 2020, 38, 118–124. [Google Scholar] [CrossRef]
- Lee, S.; McMurtry, C.M.; Summers, C.; Edwards, K.; Elik, N.; Lumley, M.N. Quality of Life in Youth with Chronic Pain: An Examination of Youth and Parent Resilience and Risk Factors. Clin. J. Pain 2020, 36, 440–448. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Rothschild, C.B.; Rychlik, K.L.; Goodman, D.M.; Charleston, E.; Brown, M.L.; Michelson, K.N.; Navigate Study Investigators. Association Between Resilience and Psychological Morbidity in Parents of Critically Ill Children. Pediatr. Crit. Care Med. 2020, 21, e177–e185. [Google Scholar] [CrossRef]
- Vincent, A.; Beck, K.; Becker, C.; Zumbrunn, S.; Ramin-Wright, M.; Urben, T.; Quinto, A.; Schaefert, R.; Meinlschmidt, G.; Gaab, J.; et al. Psychological burden in patients with COVID-19 and their relatives 90 days after hospitalization: A prospective observational cohort study. J. Psychosom. Res. 2021, 147, 110526. [Google Scholar] [CrossRef]
- Lester, E.G.; Mace, R.A.; Bannon, S.M.; Popok, P.J.; Gates, M.V.; Meyers, E.; Tehan, T.; Sagueiro, D.; Rosand, J.; Macklin, E.A.; et al. Can a Dyadic Resiliency Program Improve Quality of Life in Cognitively Intact Dyads of Neuro-ICU Survivors and Informal Caregivers? Results from a Pilot RCT. Neurocritical Care 2021, 35, 756–766. [Google Scholar] [CrossRef] [PubMed]
- Elliott, A.M.; Burton, C.D.; Hannaford, P.C. Resilience does matter: Evidence from a 10-year cohort record linkage study. BMJ Open 2014, 4, e003917. [Google Scholar] [CrossRef]
- Brown, S.E.; Weisberg, D.F.; Sledge, W.H. Family caregiving for adults with sickle cell disease and extremely high hospital use. J. Health Psychol. 2016, 21, 2893–2902. [Google Scholar] [CrossRef]
- Hamideh, D.; Alvarez, O. Sickle cell disease related mortality in the United States (1999–2009). Pediatr. Blood Cancer 2013, 60, 1482–1486. [Google Scholar] [CrossRef]
- Calhoun, C.L.; Abel, R.A.; Pham, H.A.; Thompson, S.; King, A.A. Implementation of an educational intervention to optimize self-management and transition readiness in young adults with sickle cell disease. Pediatr. Blood Cancer 2019, 66, e27722. [Google Scholar] [CrossRef]
- Mulchan, S.S.; Valenzuela, J.M.; Crosby, L.E.; Diaz Pow Sang, C. Applicability of the SMART Model of Transition Readiness for Sickle-Cell Disease. J. Pediatr. Psychol. 2016, 41, 543–554. [Google Scholar] [CrossRef]
- Melita, N.; Diaz-Linhart, Y.; Kavanagh, P.L.; Sobota, A. Developing a Problem-solving Intervention to Improve Self-Management and Transition Readiness in Adolescents with Sickle Cell Disease. J. Pediatr. Nurs. 2019, 46, 26–32. [Google Scholar] [CrossRef]
- Rosenberg, A.R.; Bradford, M.C.; McCauley, E.; Curtis, J.R.; Wolfe, J.; Baker, K.S.; Yi-Frazier, J.P. Promoting resilience in adolescents and young adults with cancer: Results from the PRISM randomized controlled trial. Cancer 2018, 124, 3909–3917. [Google Scholar] [CrossRef]
- Rosenberg, A.R.; Bradford, M.C.; Junkins, C.C.; Taylor, M.; Zhou, C.; Sherr, N.; Kross, E.; Curtis, J.R.; Yi-Frazier, J.P. Effect of the Promoting Resilience in Stress Management Intervention for Parents of Children with Cancer (PRISM-P): A Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e1911578. [Google Scholar] [CrossRef]
- Gillard, A.; Gagnon, R.; Pashankar, F.; Balsamo, L.; Grafft, N.; Miranda, J.; Boruchov, D.; Neri, C.; Sprinz, P.; Longyear, C. Sense of mastery and attitude towards illness: Examining longitudinal benefits of a medical specialty camp for youth with sickle cell disease. Clin. Child Psychol. Psychiatry 2023, 28, 1012–1023. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Richardson, P.A.; Rajagopalan, A.V.; Bhandari, R.P. Factors Related to Agreement Between Child and Caregiver Report of Child Functioning with Chronic Pain: PROMIS Pediatric and Parent Proxy Report. Clin. J. Pain 2020, 36, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Reader, S.K.; Pantaleao, A.; Keeler, C.N.; Ruppe, N.M.; Kazak, A.E.; Rash-Ellis, D.L.; Wadman, J.; Miller, R.E.; Deatrick, J.A. Family Resilience from the Perspective of Caregivers of Youth with Sickle Cell Disease. J. Pediatr. Hematol. Oncol. 2020, 42, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Adams, E.L.; Smith, D.; Caccavale, L.J.; Bean, M.K. Parents Are Stressed! Patterns of Parent Stress Across COVID-19. Front. Psychiatry 2021, 12, 626456. [Google Scholar] [CrossRef]
- Catanzarite, A.; Bouck, J.R.; Matthes, M.; Goubeaux, D.L.; Carter, A.; LaMotte, J.E.; Jacob, S.A. Impact of Neighborhood Disadvantage on Preventive and Acute Care Utilization in Sickle Cell Disease. Pediatr. Blood Cancer 2025, 72, e31422. [Google Scholar] [CrossRef]
| Caregiver a (N = 55) | Child (N = 55) | |
|---|---|---|
| Age (Mean, SD) | 43.4 (7.1) | 15.2 (2.2) |
| Female Gender (N %) | 55, 100% | 24, 43.6% |
| Race (N, %) | ||
| Black or African American | 54, 98.2% | 53, 98.2% |
| White | 1, 1.8% | 0 |
| Other/Prefer not to say/No response | 0 | 2, 3.6% |
| Ethnicity (N, %) | ||
| Hispanic/Latino/Spanish Origin | 0 | 1, 1.8% |
| Not Hispanic/Latino/Spanish Origin | 50, 90.9% | 48, 87.3% |
| No response | 5, 9.1% | 6, 10.9% |
| Number of adults living in home (median, IQR) | 2 (1–2) | |
| Number of children living in home (median, IQR) | 2 (1–3) | |
| Highest level of completed education (N, %) | ||
| Some high school | 5, 9.1% | |
| Completed high school or GED | 20, 36.4% | |
| Trade school or associate degree | 15, 27.3% | |
| Bachelor’s degree | 8, 14.5% | |
| Post graduate coursework | 6, 10.9% | |
| Doctorate degree | 1, 1.8% | |
| Household annual income (N, %) | ||
| <$10,000 | 11, 20.0% | |
| $10,000–25,000 | 10, 18.2% | |
| $25,000–50,000 | 16, 29.1% | |
| $50,000–75,000 | 9, 16.3% | |
| $75,000–100,000 | 5, 9.1% | |
| >$100,000 | 4, 7.3% | |
| History of Stroke (N, %) | 20, 36.4% | |
| History of Transplant (N, %) | 4, 7.2% | |
| Number of ER Visits in last year (N, %) | ||
| 0 | 27, 49.1% | |
| 1–2 | 14, 25.5% | |
| ≥3 | 14, 25.5% | |
| Number of Hospitalizations in last year (N, %) | ||
| 0 | 26, 47.3% | |
| 1–2 | 16, 29.1% | |
| ≥3 | 13, 23.6% |
| Score | Mean (SD) | Median (IQR) | Range |
|---|---|---|---|
| Child CD-RISC | 68.5 (13.3) | 69 (60–78) | 35–92 |
| Caregiver CD-RISC | 75.8 (12.7) | 77 (70–84) | 46–99 |
| Child PSS-10 | 16.1 (6) | 16 (11–21) | 4–29 |
| Caregiver PSS-10 | 15.3 (7.1) | 14 (10–19) | 3–35 |
| Caregiver for Child CD-RISC | 67.4 (14.4) | 67 (59–76) | 23–99 |
| Discordant CD-RISC Items Between Caregiver for Child and Child Resilience Score | (N, %) |
|---|---|
| Good or bad, I believe that most things happen for a reason | p = 0.0025 |
| Parent > Child | 8 (14.55%) |
| Parent = Child | 22 (40%) |
| Parent < Child | 25 (45.45%) |
| I am able to handle unpleasant or painful feelings like sadness, fear, and anger | p = 0.0144 |
| Parent > Child | 7 (12.73%) |
| Parent = Child | 30 (54.55%) |
| Parent < Child | 18 (32.73%) |
| In dealing with life’s problems, sometimes you have to act on a hunch without knowing why | p = 0.0435 |
| Parent > Child | 11 (20%) |
| Parent = Child | 24 (43.64%) |
| Parent < Child | 20 (36.36%) |
| I work to attain my goals no matter what roadblocks I encounter along the way | p = 0.0315 |
| Parent > Child | 9 (16.36%) |
| Parent = Child | 27 (49.09%) |
| Parent < Child | 19 (34.55%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zavadil, J.A.; Azul, M.; Carpenter, B.D.; Calhoun, C. Resiliency in Child–Caregiver Dyads and the Impact on Health Outcomes in Sickle Cell Disease. Children 2025, 12, 394. https://doi.org/10.3390/children12040394
Zavadil JA, Azul M, Carpenter BD, Calhoun C. Resiliency in Child–Caregiver Dyads and the Impact on Health Outcomes in Sickle Cell Disease. Children. 2025; 12(4):394. https://doi.org/10.3390/children12040394
Chicago/Turabian StyleZavadil, Jessica A., Melissa Azul, Brian D. Carpenter, and Cecelia Calhoun. 2025. "Resiliency in Child–Caregiver Dyads and the Impact on Health Outcomes in Sickle Cell Disease" Children 12, no. 4: 394. https://doi.org/10.3390/children12040394
APA StyleZavadil, J. A., Azul, M., Carpenter, B. D., & Calhoun, C. (2025). Resiliency in Child–Caregiver Dyads and the Impact on Health Outcomes in Sickle Cell Disease. Children, 12(4), 394. https://doi.org/10.3390/children12040394