

Neurodevelopmental Disorders and Connective Tissue-Related Symptoms: An Exploratory Case-Control Study in Children

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
- Varicose veins, vasculitis, and haemorrhoids;
- Striae rubrae, skin irregularities, or redness;
- Excessive sweating of the hands and feet;
- Joint inflammation and rheumatism;
- Joint dislocations and subluxations/dislocations;
- Joint pain involving 1 to 3 large joints lasting for more than 3 months;
- Back pain, transient muscle pain in the limbs, or chronic fatigue;
- Hip dysplasia, scoliosis, or kyphosis;
- Inguinal, umbilical, abdominal, or disc hernias;
- Flat feet;
- Constipation, diarrhoea, or alternating bowel patterns;
- Heartburn, gastroesophageal reflux, or hiatal hernia;
- Use of orthodontic appliances;
- Tactile, visual, auditory, olfactory, or gustatory hypersensitivity;
- Myopia or drooping eyelids, including unilateral or bilateral ptosis;
- Immune and/or autoimmune diseases.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Subject’s gender:
- Male
- Female
- Subject’s diagnosis:
- Autism
- ADHD
- Tourette’s syndrome
- Control
- How many brothers does the subject have?
- How many sisters does the subject have?
- Has the child or their parents had high blood pressure on two or three occasions?
- Has the child or their parents had varicose veins, vasculitis, or haemorrhoids?
- Has the child or their parents had stretch marks, skin discolouration, or unexplained reddened skin?
- Has the child or their parents had excessive sweating of the palms and/or soles of the feet?
- Has the child or their parents had joint inflammation or rheumatism (bursitis, tenosynovitis, etc.)?
- Has the child or their parents had dislocations, subluxations, or luxation of one or more joints on more than one occasion?
- Has the child or their parents had joint pain involving 1 to 3 large joints for more than 3 months?
- Has the child or their parents had back pain, transient muscle aches in the limbs (e.g., growing pains), or symptoms of chronic fatigue?
- Has the child or their parents had hip dysplasia, scoliosis, or a curved spine?
- Has the child or their parents had inguinal, umbilical, or abdominal hernias, or herniated discs?
- Has the child or their parents had flat feet?
- Has the child or their parents had constipation, diarrhoea, or alternating bowel habits?
- Has the child or their parents had heartburn, gastro-oesophageal reflux, or a hiatus hernia?
- Has the child or their parents had rectal or uterine prolapse, or urinary or faecal incontinence?
- Has the child or their parents worn or wear orthodontic appliances?
- Has the child or their parents had hypersensitivity to touch (feeling tags on trousers, discomfort with a belt, feeling of tight trousers), sight (perception of bright lights, glare), hearing (perception of reverberations, amplified noises), smell (heightened perception of odours, dysosmia), or taste?
- Has the child or their parents had a diagnosis of myopia or drooping eyelids (ptosis), either unilateral or bilateral? Has the child or their parents had any immune or autoimmune diseases? (e.g., type 1 diabetes, coeliac disease, thyroiditis, rheumatoid arthritis, Crohn’s disease, polyneuropathy, multiple sclerosis, etc.)
- Has the child or have the parents had, or do they currently have, any immune or autoimmune diseases? (e.g., type 1 diabetes, coeliac disease, thyroiditis, rheumatoid arthritis, Crohn’s disease, polyneuropathies, multiple sclerosis, etc.)
- Genere del soggetto:
- Maschio
- Femmina
- Patologia del soggetto:
- Autismo
- ADHD
- Sindrome di Tourette
- Controllo
- Quanti fratelli ha il soggetto?
- Quante sorelle ha il soggetto?
- Il bambino o i genitori hanno presentato o presentano ipertensione arteriosa in due o tre rilevazioni?
- Il bambino o i genitori hanno presentato o presentano vene varicose, vasculiti o emorroidi?
- Il bambino o i genitori hanno presentato o presentano striae rubre, smagliature e segni cutanei, cute arrossata senza apparente causa?
- Il bambino o i genitori hanno presentato o presentano un eccesso di sudorazione ai palmi delle mani e/o alle piante dei piedi?
- Il bambino o i genitori hanno presentato o presentano infiammazioni o reumatismi articolari (borsiti, tenosinoviti, ecc.)?
- Il bambino o i genitori hanno presentato o presentano dislocazioni, sublussazioni o lussazioni di una o più articolazioni in più di una occasione?
- Il bambino o i genitori hanno presentato o presentano dolore articolare coinvolgente da 1 a 3 grosse articolazioni lamentato per più di 3 mesi?
- Il bambino o i genitori hanno presentato o presentano dolore alla schiena, dolori muscolari transitori agli arti (ad es. dolori della crescita) o sintomi da affaticamento cronico?
- Il bambino o i genitori hanno presentato o presentano displasia dell’anca, scoliosi o dorso curvo?
- Il bambino o i genitori hanno presentato o presentano ernie inguinali, ombelicali, addominali oppure ernie discali?
- Il bambino o i genitori hanno presentato o presentano piedi piatti?
- Il bambino o i genitori hanno presentato o presentano stipsi, diarrea o alvo alterno?
- Il bambino o i genitori hanno presentato o presentano pirosi retrosternale, reflusso gastroesofageo o ernia iatale?
- Il bambino o i genitori hanno presentato o presentano prolassi rettali/uterini oppure incontinenza urinaria e/o fecale?
- Il bambino o i genitori hanno utilizzato o utilizzano apparecchi ortodontici?
- Il bambino o i genitori hanno presentato o presentano ipersensorialità a livello tattile (percepiscono etichette dei pantaloni, fastidio per cintura, senso di pantaloni stretti), a livello visivo (percezione di luci intense, abbagliamenti), a livello uditivo (percezione di rimbombi, rumori accentuati), a livello olfattivo (percezioni accentuate di odori, disosmie) a livello gustative?
- Il bambino o i genitori hanno presentato o presentano un quadro oculistico di miopia oppure un rilievo di palpebre cadenti o ptosi palpebrale mono o bi laterale?
- Il bambino o i genitori hanno presentato o presentano malattie immunitarie e/o autoimmunitarie? (es. diabete di tipo 1, celiachia, tiroiditi, artrite reumatoide, morbo di Crohn, polineuropatie, sclerosi multipla, etc.)
References
- Huisman-van Dijk, H.M.; Schoot, R.; Rijkeboer, M.M.; Mathews, C.A.; Cath, D.C. The relationship between tics, OC, ADHD and autism symptoms: A cross- disorder symptom analysis in Gilles de la Tourette syndrome patients and family-members. Psychiatry Res. 2016, 237, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Morris-Rosendahl, D.J.; Crocq, M.A. Neurodevelopmental disorders—The history and future of a diagnostic concept. Dialogues Clin. Neurosci. 2020, 22, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Karlsson, H.; Dalman, C.; Widman, L.; Rai, D.; Gardner, R.M.; Magnusson, C.; Sandin, S.; Tabb, L.P.; Newschaffer, C.J.; et al. The Familial Risk of Autism Spectrum Disorder with and without Intellectual Disability. Autism Res. 2020, 13, 2242–2250. [Google Scholar] [CrossRef]
- Yang, Z.; Wu, H.; Lee, P.H.; Tsetsos, F.; Davis, L.K.; Yu, D.; Lee, S.H.; Dalsgaard, S.; Haavik, J.; Barta, C.; et al. Investigating Shared Genetic Basis Across Tourette Syndrome and Comorbid Neurodevelopmental Disorders Along the Impulsivity-Compulsivity Spectrum. Biol. Psychiatry 2021, 90, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E. Obsessive-compulsive disorder and spectrum across the life span. Int. J. Psychiatry Clin. Pract. 2005, 9, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Darrow, S.M.; Grados, M.; Sandor, P.; Hirschtritt, M.E.; Illmann, C.; Osiecki, L.; Dion, Y.; King, R.; Pauls, D.; Budman, C.L.; et al. Autism Spectrum Symptoms in a Tourette’s Disorder Sample. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 610–617.e1. [Google Scholar] [CrossRef] [PubMed]
- Petti, T.; Gupta, M.; Fradkin, Y.; Gupta, N. Management of sleep disorders in autism spectrum disorder with co-occurring attention-deficit hyperactivity disorder: Update for clinicians. BJPsych Open 2023, 10, e11. [Google Scholar] [CrossRef]
- Lau-Zhu, A.; Fritz, A.; McLoughlin, G. Overlaps and distinctions between attention deficit/hyperactivity disorder and autism spectrum disorder in young adulthood: Systematic review and guiding framework for EEG-imaging research. Neurosci. Biobehav. Rev. 2019, 96, 93–115. [Google Scholar] [CrossRef]
- Vasa, R.A.; Mostofsky, S.H.; Ewen, J.B. The Disrupted Connectivity Hypothesis of Autism Spectrum Disorders: Time for the Next Phase in Research. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2016, 1, 245–252. [Google Scholar] [CrossRef]
- Tomasi, D.; Volkow, N.D. Reduced Local and Increased Long-Range Functional Connectivity of the Thalamus in Autism Spectrum Disorder. Cereb. Cortex 2019, 29, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Geier, D.A.; King, P.G.; Sykes, L.K.; Mehta, J.A.; Geier, M.R. Shared Brain Connectivity Issues, Symptoms, and Comorbidities in Autism Spectrum Disorder, Attention Deficit/Hyperactivity Disorder, and Tourette Syndrome. Brain Connect. 2015, 5, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Staines, D.R. Is chronic fatigue syndrome an autoimmune disorder of endogenous neuropeptides, exogenous infection and molecular mimicry? Med. Hypotheses 2004, 62, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Coon, E.A.; Cheshire, W.P., Jr. Sweating Disorders. Continuum 2020, 26, 116–137. [Google Scholar] [CrossRef]
- Parvaneh, V.J.; Shahvaladi, H.; Rahmani, K.; Yekta, S.J.; Gorji, F.A.; Shiari, R.; Abdollahimajd, F. Correlation between benign joint hypermobility syndrome and primary focal hyperhidrosis in children: A novel concept. BMC Musculoskelet. Disord. 2020, 21, 268. [Google Scholar] [CrossRef] [PubMed]
- Fikree, A.; Chelimsky, G.; Collins, H.; Kovacic, K.; Aziz, Q. Gastrointestinal involvement in the Ehlers-Danlos syndromes. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.B.; Kretschmar, J.M.; Gerhardt, D.C.; Winship, D.H.; Winn, D.; Treadwell, E.L.; Sharp, G.C. Gastrointestinal manifestations of mixed connective tissue disease. Gastroenterology 1990, 98 Pt 1, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Balasco, L.; Provenzano, G.; Bozzi, Y. Sensory Abnormalities in Autism Spectrum Disorders: A Focus on the Tactile Domain, From Genetic Mouse Models to the Clinic. Front. Psychiatry 2019, 10, 1016. [Google Scholar] [CrossRef] [PubMed]
- Cikes, N. Central nervous system involvement in systemic connective tissue diseases. Clin. Neurol. Neurosurg. 2006, 108, 311–317. [Google Scholar] [CrossRef]
- Kurosinski, P.; Götz, J. Glial cells under physiologic and pathologic conditions. Arch. Neurol. 2002, 59, 1524–1528. [Google Scholar] [CrossRef]
- Chien, Y.L.; Wu, P.Y.; Wu, J.H.; Huang, W.L.; Hsiao, C.C.; Hsieh, Y.T.; Cheng, T.; Gau, S.S.; Chen, W.L. Corneal structural alterations in autism spectrum disorder: An in vivo confocal microscopy study. Autism Res. 2023, 16, 2316–2325. [Google Scholar] [CrossRef]
- Zoccante, L.; Ciceri, M.L.; Gozzi, L.A.; Gennaro, G.D.; Zerman, N. The “Connectivome Theory”: A New Model to Understand Autism Spectrum Disorders. Front. Psychiatry 2021, 12, 794516. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Islam, M.R.; Yamin, M.; Islam, M.M.; Sarker, M.T.; Meem, A.F.K.; Akter, A.; Emran, T.B.; Cavalu, S.; Sharma, R. Emerging Role of Neuron-Glia in Neurological Disorders: At a Glance. Oxid. Med. Cell. Longev. 2022, 2022, 3201644. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Puhr, R. Bias-reduced and separation-proof conditional logistic regression with small or sparse data sets. Stat. Med. 2010, 29, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Schemper, M. A solution to the problem of separation in logistic regression. Stat. Med. 2002, 21, 2409–2419. [Google Scholar] [CrossRef]
- Guinchat, V.; Baeza-Velasco, C.; Bulbena, A.; Castori, M. Editorial: Neurodevelopmental, neuropsychiatric and psychosocial correlates of joint hypermobility and related disorders. Front. Psychiatry 2022, 13, 1109515. [Google Scholar] [CrossRef]
- Poshattiwar, R.S.; Acharya, S.; Shukla, S.; Kumar, S. Neurological Manifestations of Connective Tissue Disorders. Cureus 2023, 15, e47108. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.G.; Hossain, W.A.; Steinle, J.; Gao, H.; Cox, E.; Niu, Y.; Quach, M.; Veatch, O.J. Connective Tissue Disorders and Fragile X Molecular Status in Females: A Case Series and Review. Int. J. Mol. Sci. 2022, 23, 9090. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Cheyne, J.A.; Duque, G.A.; Ayala-Zapata, S.; Saldarriaga-Gil, W.; Hagerman, P.; Hagerman, R.; Payán-Gómez, C. Fragile X syndrome and connective tissue dysregulation. Clin. Genet. 2019, 95, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, M.; Kotz, R.; Ledl, T.; Hauser, G.; Sluga, M. Prevalence of flat foot in preschool-aged children. Pediatrics 2006, 118, 634–639. [Google Scholar] [CrossRef]
- Xu, L.; Gu, H.; Zhang, Y.; Sun, T.; Yu, J. Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8247. [Google Scholar] [CrossRef]
- Kaya Mutlu, E.; Birinci, T.; Kaya Aytutuldu, G.; Mutlu, C.; Razak Ozdincler, A. The investigation of foot structure within children who have attention-deficit hyperactivity disorder: A case-controlled study. J. Pediatr. Orthop. B 2022, 31, e24–e30. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, K.B.; Jeong, J.O.; Kwon, N.Y.; Jeong, S.M. Correlation of foot posture index with plantar pressure and radiographic measurements in pediatric flatfoot. Ann. Rehabil. Med. 2015, 39, 10–17. [Google Scholar] [CrossRef]
- Pezaro, S.; Brock, I.; Buckley, M.; Callaway, S.; Demirdas, S.; Hakim, A.; Harris, C.; High Gross, C.; Karanfil, M.; Le Ray, I.; et al. Management of childbearing with hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorders: A scoping review and expert co-creation of evidence-based clinical guidelines. PLoS ONE 2024, 19, e0302401. [Google Scholar] [CrossRef] [PubMed]
- Loblein, H.J.; Vukmirovich, P.W.; Donofrio, M.T.; Sanz, J.H. Prevalence of neurodevelopmental disorders in a clinically referred sample of children with CHD. Cardiol. Young 2023, 33, 619–626. [Google Scholar] [CrossRef]
- Morton, P.D.; Ishibashi, N.; Jonas, R.A. Neurodevelopmental Abnormalities and Congenital Heart Disease: Insights Into Altered Brain Maturation. Circ. Res. 2017, 120, 960–977. [Google Scholar] [CrossRef]
- Nattel, S.N.; Adrianzen, L.; Kessler, E.C.; Andelfinger, G.; Dehaes, M.; Côté-Corriveau, G.; Trelles, M.P. Congenital Heart Disease and Neurodevelopment: Clinical Manifestations, Genetics, Mechanisms, and Implications. Can. J. Cardiol. 2017, 33, 1543–1555. [Google Scholar] [CrossRef] [PubMed]
- Kielty, C.M.; Sherratt, M.J.; Shuttleworth, C.A. Elastic fibres. J. Cell Sci. 2002, 115, 2817–2828. [Google Scholar] [CrossRef] [PubMed]
- Ben-Sasson, A.; Carter, A.S.; Briggs-Gowan, M.J. Sensory over-responsivity in elementary school: Prevalence and social-emotional correlates. J. Abnorm. Child Psychol. 2009, 37, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Jussila, K.; Junttila, M.; Kielinen, M.; Ebeling, H.; Joskitt, L.; Moilanen, I.; Mattila, M.L. Sensory Abnormality and Quantitative Autism Traits in Children With and Without Autism Spectrum Disorder in an Epidemiological Population. J. Autism Dev. Disord. 2020, 50, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Gage, N.M.; Siegel, B.; Callen, M.; Roberts, T.P. Cortical sound processing in children with autism disorder: An MEG investigation. Neuroreport 2003, 14, 2047–2051. [Google Scholar] [CrossRef] [PubMed]
- Hitoglou, M.; Ververi, A.; Antoniadis, A.; Zafeiriou, D.I. Childhood autism and auditory system abnormalities. Pediatr. Neurol. 2010, 42, 309–314. [Google Scholar] [CrossRef]
- Guimarães-Souza, E.M.; Joselevitch, C.; Britto, L.R.G.; Chiavegatto, S. Retinal alterations in a pre-clinical model of an autism spectrum disorder. Mol. Autism 2019, 10, 19. [Google Scholar] [CrossRef]
- Lindly, O.J.; Chan, J.; Fenning, R.M.; Farmer, J.G.; Neumeyer, A.M.; Wang, P.; Swanson, M.; Parker, R.A.; Kuhlthau, K.A. Vision care among school-aged children with autism spectrum disorder in North America: Findings from the Autism Treatment Network Registry Call-Back Study. Autism 2021, 25, 840–853. [Google Scholar] [CrossRef]
- Longo, R.; Allegrini, F.; Gusson, E.; Morbio, R.; Di Gennaro, G.; Gozzi, L.A.; Marchini, G.; Zoccante, L. Visual-motor involvement in autism spectrum disorder: Could the stereopsis deficit affect motor coordination? Front. Psychiatry 2023, 14, 1130185. [Google Scholar] [CrossRef]
- Alrasheed, S.H.; Alghamdi, W. Systematic review and meta-analysis of the prevalence of myopia among school-age children in the Eastern Mediterranean Region. East. Mediterr. Health J. 2024, 30, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.P.; Chen, Y.L.; Hsiao, R.C.; Lai, Y.H.; Yen, C.F. Bidirectional associations between hyperopia, myopia, astigmatism, and strabismus, and attention-deficit/hyperactivity disorder in children: A national population-based cohort study. Braz. J. Psychiatry 2023, 45, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.R.; DeMand, A.; Lecavalier, L.; Smith, T.; Aman, M.; Foldes, E.; Scahill, L. Psychometric properties of the children’s sleep habits questionnaire in children with autism spectrum disorder. Sleep Med. 2016, 20, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, J.; Davitt, B.V.; Ultmann, M.; Maxim, R.; Cruz, O.A. Brief report: Incidence of ophthalmologic disorders in children with autism. J. Autism Dev. Disord. 2013, 43, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Asif, M.I.; Kalra, N.; Sharma, N.; Jain, N.; Sharma, M.; Sinha, R. Connective tissue disorders and eye: A review and recent updates. Indian J. Ophthalmol. 2023, 71, 2385–2398. [Google Scholar] [CrossRef]
- Sridhar, M.S. Anatomy of cornea and ocular surface. Indian J. Ophthalmol. 2018, 66, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Krey, K.F.; Hirsch, C. Frequency of orthodontic treatment in German children and adolescents: Influence of age, gender, and socio-economic status. Eur. J. Orthod. 2012, 34, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Rölling, S. Orthodontic treatment-service studied retrospectively in a group of Danish children aged 15–16 years. Community Dent. Oral Epidemiol. 1984, 12, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.M.; Hindin, J.S.; Mohatt, J.; Bauer, C.; Schild, J.; Falk, A.; Specht, M.; Woods, D.; Walkup, J. Proof of Concept Study of an Oral Orthotic in Reducing Tic Severity in Tourette Syndrome. Child Psychiatry Hum. Dev. 2022, 53, 953–963. [Google Scholar] [CrossRef] [PubMed]
- Murakami, J.; Tachibana, Y.; Akiyama, S.; Kato, T.; Taniguchi, A.; Nakajima, Y.; Shimoda, M.; Wake, H.; Kano, Y.; Takada, M.; et al. Oral splint ameliorates tic symptoms in patients with tourette syndrome. Mov. Disord. 2019, 34, 1577–1578. [Google Scholar] [CrossRef] [PubMed]
- Sandin, S.; Lichtenstein, P.; Kuja-Halkola, R.; Hultman, C.; Larsson, H.; Reichenberg, A. The Heritability of Autism Spectrum Disorder. JAMA 2017, 318, 1182–1184. [Google Scholar] [CrossRef]
- Arun, T.; Nalbantgil, D.; Sayinsu, K. Orthodontic treatment protocol of Ehlers-Danlos syndrome type VI. Angle Orthod. 2006, 76, 177–183. [Google Scholar]
- Csecs, J.L.L.; Iodice, V.; Rae, C.L.; Brooke, A.; Simmons, R.; Quadt, L.; Savage, G.K.; Dowell, N.G.; Prowse, F.; Themelis, K.; et al. Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. Front. Psychiatry 2021, 12, 786916. [Google Scholar] [CrossRef] [PubMed]
- Zoccante, L.; Zaffanello, M.; Di Gennaro, G. Editorial: The “Connectivome Theory”: Psyche, soma and the systemic involvement of connective tissue in neurodivergence. Front. Psychiatry 2024, 15, 1436796. [Google Scholar] [CrossRef] [PubMed]
- Damianidou, E.; Mouratidou, L.; Kyrousi, C. Research models of neurodevelopmental disorders: The right model in the right place. Front. Neurosci. 2022, 16, 1031075. [Google Scholar] [CrossRef] [PubMed]
- Hadders-Algra, M. Early Diagnostics and Early Intervention in Neurodevelopmental Disorders—Age-Dependent Challenges and Opportunities. J. Clin. Med. 2021, 10, 861. [Google Scholar] [CrossRef] [PubMed]
- Kushki, A.; Anagnostou, E.; Hammill, C.; Duez, P.; Brian, J.; Iaboni, A.; Schachar, R.; Crosbie, J.; Arnold, P.; Lerch, J.P. Examining overlap and homogeneity in ASD, ADHD, and OCD: A data-driven, diagnosis-agnostic approach. Transl. Psychiatry 2019, 9, 318. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.L.; Chen, L.H.; Lee, C.C.; Lai, K.Y.C.; Hung, S.F.; Tang, C.P.; Ho, T.P.; Shea, C.; Mo, F.; Mak, T.S.H.; et al. Genetic Overlap Between Attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in SHANK2 Gene. Front. Neurosci. 2021, 15, 649588. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
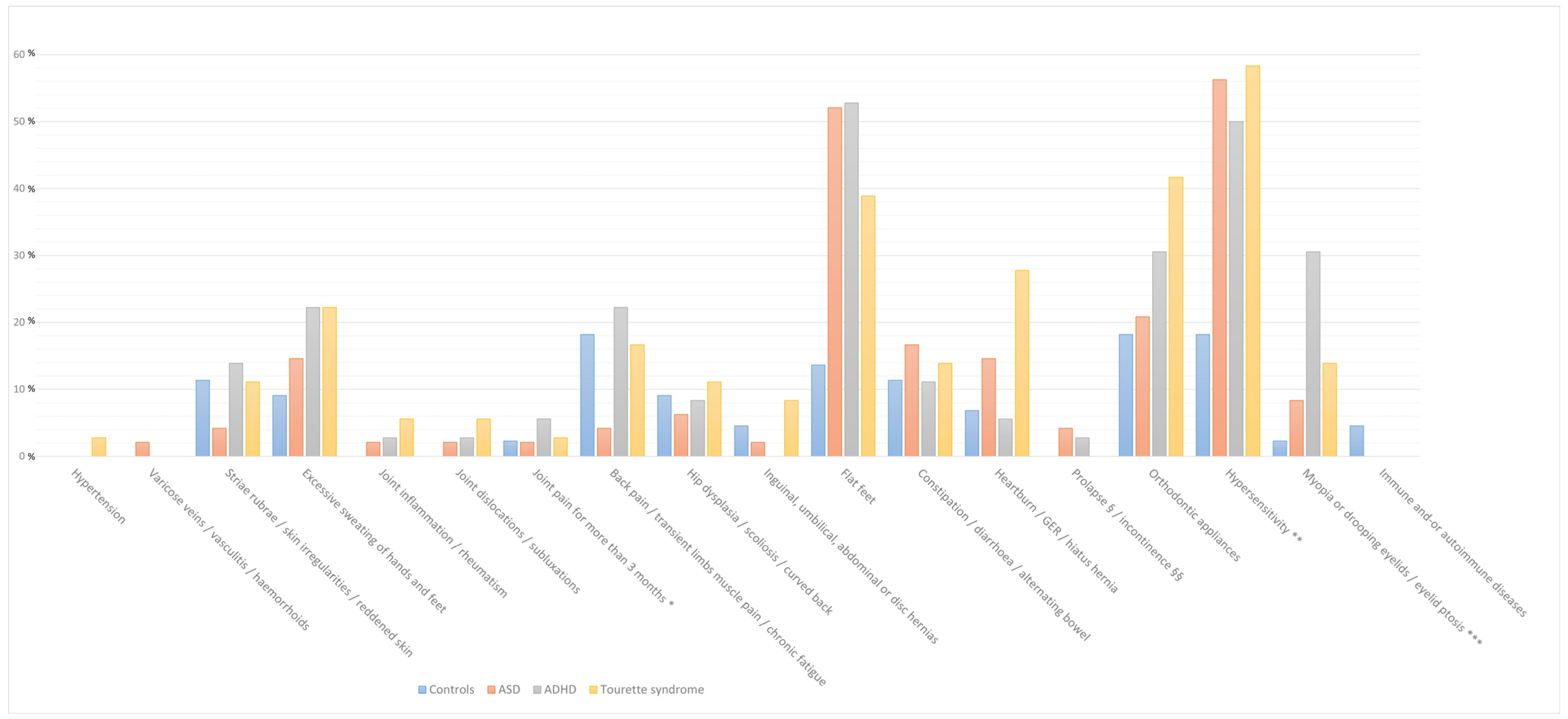
| Symptoms | ASD (%) | Δ% | ADHD (%) | Δ% | TS (%) | Δ% | Controls (%) |
|---|---|---|---|---|---|---|---|
| Hypertension | 0.0 | 0 | 0.0 | 0 | 2.8 | 2.8 | 0.0 |
| Varicose veins/vasculitis/haemorrhoids | 2.1 | 2.1 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Striae rubrae/skin irregularities/reddened skin | 4.2 | −7.2 | 13.9 | 2.5 | 11.1 | −0.3 | 11.4 |
| Excessive sweating of hands and feet | 14.6 | 5.5 | 22.2 | 13.1 | 22.2 | 13.1 | 9.1 |
| Joint inflammation/rheumatism | 2.1 | 2.1 | 2.8 | 2.8 | 5.6 | 5.6 | 0.0 |
| Joint dislocations/subluxations/dislocations | 2.1 | 2.1 | 2.8 | 2.8 | 5.6 | 5.6 | 0.0 |
| Joint pain involving 1 to 3 large joints lasting for more than 3 months | 2.1 | −0.2 | 5.6 | 3.3 | 2.8 | 0.5 | 2.3 |
| Back pain/transient muscle pain in the limbs/chronic fatigue | 4.2 | −14 | 22.2 | 4 | 16.7 | −1.5 | 18.2 |
| Hip dysplasia/scoliosis/curved back | 6.3 | −2.8 | 8.3 | −0.8 | 11.1 | 2 | 9.1 |
| Inguinal/umbilical, abdominal, or disc hernias | 2.1 | −2.4 | 0.0 | −4.5 | 8.3 | 3.8 | 4.5 |
| Flat feet | 52.1 | 38.5 | 52.8 | 39.2 | 38.9 | 25.3 | 13.6 |
| Constipation/diarrhoea/alternating bowel | 16.7 | 5.3 | 11.1 | −0.3 | 13.9 | 2.5 | 11.4 |
| Heartburn/gastroesophageal reflux/hiatal hernia | 14.6 | 7.8 | 5.6 | −1.2 | 27.8 | 21 | 6.8 |
| Rectal or uterine prolapse/urinary and/or faecal incontinence | 4.2 | 4.2 | 2.8 | 2.8 | 0.0 | 0 | 0.0 |
| Use of orthodontic appliances | 20.8 | 2.6 | 30.6 | 12.4 | 41.7 | 23.5 | 18.2 |
| Tactile/visual/auditory/olfactory or gustatory hypersensibility | 56.3 | 38.1 | 50.0 | 31.8 | 58.3 | 34.8 | 18.2 |
| Myopia or drooping eyelids/unilateral or bilateral eyelid ptosis | 8.3 | 6 | 30.6 | 28.3 | 13.9 | 11.6 | 2.3 |
| Immune and/or autoimmune diseases | 0.0 | −4.5 | 0.0 | 0 | 0.0 | 0 | 4.5 |
| Symptoms | ASD (OR, 95% CI) | p Value (ASD) | ADHD (OR, 95% CI) | p Value (ADHD) | TS (OR, 95% CI) | p Value (TS) |
|---|---|---|---|---|---|---|
| Hypertension | 2.19 (0.021–228.08) | 0.740 | 1.86 (0.011–306.46) | 0.812 | 4.90 (0.033–734.81) | 0.534 |
| Varicose veins/vasculitis/haemorrhoids | 3.58 (0.069–185.13) | 0.526 | 1.26 (0.011–143.97) | 0.924 | 1.09 (0.009–135.69) | 0.973 |
| Striae rubrae/skin irregularities/reddened skin | 0.34 (0.062–1.91) | 0.222 | 0.81 (0.188–3.45) | 0.771 | 0.52 (0.107–2.54) | 0.419 |
| Excessive sweating of hands and feet | 1.78 (0.451–7.01) | 0.411 | 2.12 (0.523–8.56) | 0.293 | 1.79 (0.422–7.62) | 0.429 |
| Joint inflammation/rheumatism | 2.61 (0.065–105.07) | 0.610 | 2.43 (0.059–99.60) | 0.639 | 3.40 (0.082–141.57) | 0.520 |
| Joint dislocations/subluxations | 2.79 (0.075–104.34) | 0.578 | 3.10 (0.071–134.14) | 0.557 | 4.82 (0.116–201.07) | 0.409 |
| Joint pain involving 1 to 3 large joints for more than 3 months | 1.14 (0.083–15.65) | 0.922 | 1.79 (0.151–21.20) | 0.645 | 0.90 (0.053–15.23) | 0.942 |
| Back pain/transient muscle pain in the limbs/chronic fatigue | 0.25 (0.053–1.16) | 0.076 | 1.21 (0.353–4.12) | 0.765 | 0.82 (0.211–3.15) | 0.769 |
| Hip dysplasia/scoliosis/curved back | 0.91 (0.170–4.92) | 0.915 | 0.84 (0.151–4.69) | 0.846 | 0.99 (0.176–5.55) | 0.988 |
| Inguinal, umbilical, abdominal or disc hernias | 0.55 (0.060–5.03) | 0.596 | 0.18 (0.007–4.70) | 0.306 | 1.21 (0.150–9.71) | 0.860 |
| Flat feet | 7.20 (2.438–21.23) | <0.001 | 6.73 (2.097–21.63) | 0.001 | 3.70 (1.107–12.34) | 0.034 |
| Constipation/diarrhoea/alternating bowel | 2.07 (0.579–7.44) | 0.263 | 1.45 (0.325–6.49) | 0.625 | 1.85 (0.414–8.28) | 0.421 |
| Heartburn/gastroesophageal reflux/hiatus hernia | 1.92 (0.460–7.98) | 0.372 | 0.63 (0.105–3.75) | 0.609 | 3.05 (0.697–13.37) | 0.138 |
| Rectal or uterine prolapse/urinary and/or faecal incontinence | 4.34 (0.144–131.51) | 0.399 | 2.58 (0.068–97.84) | 0.609 | 0.71 (0.009–56.36) | 0.880 |
| Use of orthodontic appliances | 2.02 (0.602–6.77) | 0.255 | 2.36 (0.650–8.57) | 0.192 | 3.20 (0.887–11.51) | 0.076 |
| Tactile, visual, auditory, olfactory or gustatory hypersensitivity | 5.90 (2.160–16.12) | 0.001 | 4.11 (1.385–12.19) | 0.011 | 5.35 (1.738–16.47) | 0.003 |
| Myopia or drooping eyelids/unilateral or bilateral eyelid ptosis | 3.18 (0.433–23.37) | 0.255 | 13.12 (1.859–92.56) | 0.010 | 5.01 (0.615–40.81) | 0.132 |
| Immune and/or autoimmune diseases | 0.38 (0.018–8.18) | 0.537 | 0.30 (0.010–9.11) | 0.488 | 0.38 (0.011–13.29) | 0.594 |
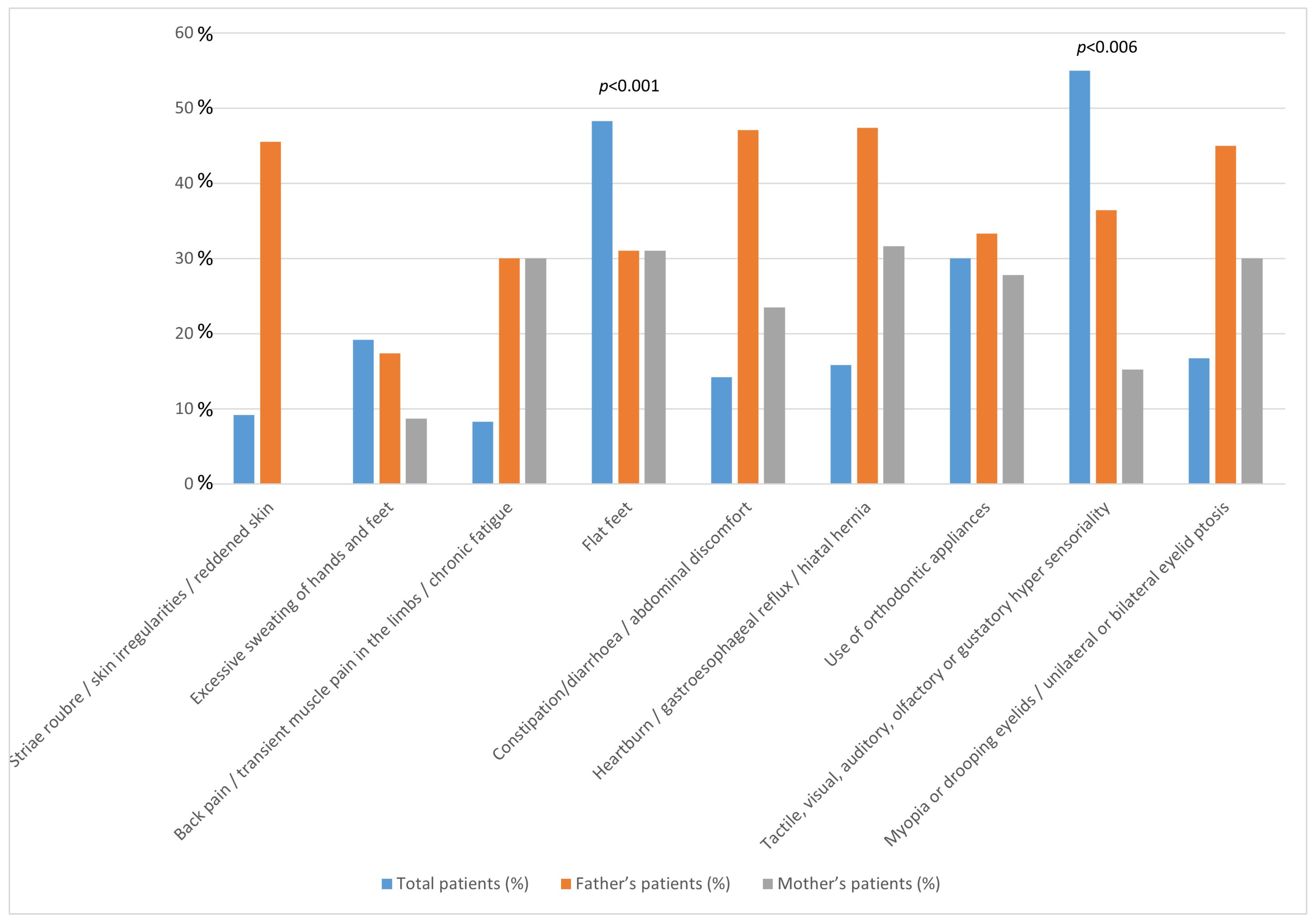
| Symptoms | Controls | Overall Patients (ASD + ADHD + TS) | Father’s Patients | Mother’s Patients | Statistical Analysis | |||
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | OR | p-Value | p-Overall | ||
| Totals | 44 | 120 | ||||||
| Striae rubrae/skin irregularities/reddened skin | absent | 39 (88.6) | 109 (90.8) | 15 (13.8) | 7 (6.4) | 2.44 | 0.206 | 0.330 |
| present | 55 (11.4) | 11 (9.2) | 5 (45.5) | 0 (0) | ||||
| Excessive sweating of hands and feet | absent | 40 (90.9) | 97 (80.8) | 11 (11.3) | 10 (10.3) | 1.49 | 0.480 | 0.299 |
| present | 4 (9.1) | 23 (19.2) | 4 (17.4) | 2 (8.7) | ||||
| Back pain/transient muscle pain in the limbs/chronic fatigue | absent | 36 (81.8) | 110 (91.7) | 21 (19.1) | 19 (17.3) | 2.08 | 0.283 | 0.862 |
| present | 8 (18.2) | 10 (8.3) | 3 (30.0) | 3 (30.0) | ||||
| Flat feet | absent | 38 (86.4) | 62 (51.7) | 5 (8.1) | 4 (4.5) | 8.3 | <0.001 | <0.001 |
| present | 6 (13.6) | 58 (48.3) | 18 (31.0) | 18 (31.0) | ||||
| Constipation/diarrhoea/abdominal discomfort | absent | 39 (88.6) | 103 (85.8) | 23 (22.3) | 8 (7.8) | 3.01 | 0.041 | 0.302 |
| present | 55 (11.4) | 17 (14.2) | 8 (47.1) | 4 (23.5) | ||||
| Heartburn/gastroesophageal reflux/hiatus hernia | absent | 41 (93.2) | 101 (84.2) | 33 (32.7) | 25 (24.8) | 1.68 | 0.344 | 0.389 |
| present | 3 (6.8) | 19 (15.8) | 9 (47.4) | 6 (31.6) | ||||
| Use of orthodontic appliances | absent | 36 (81.8) | 84 (70.0) | 23 (27.4) | 10 (11.9) | 1.48 | 0.372 | 0.109 |
| present | 8 (18.2) | 36 (30.0) | 12 (33.3) | 10 (27.8) | ||||
| Tactile, visual, auditory, olfactory or gustatory hypersensitivity | absent | 36 (81.8) | 54 (45.0) | 8 (14.8) | 3 (5.6) | 3.31 | 0.006 | <0.001 |
| present | 8 (18.2) | 66 (55.0) | 24 (36.4) | 10 (15.2) | ||||
| Myopia or drooping eyelids/unilateral or bilateral eyelid ptosis | absent | 43 (97.7) | 100 (83.3) | 28 (28.0) | 26 (26.0) | 1.27 | 0.635 | 0.059 |
| present | 1 (2.3) | 20 (16.7) | 9 (45.0) | 6 (30.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zoccante, L.; Di Gennaro, G.; Rigotti, E.; Ciceri, M.L.; Sbarbati, A.; Zaffanello, M. Neurodevelopmental Disorders and Connective Tissue-Related Symptoms: An Exploratory Case-Control Study in Children. Children 2025, 12, 33. https://doi.org/10.3390/children12010033
Zoccante L, Di Gennaro G, Rigotti E, Ciceri ML, Sbarbati A, Zaffanello M. Neurodevelopmental Disorders and Connective Tissue-Related Symptoms: An Exploratory Case-Control Study in Children. Children. 2025; 12(1):33. https://doi.org/10.3390/children12010033
Chicago/Turabian StyleZoccante, Leonardo, Gianfranco Di Gennaro, Erika Rigotti, Marco Luigi Ciceri, Andrea Sbarbati, and Marco Zaffanello. 2025. "Neurodevelopmental Disorders and Connective Tissue-Related Symptoms: An Exploratory Case-Control Study in Children" Children 12, no. 1: 33. https://doi.org/10.3390/children12010033
APA StyleZoccante, L., Di Gennaro, G., Rigotti, E., Ciceri, M. L., Sbarbati, A., & Zaffanello, M. (2025). Neurodevelopmental Disorders and Connective Tissue-Related Symptoms: An Exploratory Case-Control Study in Children. Children, 12(1), 33. https://doi.org/10.3390/children12010033