
Motor-Sensory Learning in Children with Disabilities: Does Piano Practice Help?


Abstract
1. Introduction
2. Method
2.1. Participants
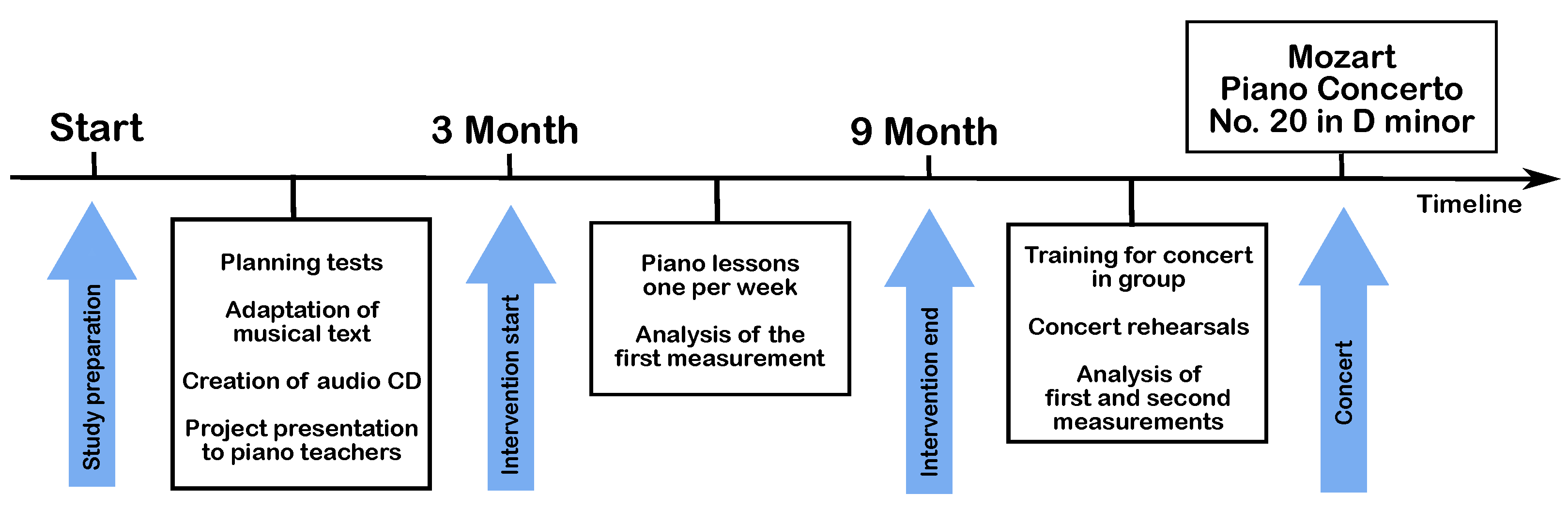
2.2. Design
2.3. Procedure
2.3.1. Box and Block Test
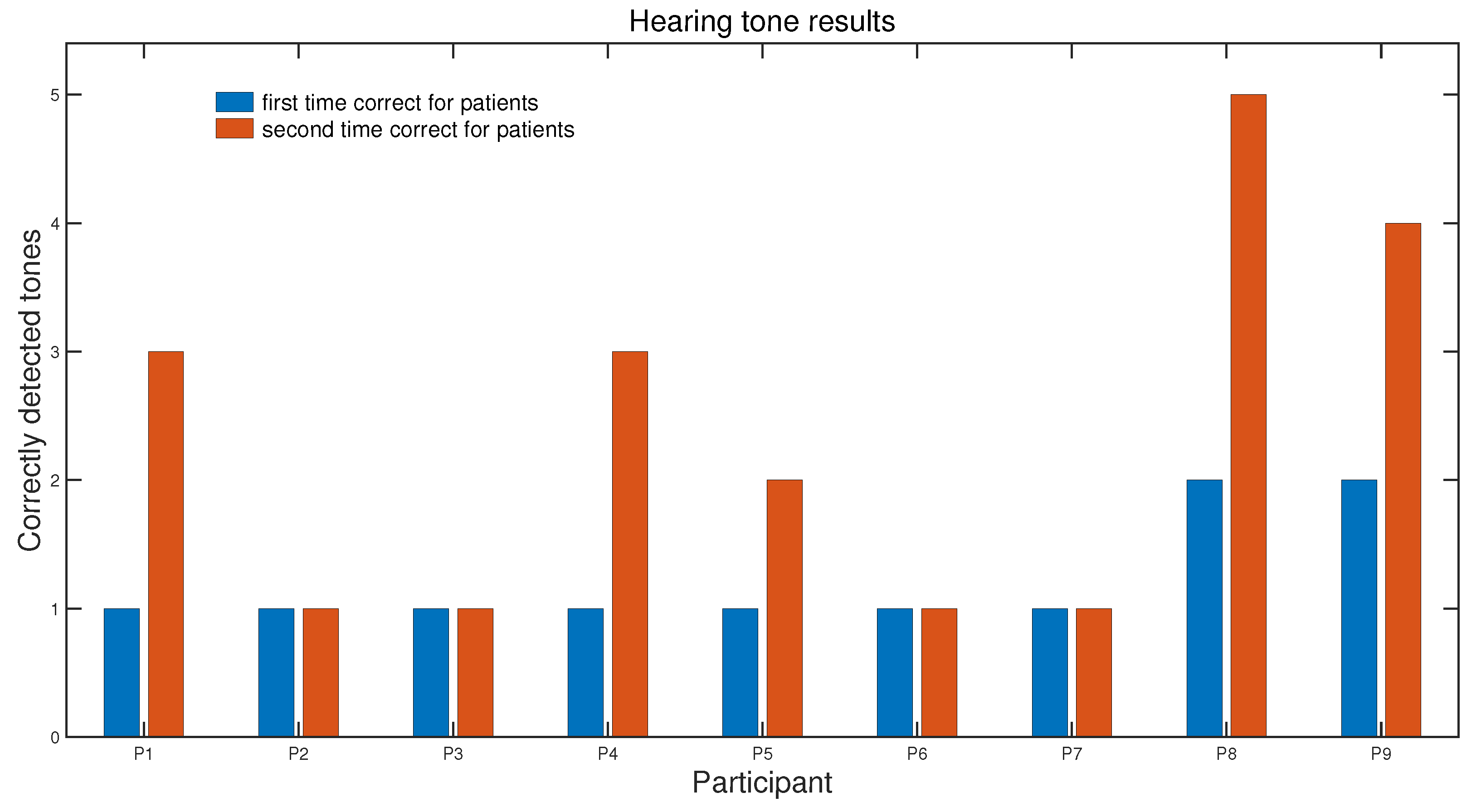
2.3.2. Tone Recognition Test
2.3.3. Hand Motor Tests on the Piano (Piano Tests)
- Task 1: The five fingers of the right hand were placed on the piano keys C to G with the thumb on C, the index finger on D, and so on. The participants were instructed to press a single key of the piano with each finger three times (hereafter mentioned as triple key test), in ascending and descending order, starting from the thumb and returning to the thumb via all fingers. Data were recorded for three trials.
- Task 2: The same as task 1 but performed with the left hand.
- Task 3: The same as task 1 but performed with both hands simultaneously.
- Task 4: The five fingers of the right hand were placed on the piano keys C to G with the thumb on C, the index finger on D, and so on. The ascending and descending order of playing from C to G, pressing each key once (hereafter mentioned as a single key test), was recorded for three trials.
- Task 5: The same as task 4 but performed with the left hand.
- Task 6: The same as task 4 but performed with both hands simultaneously.
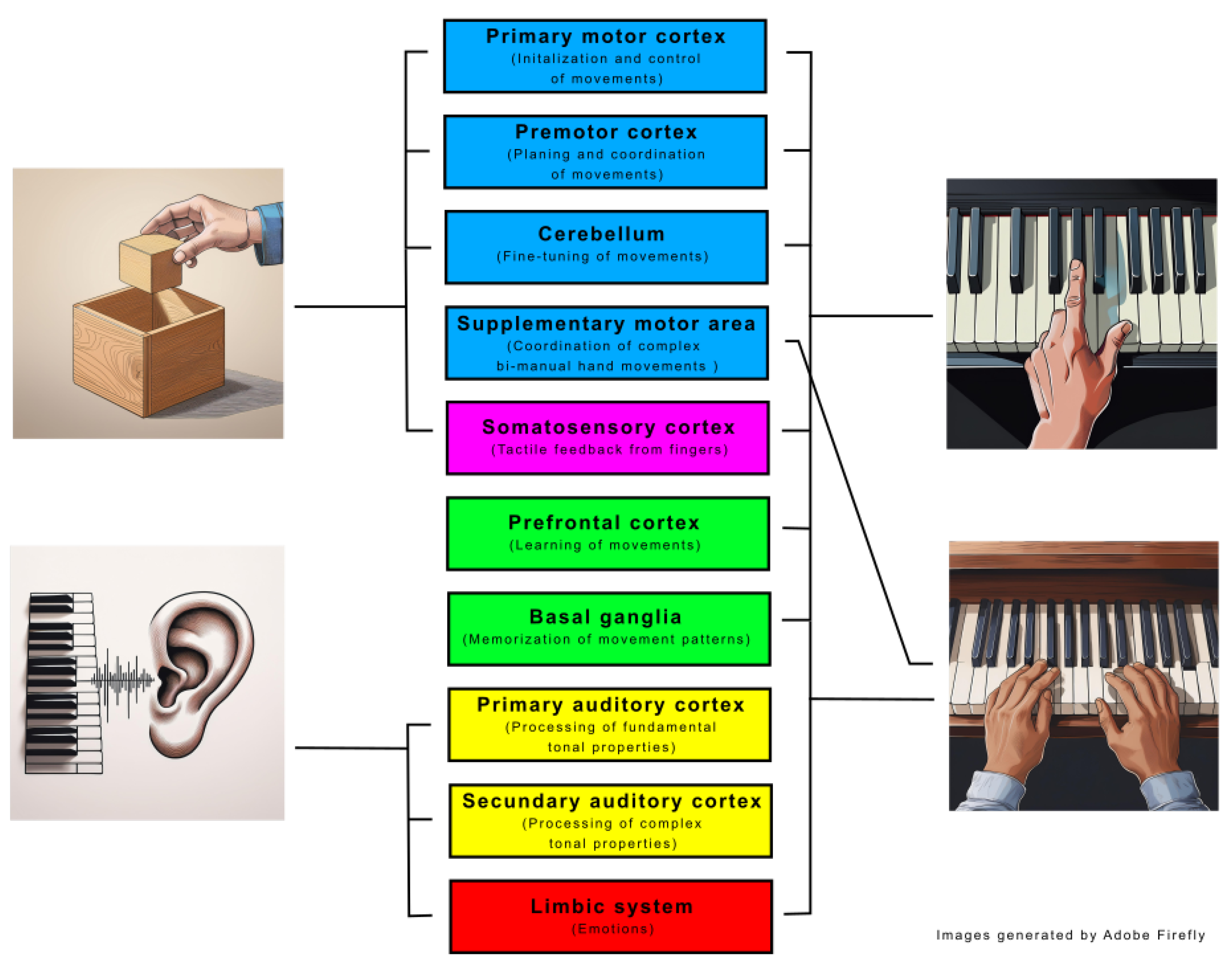
2.4. Involved Brain Regions in the Tests
2.5. Questionnaire for Participants
3. Results
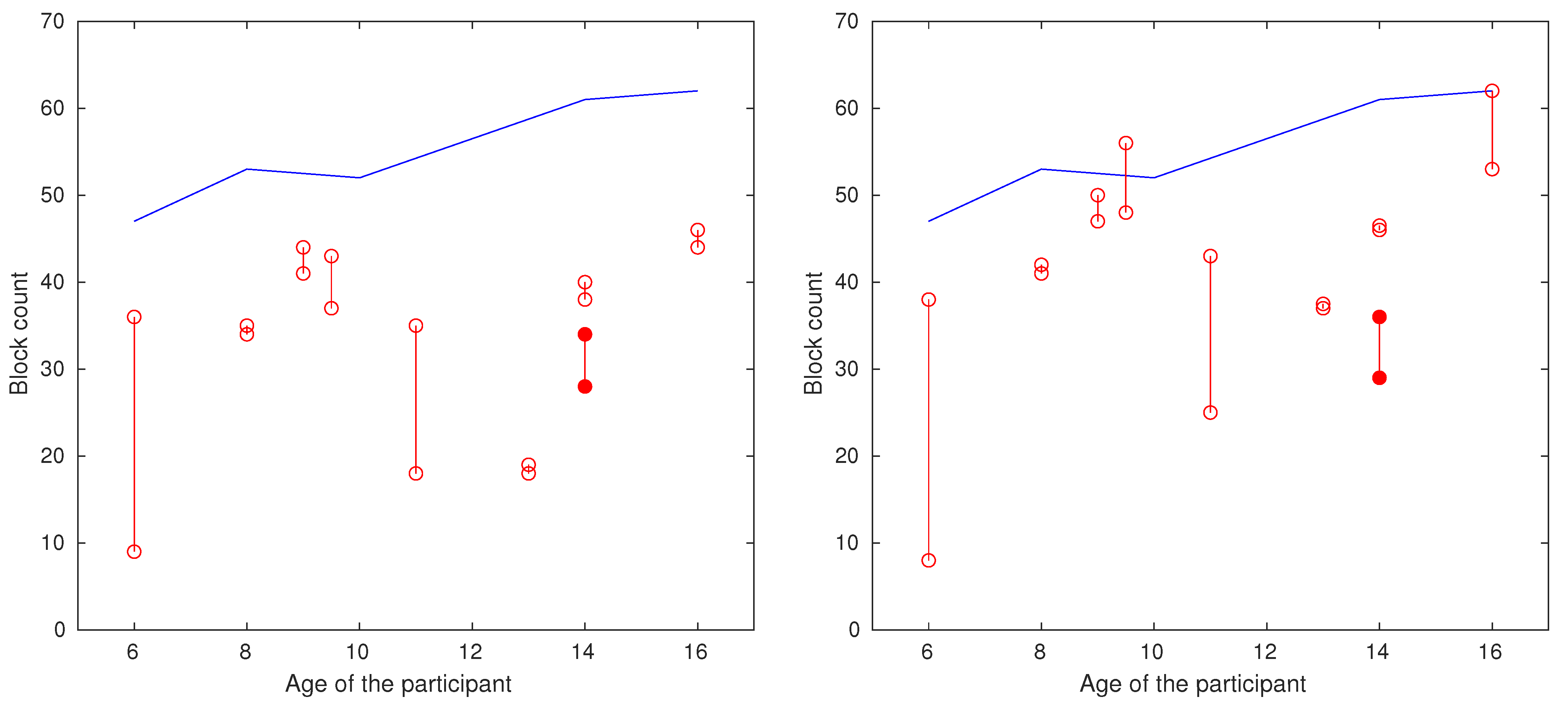
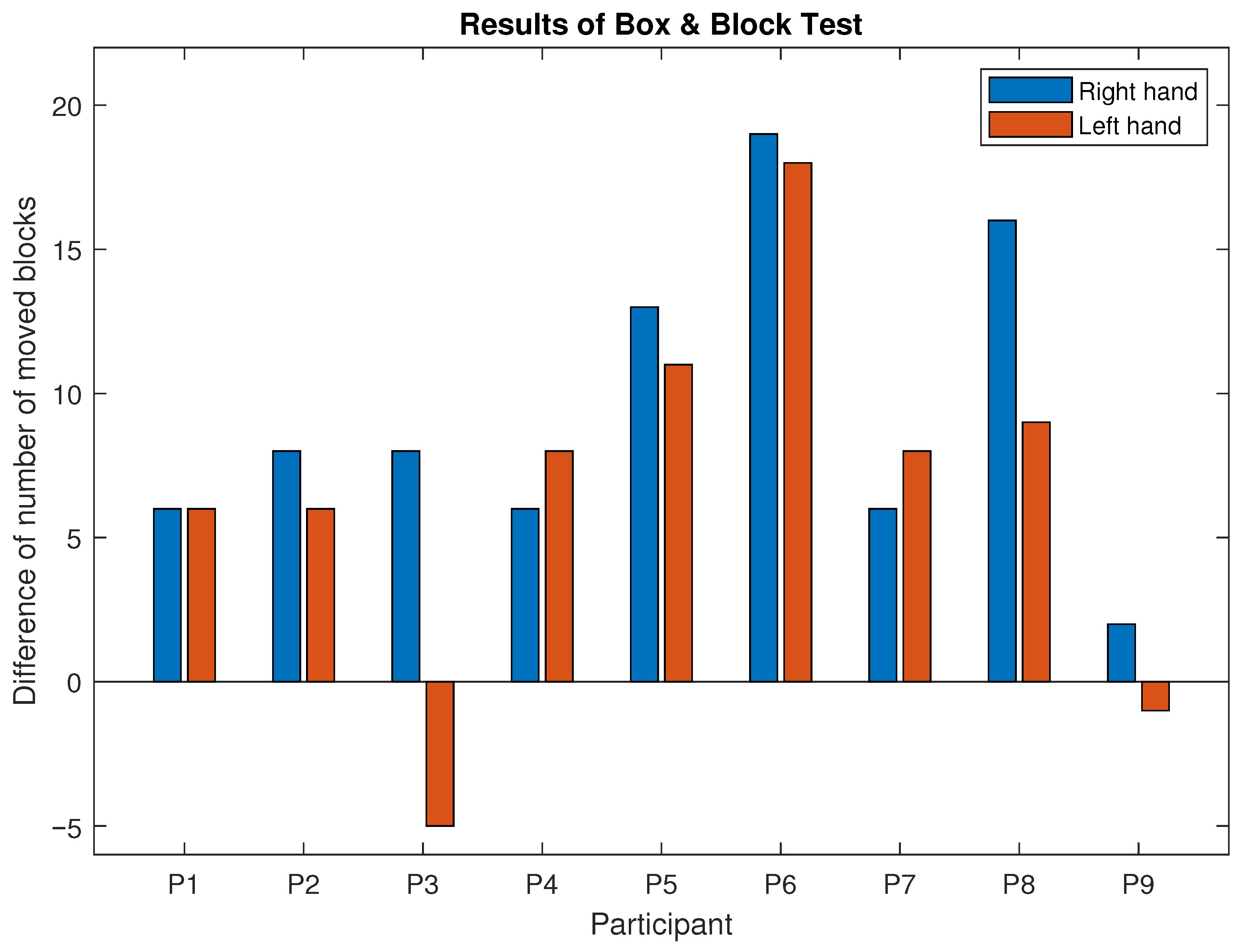
3.1. Results of BBT
3.2. Results of Tone Recognition Test
3.3. Results of the Piano Tests
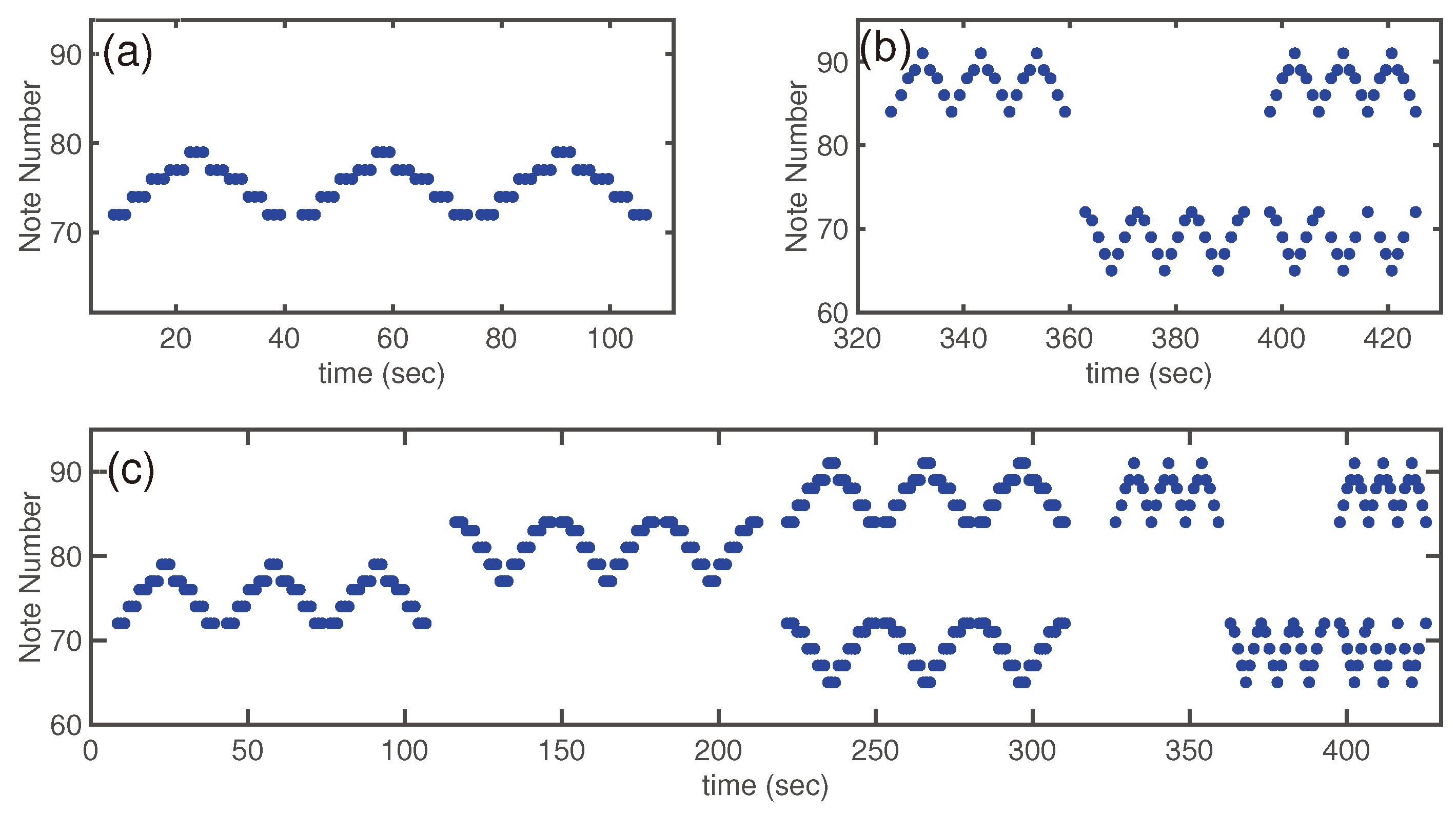
3.3.1. Visual Representation of the Ideal Piano Test
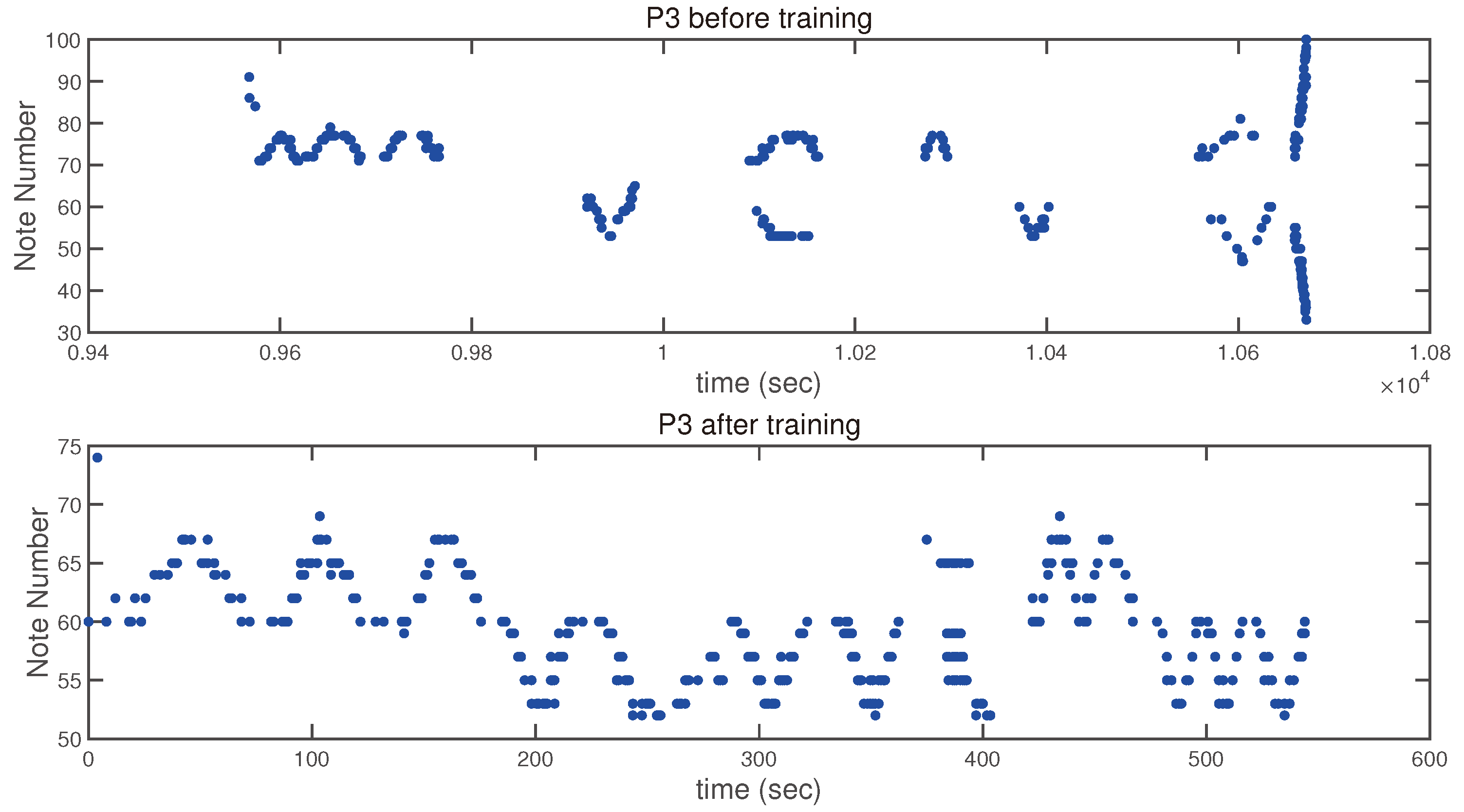
3.3.2. Visual Representation of the Piano Tests of a Participant
3.3.3. Evaluation of the Piano Tests of All Participants
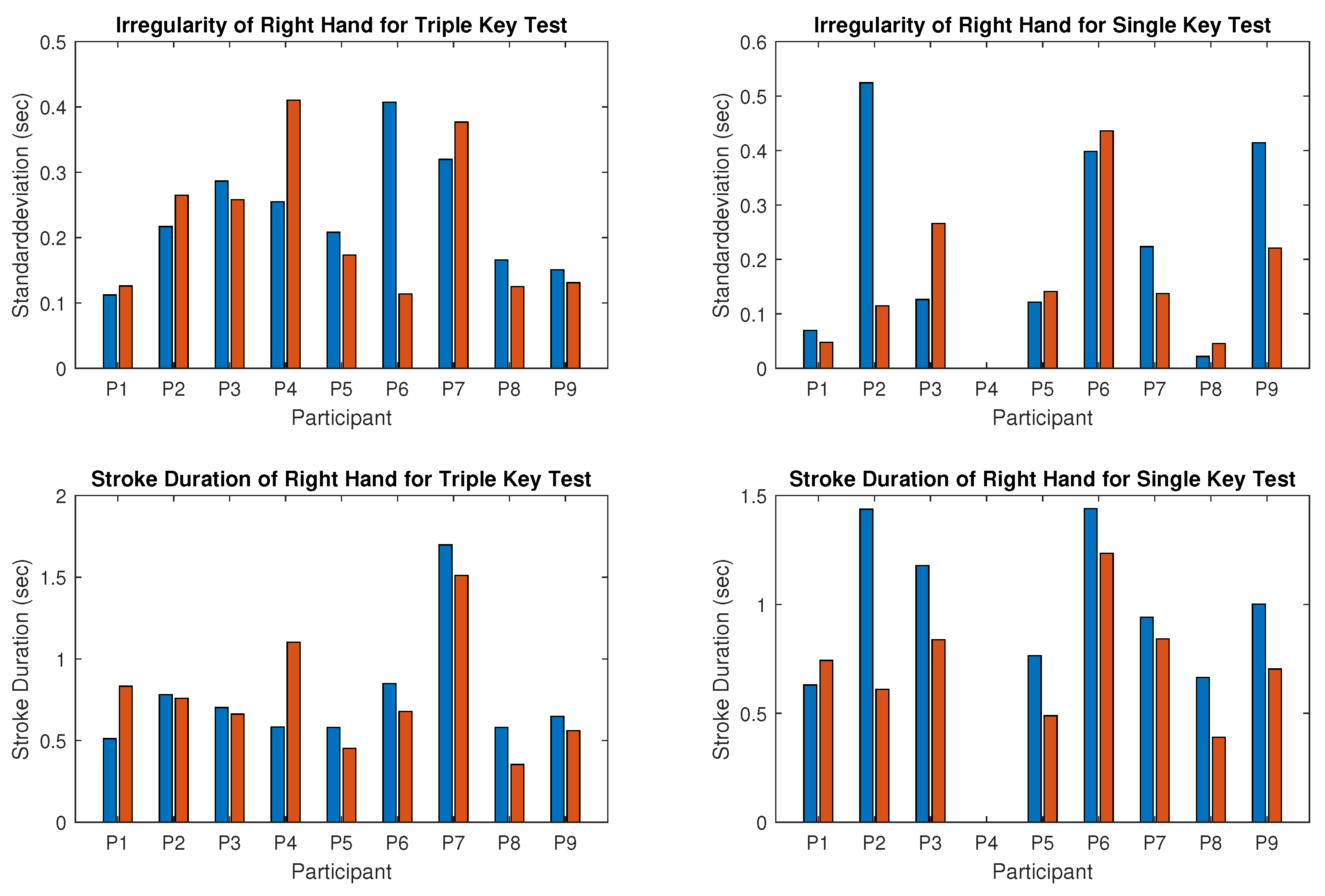
- Results for the right hand:The computed irregularity and stroke duration for the right hand, which was the dominant hand in seven of the nine participants, are illustrated in Figure 9. Reduced irregularity and shorter stroke duration indicate better performance. Regularity (opposite to irregularity shown in the upper panel of Figure 9) of the right hand improved in five of the nine participants during the triple key tests (Figure 9 left) and in four of the eight participants during the single key test (Figure 9 right). Participant 4 was unable to perform the single key test. Some participants showed no improvement, with either stable scores or slight deterioration. Statistical tests for right-hand regularity showed no significant changes (p-value > 0.05).The tempo (inverse of stroke duration shown in the lower panel of Figure 9) of the right hand increased in all participants except participant 1, who played slightly slower in both tests after training. For the whole group, this improvement was statistically significant (p-value < 0.05). Participant 4, with severe right-hand restriction, could only perform the triple key test and required multiple re-instructions, showing high irregularity.
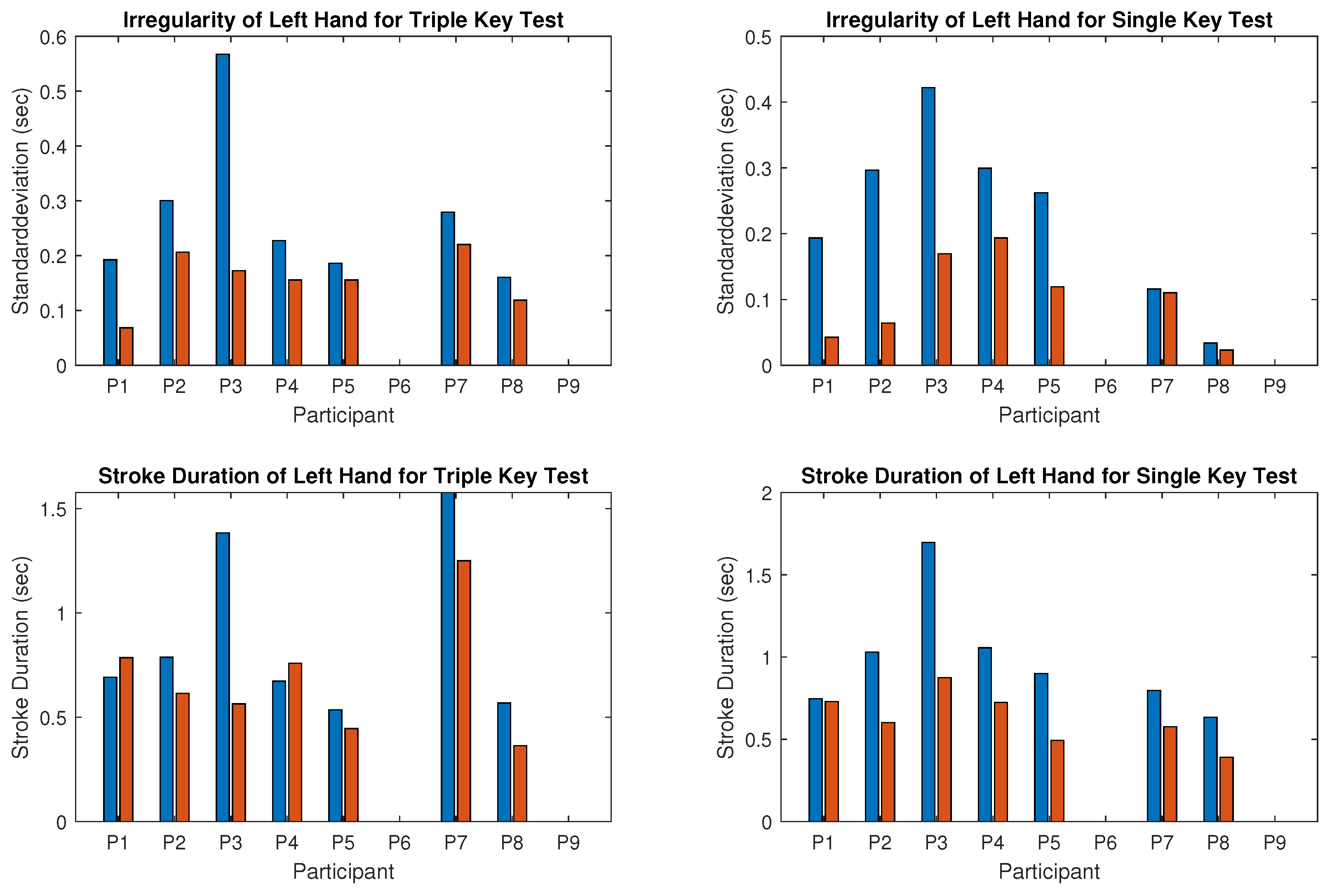
- Results for the left hand:Figure 10 presents the results for the left hand, typically the non-dominant hand, showing clear improvements in all participants except 6 and 9, who could not perform the test due to motor limitations. Regularity (opposite to irregularity shown in the upper panel of Figure 10) increased significantly after the training. For instance, irregularity in the triple key test decreased by more than half for participants 1 and 3, and similar reductions were observed in the single key test for participants 1, 2, 3, and 5. Group results were statistically significant (p-value < 0.001). The tempo (inverse stroke duration, lower panel of Figure 10) improved significantly (p-value < 0.005) in both tests for most participants, except for participants 1 and 4, who played slightly slower in the triple key test.
- Correlation between improvement and dominant hand:For all participants except 4 and 6, the left hand (non-dominant) showed clear improvements in regularity and tempo. Participant 6, left-hand dominant, improved in the right hand during the triple key test, while the regularity in the single key test remained almost unchanged. Participant 4, also left-hand dominant, could not perform the right-hand single key test and showed no improvement in the triple key test despite multiple instructions.
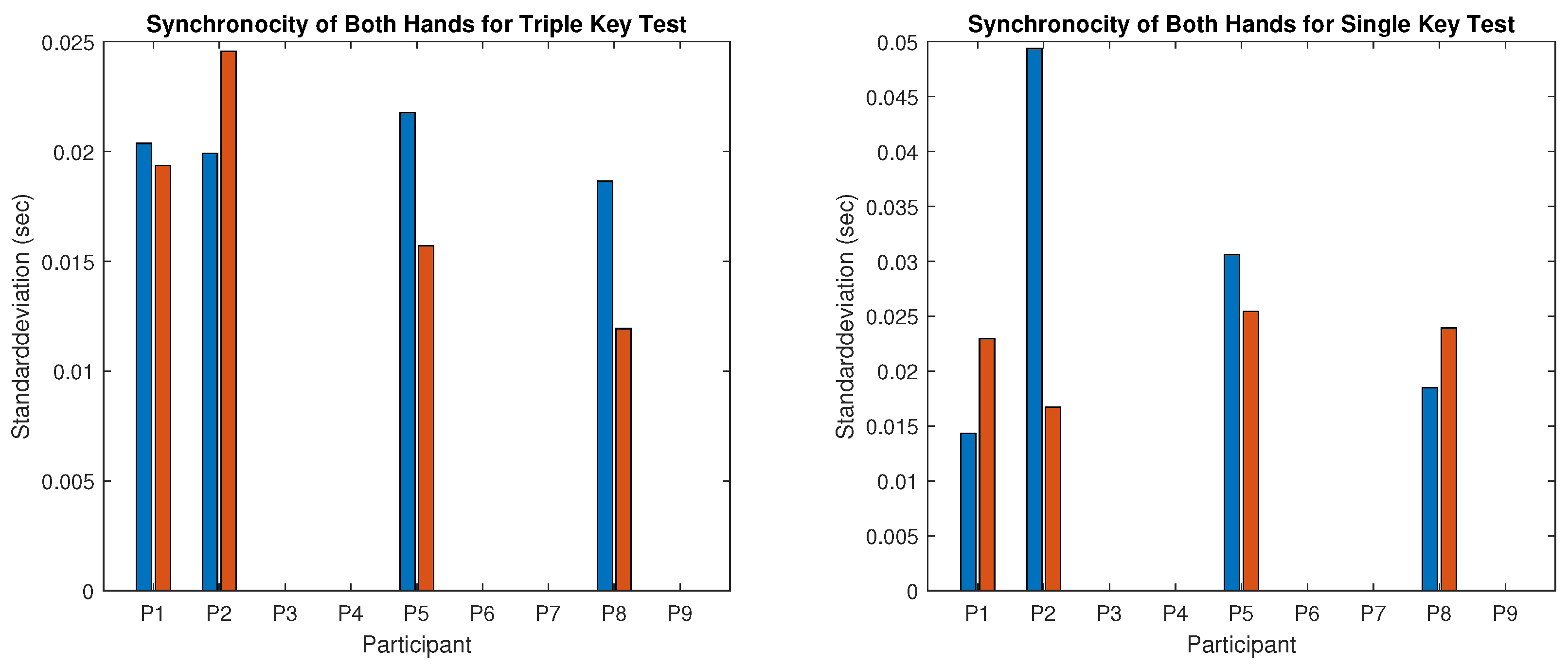
- Results for the synchronicity of both hands:The averaged synchronicity of both hands in the triple and single key tests, measured as the standard deviation of keystroke offsets, is shown in Figure 11. Due to motor limitations, only participants 1, 2, 5, and 8 could perform this test. Figure 11 reveals no clear correlation between training and synchronicity improvement. Participants 5 and 8 improved in the triple key test, and participant 2 improved in the single key test, while others showed no change or reduced synchronicity. The p-value indicates no significant improvement.
3.3.4. Results of the Questionnaire
4. Discussion
- The results of the standard BBT show a significant improvement (p-value < 0.001) after six months of piano training in a group of children and adolescents with disabilities.
- The regularity and tempo of consecutive and repeated finger strokes by the left hand, typically the non-dominant hand, also improved significantly during piano tests after the training (p-value < 0.001 and p-value < 0.005, respectively).
- The improvement in the regularity of the right hand for similar tests was not significant, but the tempo of the right hand improved significantly (p-value < 0.05).
- The questionnaire responses indicate that all participants thoroughly enjoyed the piano lessons and expressed a strong appreciation for music.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barbas, H. Connections underlying the synthesis of cognition, memory, and emotion in primate prefrontal cortices. Brain Res. Bull. 2000, 52, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Zatorre, R.J.; Chen, J.L.; Penhune, V.B. When the brain plays music: Auditory-motor interactions in music perception and production. Nat. Rev. Neurosci. 2007, 8, 547–558. [Google Scholar] [CrossRef]
- Miall, R.C.; Reckess, G.Z.; Imamizu, H. The cerebellum coordinates eye and hand tracking movements. Nat. Neurosci. 2001, 4, 638–644. [Google Scholar] [CrossRef]
- McIntosh, G.C.; Brown, S.H.; Rice, R.R.; Thaut, M.H. Rhythmic auditory-motor facilitation of gait patterns in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1997, 62, 22–26. [Google Scholar] [CrossRef]
- Thaut, M.H.; McIntosh, G.C.; Rice, R.R. Rhythmic facilitation of gait training in hemiparetic stroke rehabilitation. J. Neurol. Sci. 1997, 151, 207–212. [Google Scholar] [CrossRef]
- Drake, C.; Penel, A.; Bigand, E. Tapping in time with mechanically and expressively performed music. Music Percept. 2000, 18, 1–23. [Google Scholar] [CrossRef]
- Lahav, A.; Saltzman, E.; Schlaug, G. Action representation of sound: Audiomotor recognition network while listening to newly acquired actions. J. Neurosci. 2007, 27, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Baumann, S.; Koeneke, S.; Meyer, M.; Lutz, K.; Jäncke, L. A network for sensory-motor integration: What happens in the auditory cortex during piano playing without acoustic feedback? Ann. N. Y. Acad. Sci. 2005, 1060, 186–188. [Google Scholar] [CrossRef]
- Meyer-Heim, A.; van Hedel, H.J.; Baumann, T. Zerebralparese: Ein update. PäDiatrie Up2date 2014, 9, 183–214. [Google Scholar] [CrossRef]
- Marret, S.; Vanhulle, C.; Laquerriere, A. Pathophysiology of cerebral palsy. Handb. Clin. Neurol. 2013, 111, 169–176. [Google Scholar]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14, Erratum in Dev. Med. Child Neurol. 2007, 49, 480. [Google Scholar] [PubMed]
- Liuzzi, T.; Bompard, S.; Raponi, M.; D’Arienzo, F.; Staccioli, S.; Napoli, E.; Diotallevi, M.F.; Piga, S.; Giuliani, R.; Castelli, E. Euterpe music therapy method for children with cerebral palsy. Front. Neurol. 2024, 15, 1388712. [Google Scholar] [CrossRef]
- Chong, H.J.; Cho, S.R.; Jeong, E.; Kim, S.J. Finger exercise with keyboard playing in adults with cerebral palsy: A preliminary study. J. Exerc. Rehabil. 2013, 9, 420–425. [Google Scholar] [CrossRef]
- Yang, S.; Suh, J.H.; Kwon, S.; Chang, M.C. The effect of neurologic music therapy in patients with cerebral palsy: A systematic narrative review. Front. Neurol. 2022, 13, 852277. [Google Scholar] [CrossRef]
- Kim, S.J.; Yoo, G.E.; Shin, Y.K.; Cho, S.R. Gait training for adults with cerebral palsy following harmonic modification in rhythmic auditory stimulation. Ann. N. Y. Acad. Sci. 2020, 1473, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, D.; Hegde, S.; Thaut, M. Neural plasticity: The substratum of music-based interventions in neurorehabilitation. NeuroRehabilitation 2021, 48, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Santonja-Medina, C.S.; Marrades-Caballero, E.; Santonja-Medina, F.; Sanz-Mengibar, J.M. Neurologic Music Therapy Improves Participation in Children With Severe Cerebral Palsy. Front. Neurol. 2022, 13, 795533. [Google Scholar] [CrossRef] [PubMed]
- Foxx, R.M. Applied behavior analysis treatment of autism: The state of the art. Child Adolesc. Psychiatr. Clin. N. Am. 2008, 17, 821–834. [Google Scholar] [CrossRef]
- Zhang, Q.; Park, A.; Suh, K.H. Relationship between Playing Musical Instruments and Subjective Well-Being: Enjoyment of Playing Instruments Scale. Behav. Sci. 2024, 14, 744. [Google Scholar] [CrossRef]
- Tatiana, D.; Alexandra, Z. Piano with a twist: A pilot study exploring the preliminary effects of a piano therapy program for children with autism spectrum disorder. Arts Psychother. 2023, 82, 101987. [Google Scholar] [CrossRef]
- Alves-Pinto, A.; Turova, V.; Blumenstein, T.; Thienel, A.; Wohlschläger, A.; Lampe, R. fMRI assessment of neuroplasticity in youths with neurodevelopmental-associated motor disorders after piano training. Eur. J. Paediatr. Neurol. 2015, 19, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Federman, S.; Wiemer, D. Box and Block Test of Manual Dexterity: Norms for 6–19 Year Olds. Can. J. Occup. Ther. 1985, 52, 241–245. [Google Scholar] [CrossRef]
- Alves-Pinto, A.; Ehrlich, S.; Cheng, G.; Turova, V.; Blumenstein, T.; Lampe, R. Effects of short-term piano training on measures of finger tapping, somatosensory perception and motor-related brain activity in patients with cerebral palsy. Neuropsychiatr. Dis. Treat. 2017, 13, 2705–2718. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, M.; Lamontagne, A. Playing piano can improve upper extremity function after stroke: Case studies. Stroke Res. Treat. 2013, 2013, 159105. [Google Scholar] [CrossRef]
- Altenmüller, E.; Marco-Pallares, J.; Münte, T.; Schneider, S. Neural reorganization underlies improvement in stroke-induced motor dysfunction by music-supported therapy. Ann. N. Y. Acad. Sci. 2009, 1169, 395–405. [Google Scholar] [CrossRef]
- Schneider, S.; Münte, T.; Rodriguez-Fornells, A.; Sailer, M.; Altenmüller, E. Music-supported training is more efficient than functional motor training for recovery of fine motor skills in stroke patients. Music Perception Interdiscip. J. 2010, 27, 271–280. [Google Scholar] [CrossRef]
- Fedrizzi, E.; Pagliano, E.; Andreucci, E.; Oleari, G. Hand function in children with hemiplegic cerebral palsy: Prospective follow-up and functional outcome in adolescence. Dev. Med. Child Neurol. 2003, 45, 85–91, Erratum in Dev. Med. Child Neurol. 2003, 45, 206. [Google Scholar] [CrossRef]
- Siebers, A.; Oberg, U.; Skargren, E. The effect of modified constraint-induced movement therapy on spasticity and motor function of the affected arm in patients with chronic stroke. Physiother. Can. 2010, 62, 388–396. [Google Scholar] [CrossRef]
- Veerbeek, J.; Langbroek-Amersfoort, A.; van Wegen, E.; Meskers, C.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb After Stroke: A Systematic Review and Meta-analysis. Neurorehabilit. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Arceo, R.; Chen, S.; Ding, L.; Jia, J.; Yao, J. Effectiveness of interventions to improve hand motor function in individuals with moderate to severe stroke: A systematic review protocol. BMJ Open 2019, 9, e032413. [Google Scholar] [CrossRef] [PubMed]
- Karatekin, B.D.; Icagasioglu, A. The effect of therapeutic instrumental music performance method on upper extremity functions in adolescent cerebral palsy. Acta Neurol. Belg. 2021, 121, 1179–1189. [Google Scholar] [CrossRef]
- Lampe, R.; Thienel, A.; Mitternacht, J.; Blumenstein, T.; Turova, V.; Alves-Pinto, A. Piano training in youths with hand motor impairments after damage to the developing brain. Neuropsychiatr. Dis. Treat. 2015, 11, 1929–1938. [Google Scholar] [CrossRef] [PubMed]
- Thyen, U.; Konrad, K. Wachstum und neurobiologische Entwicklung im Kindes- und Jugendalter. In Psychiatrie und Psychotherapie des Kindes-und Jugendalters; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–29. [Google Scholar] [CrossRef]
- Amunts, K.; Schlaug, G.; Jäncke, L.; Steinmetz, H.; Schleicher, A.; Dabringhaus, A.; Zilles, K. Motor Cortex and Hand Motor Skills: Structural Compliance in the Human Brain. Hum. Brain Mapp. 1997, 5, 206–221. [Google Scholar] [CrossRef]
- Cheng, L.; Chiu, Y.; Lin, Y.; Li, W.; Hong, T.; Yang, C.; Shih, C.; Yeh, T.; Tseng, W.; Yu, H.; et al. Long-term musical training induces white matter plasticity in emotion and language networks. Hum. Brain Mapp. 2023, 44, 5–17. [Google Scholar] [CrossRef] [PubMed]
- François, C.; Grau-Sánchez, J.; Duarte, E.; Rodriguez-Fornells, A. Musical training as an alternative and effective method for neuro-education and neuro-rehabilitation. Front. Psychol. 2015, 6, 475. [Google Scholar] [CrossRef]
- Schlaug, G. Musicians and music making as a model for the study of brain plasticity. Prog. Brain Res. 2015, 217, 37–55. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Gender | Age (Years) | Dominant Hand | GMFCS |
|---|---|---|---|---|
| P1 | M | 9 | Right | I |
| P2 | M | 8 | Right | I |
| P3 | F | 14 | Right | II |
| P4 | M | 11 | Left | II |
| P5 | M | 9 | Right | II |
| P6 | M | 13 | Left | III |
| P7 | M | 14 | Right | I |
| P8 | M | 16 | Right | I |
| P9 | M | 6 | Right | II |
| Participant | BBT r. h. | BBT l. h. | Irr. r. h. | Dur. r. h. | Irr. l. h. | Dur. l. h. | Syn. b. Hands |
|---|---|---|---|---|---|---|---|
| P1 | +13.6% | +14.6% | −9.7% | +40.3% | −71.2% | +5.6% | +27.6% |
| P2 | +23.5% | +17.1% | −28.0% | −30.1% | −54.8% | −31.8% | −21.4% |
| P3 | +28.6% | −14.7% | +50.3% | −17.3% | −64.7% | −53.8% | NAN |
| P4 | +38.9% | +22.9% | NAN | NAN | −33.5% | −9.3% | NAN |
| P5 | +28.3% | +29.7% | −0.3% | −29.0% | −35.5% | −30.9% | −22.4% |
| P6 | +105.5% | +94.7% | −31.3% | −17.2% | NAN | NAN | NAN |
| P7 | +15.0% | +21.1% | −10.4% | −10.8% | −13.0% | −24.2% | NAN |
| P8 | +34.8% | +20.5% | +42.1% | −40.3% | −28.7% | −37.1% | −3.3% |
| P9 | +5.6% | −11.1% | −30.0% | −21.7% | NAN | NAN | NAN |
| Q. No. | Question | Answer | Percentage |
|---|---|---|---|
| 1. | Do you like taking piano lessons? | Yes | 100% |
| Sometimes | 0% | ||
| No | 0% | ||
| 2. | Was it difficult to learn to play the piano? | Yes | 31% |
| A little bit | 31% | ||
| No | 38% | ||
| 3. | What do you particularly like about playing the piano? | Techniques | 16% |
| Melody | 38% | ||
| Both | 46% | ||
| 4. | Where are the high and low tones? | Correct | 84% |
| False | 16% | ||
| 5. | How do you learn to read the musical notes? | Colors | 62% |
| Numbers | 15% | ||
| Letters | 15% | ||
| Notes | 8% | ||
| 6. | Do you have a piano or keyboard at home? | Piano | 38% |
| Keyboard | 24% | ||
| No | 38% | ||
| 7. | Do you like playing for others? | Yes | 77% |
| Sometimes | 15% | ||
| Never tried | 8% | ||
| 8. | Do you enjoy playing with others? | Yes | 77% |
| Depends | 15% | ||
| No | 8% | ||
| 9. | Does anyone else in your family play the piano? | Yes | 54% |
| No | 46% | ||
| 10. | What do you feel after you learn to play the piano? | Proud | 100% |
| Satisfied | 0% | ||
| Disappointed | 0% | ||
| 11. | Were the piano tests boring or enjoyable? | Enjoyable | 100% |
| Tolerable | 0% | ||
| Boring | 0% | ||
| 12. | What is your favorite music? | Rock, Classical, Rap, Schlager, Everything except Schlager, Drum music, Children’s music, Robot music |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strübbe, S.; Roy, S.; Sidorenko, I.; Lampe, R. Motor-Sensory Learning in Children with Disabilities: Does Piano Practice Help? Children 2025, 12, 335. https://doi.org/10.3390/children12030335
Strübbe S, Roy S, Sidorenko I, Lampe R. Motor-Sensory Learning in Children with Disabilities: Does Piano Practice Help? Children. 2025; 12(3):335. https://doi.org/10.3390/children12030335
Chicago/Turabian StyleStrübbe, Simon, Susmita Roy, Irina Sidorenko, and Renée Lampe. 2025. "Motor-Sensory Learning in Children with Disabilities: Does Piano Practice Help?" Children 12, no. 3: 335. https://doi.org/10.3390/children12030335
APA StyleStrübbe, S., Roy, S., Sidorenko, I., & Lampe, R. (2025). Motor-Sensory Learning in Children with Disabilities: Does Piano Practice Help? Children, 12(3), 335. https://doi.org/10.3390/children12030335