
Investigating the Association between Nutrient Intake and Food Insecurity among Children and Adolescents in Palestine Using Machine Learning Techniques

 ,
,  , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Variables
2.3. Nutrient Intake
2.4. Machine Learning Methods
3. Results
3.1. Descriptive Analysis
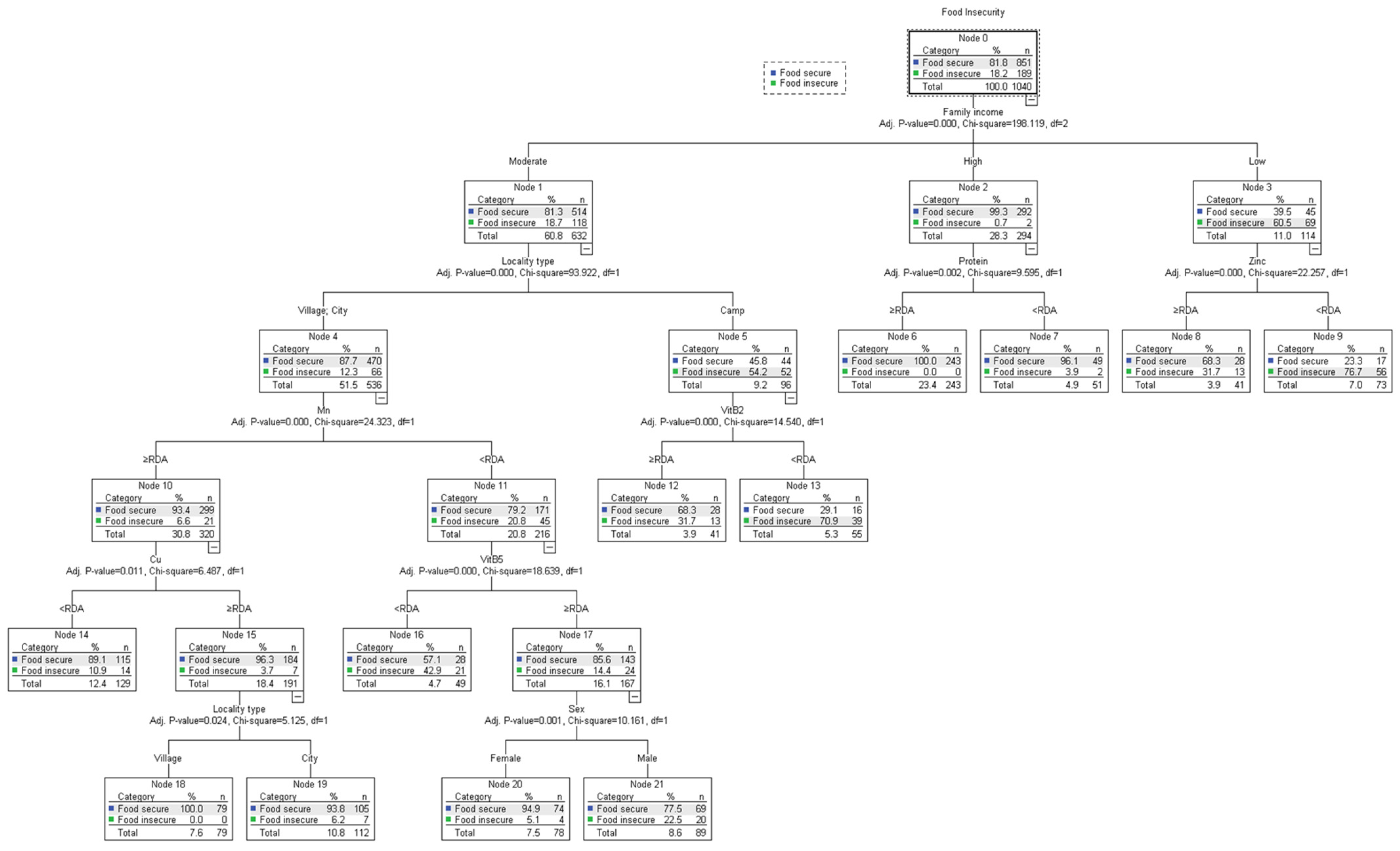
3.2. QUEST Model Analysis of Nutritional and Sociodemographic Variables
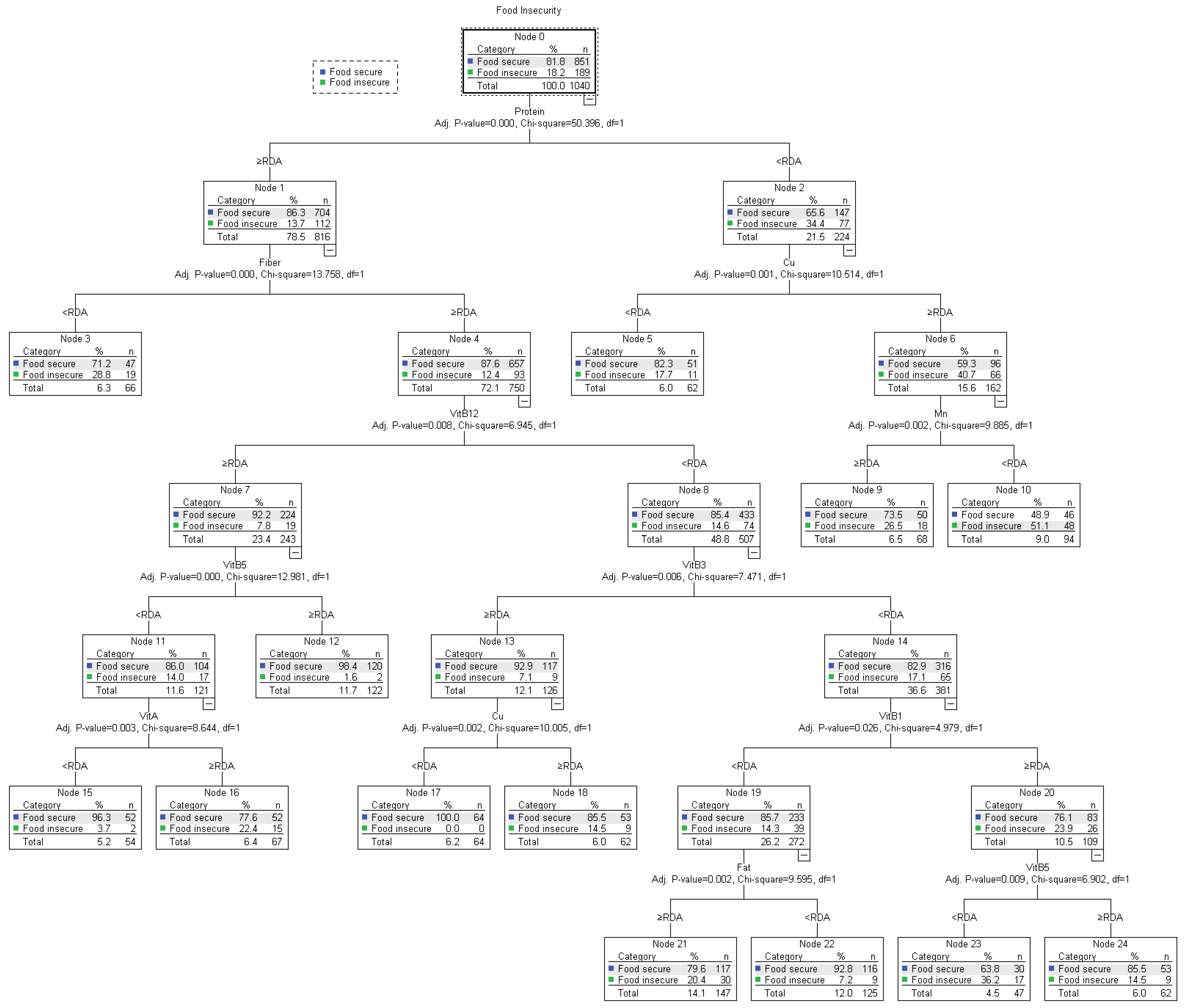
3.3. QUEST Model Analysis of Nutritional Variables
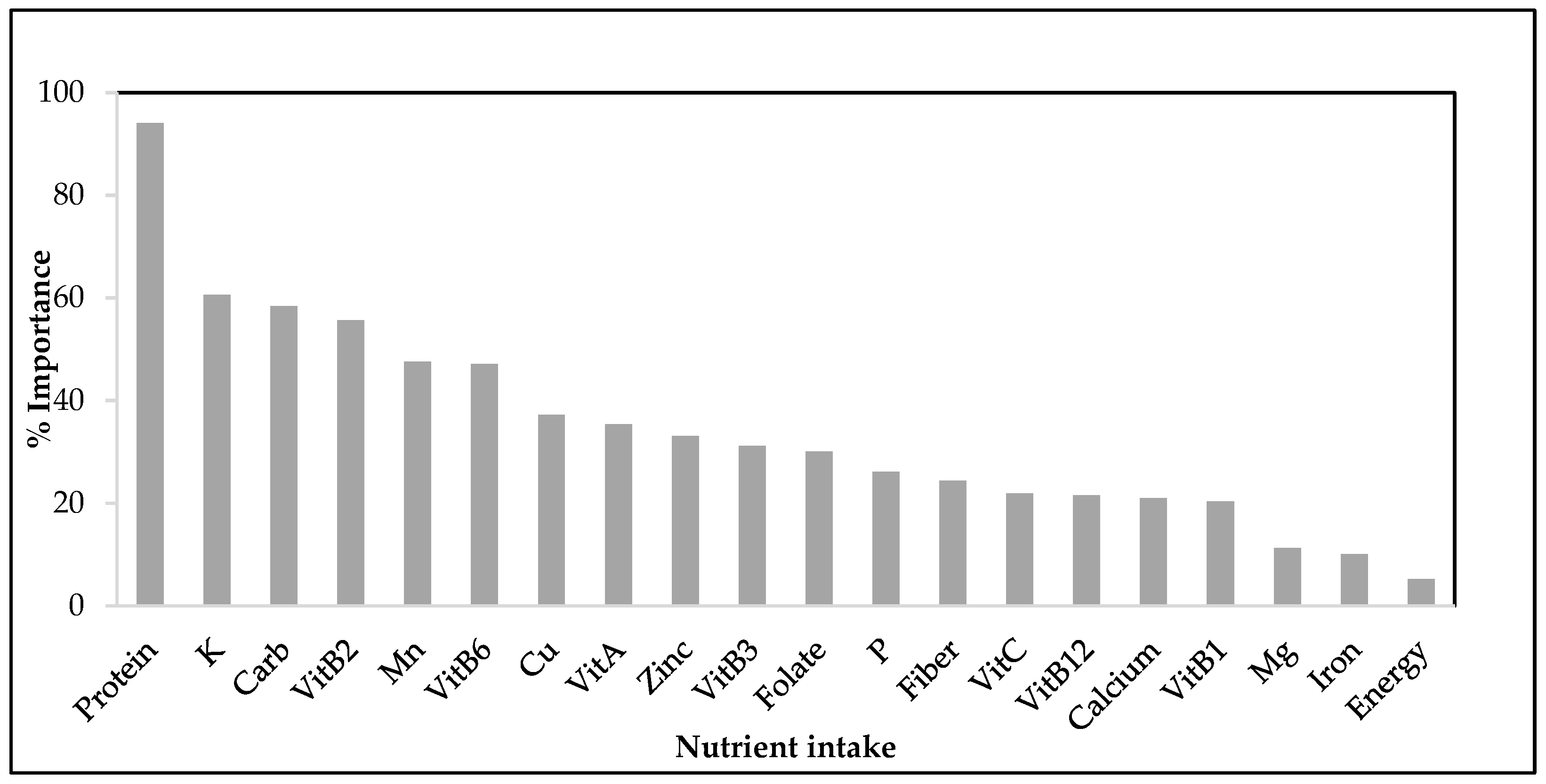
3.4. Gini Coefficient Importance Analysis
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2020. In Transforming Food Systems for Affordable Healthy Diets; FAO: Rome, Italy, 2020; 320p, Available online: https://www.fao.org/3/ca9692en/CA9692EN.pdf (accessed on 31 January 2023).
- Denney, J.T.; Brewer, M.; Kimbro, R.T. Food Insecurity in Households with Young Children: A Test of Contextual Congruence. Soc. Sci. Med. 2020, 263, 113275. [Google Scholar] [CrossRef] [PubMed]
- Morales, D.X.; Morales, S.A.; Beltran, T.F. Food Insecurity in Households with Children Amid the COVID-19 Pandemic: Evidence from the Household Pulse Survey. Soc. Curr. 2021, 8, 314–325. [Google Scholar] [CrossRef]
- Christian, V.J.; Miller, K.R.; Martindale, R.G. Food Insecurity, Malnutrition, and the Microbiome. Curr. Nutr. Rep. 2020, 9, 356–360. [Google Scholar] [PubMed]
- Pai, S.; Bahadur, K. The Impact of Food Insecurity on Child Health. Pediatr. Clin. N. Am. 2020, 67, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Sheikomar, O.B.; Wambogo, E.; Sahyoun, N.R.; Ghattas, H. Social Determinants of Food Insecurity in the Arab Region: A Comparative Study. FASEB J. 2017, 31, 729–791. [Google Scholar] [CrossRef]
- García-Chávez, C.G.; Rivera, J.A.; Monterrubio-Flores, E.; Rodríguez-Ramírez, S. Dietary Patterns Are Associated with Obesity in Mexican Schoolchildren. Eur. J. Clin. Nutr. 2020, 74, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Specter, S.E. Poverty and Obesity: The Role of Energy Density and Energy Costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Jomaa, L.; Naja, F.; Cheaib, R.; Hwalla, N. Household Food Insecurity Is Associated with a Higher Burden of Obesity and Risk of Dietary Inadequacies among Mothers in Beirut, Lebanon. BMC Public Health 2017, 17, 567. [Google Scholar] [CrossRef]
- Flores, H.L.; Amiri, A. CE: Addressing Food Insecurity in Vulnerable Populations. Am. J. Nurs. 2019, 119, 38–45. [Google Scholar] [CrossRef]
- Gupta, N.; Goel, K.; Shah, P.; Misra, A. Childhood Obesity in Developing Countries: Epidemiology, Determinants, and Prevention. Endocr. Rev. 2012, 33, 48–70. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, K.W.; Cho, M.S. Association of Food Insecurity with Nutrient Intake and Depression among Korean and Us Adults: Data from the 2014 Korea and the 2013–2014 Us National Health and Nutrition Examination Surveys. Int. J. Environ. Res. Public Health 2021, 18, 506. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.; Cowan, A.E.; Dodd, K.W.; Tooze, J.A.; Gahche, J.J.; Eicher-Miller, H.A.; Guenther, P.M.; Dwyer, J.T.; Potischman, N.; Bhadra, A.; et al. Association of Food Insecurity with Dietary Intakes and Nutritional Biomarkers among US Children, National Health and Nutrition Examination Survey (NHANES) 2011–2016. Am. J. Clin. Nutr. 2021, 114, 1059–1069. [Google Scholar] [CrossRef] [PubMed]
- Doreswamy, D.; Nigus, M. Feature Selection Methods for Household Food Insecurity Classification. In Proceedings of the 2020 International Conference on Computer Science, Engineering and Applications (ICCSEA), Gunupur, India, 13–14 March 2020. [Google Scholar] [CrossRef]
- de Araújo, M.L.; Mendonça, R.d.D.; Filho, J.D.L.; Lopes, A.C.S. Association between Food Insecurity and Food Intake. Nutrition 2018, 54, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Bercaw, H.; Reid, L.A.; Mendoza, J.A.; Frongillo, E.A.; Sauder, K.A.; Reboussin, B.A.; Mayer-Davis, E.J.; Dabelea, D.; Marcovina, S.M.; Mercado, C.; et al. Food Insecurity and Adequacy of Dietary Intake in Youth and Young Adults with Youth-Onset Type 1 and Type 2 Diabetes. J. Acad. Nutr. Diet. 2023, 123, 1162–1172. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H. Food Insecurity Is Associated with Dietary Consumption during the COVID-19 Pandemic: Data from the Korea National Health and Nutrition Examination Survey 2019–2020. Nutrients 2023, 15, 772. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.W.; Lo, Y.T.C.; Chen, Y.C.; Chen, W.C.; Huang, Y.C. Perceived Food Insecurity, Dietary Quality, and Unfavorable Food Intake among Children and Adolescents from Economically Disadvantaged Households. Nutrients 2021, 13, 3411. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Tarasuk, V. Food Insecurity Is Associated with Nutrient Inadequacies among Canadian Adults and Adolescents. J. Nutr. 2008, 138, 604–612. [Google Scholar] [CrossRef]
- Rodríguez, L.A.; Mundo-Rosas, V.; Méndez-Gómez-Humarán, I.; Pérez-Escamilla, R.; Shamah-Levy, T. Dietary Quality and Household Food Insecurity among Mexican Children and Adolescents. Matern. Child Nutr. 2017, 13, e12372. [Google Scholar] [CrossRef]
- Gu, X.; Tucker, K.L. Dietary Quality of the US Child and Adolescent Population: Trends from 1999 to 2012 and Associations with the Use of Federal Nutrition Assistance Programs. Am. J. Clin. Nutr. 2017, 105, 194–202. [Google Scholar] [CrossRef]
- Fram, M.S.; Ritchie, L.D.; Rosen, N.; Frongillo, E.A. Child Experience of Food Insecurity Is Associated with Child Diet and Physical Activity. J. Nutr. 2015, 145, 499–504. [Google Scholar] [CrossRef]
- Xu, R.; Blanchard, B.E.; McCaffrey, J.M.; Woolley, S.; Corso, L.M.L.; Duffy, V.B. Food Liking-Based Diet Quality Indexes (DQI) Generated by Conceptual and Machine Learning Explained Variability in Cardiometabolic Risk Factors in Young Adults. Nutrients 2020, 12, 882. [Google Scholar] [CrossRef] [PubMed]
- Troen, A.M.; Fraser, D.; Abdeen, Z.; Rosenberg, I.H. Child Nutrition Initiative in Israel and Palestine: Status of Food Security, Micronutrient Malnutrition, and Behavioral Change and Communication Programs. Food Nutr. Bull. 2006, 27, 180–185. [Google Scholar] [PubMed]
- Lin, T.K.; Kafri, R.; Hammoudeh, W.; Mitwalli, S.; Jamaluddine, Z.; Ghattas, H.; Giacaman, R.; Leone, T. Pathways to Food Insecurity in the Context of Conflict: The Case of the Occupied Palestinian Territory. Confl. Health 2022, 16, 38. [Google Scholar] [CrossRef]
- Ali Meerza, S.I.; Ahamed, A. Food Insecurity Through Machine Learning Lens: Identifying Vulnerable Households. In Proceedings of the 2021 Agricultural and Applied Economics Association Annual Meeting, Austin, TX, USA, 1 August 2021; pp. 1–11. [Google Scholar]
- Siy Van, V.T.; Antonio, V.A.; Siguin, C.P.; Gordoncillo, N.P.; Sescon, J.T.; Go, C.C.; Miro, E.P. Predicting Undernutrition among Elementary Schoolchildren in the Philippines Using Machine Learning Algorithms. Nutrition 2022, 96, 111571. [Google Scholar] [CrossRef] [PubMed]
- Harvey, J.; Perrat, B.; Harvey, J.; Morris, G.; Morris, G.; Nica-avram, G.; Harvey, J.; Smith, G.; Smith, A.; Goulding, J. Identifying Food Insecurity in Food Sharing Networks via Machine Learning Related Papers. J. Bus. Res. 2016, 2016, 469–484. [Google Scholar]
- Ferdowsy, F.; Alam Rahi, K.S.; Jabiullah, M.I.; Habib, M.T. A Machine Learning Approach for Obesity Risk Prediction. Curr. Res. Behav. Sci. 2021, 2, 100053. [Google Scholar] [CrossRef]
- Hu, G.; Ahmed, M.; L’Abbé, M.R. Natural Language Processing and Machine Learning Approaches for Food Categorization and Nutrition Quality Prediction Compared with Traditional Methods. Am. J. Clin. Nutr. 2023, 117, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Sood, S.; Singh, H. Computer Vision and Machine Learning Based Approaches for Food Security: A Review. Multimed. Tools Appl. 2021, 80, 27973–27999. [Google Scholar]
- Deléglise, H.; Interdonato, R.; Bégué, A.; Maître d’Hôtel, E.; Teisseire, M.; Roche, M. Food Security Prediction from Heterogeneous Data Combining Machine and Deep Learning Methods. Expert Syst. Appl. 2022, 190, 116189. [Google Scholar] [CrossRef]
- Gao, C.; Fei, C.J.; McCarl, B.A.; Leatham, D.J. Identifying Vulnerable Households Using Machine-Learning. Sustainability 2020, 12, 6002. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The Age of Adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Kendall, A.; Olson, C.M.; Frongillo, E.A.J. Validation of the Radimer/Cornell Measures of Hunger and Food Insecurity. J. Nutr. 1995, 125, 2793–2801. [Google Scholar] [PubMed]
- El Bilbeisi, A.H.; Al-Jawaldeh, A.; Albelbeisi, A.; Abuzerr, S.; Elmadfa, I.; Nasreddine, L. Households’ Food Insecurity and Its Association with Demographic and Socioeconomic Factors in Gaza Strip, Palestine: A Cross-Sectional Study. Ethiop. J. Health Sci. 2022, 32, 369–380. [Google Scholar] [PubMed]
- Huang, K.; Zhao, L.; Fang, H.; Yu, D.; Yang, Y.; Li, Z.; Mu, D.; Ju, L.; Li, S.; Cheng, X.; et al. A Preliminary Study on a Form of the 24-h Recall That Balances Survey Cost and Accuracy, Based on the NCI Method. Nutrients 2022, 14, 2740. [Google Scholar] [CrossRef]
- Cole, T.J.; Lobstein, T. Exploring an Algorithm to Harmonize International Obesity Task Force and World Health Organization Child Overweight and Obesity Prevalence Rates. Pediatr. Obes. 2022, 17, e12905. [Google Scholar] [CrossRef] [PubMed]
- National Research Council; Commission on Life Sciences; Food and Nutrition Board; Subcommittee on the Tenth Edition of the Recommended Dietary Allowance. Recommended Dietary Allowances, 10th ed.; National Academies Press: Washington, DC, USA, 1989; ISBN 0309536065.
- Song, Y.Y.; Lu, Y. Decision Tree Methods: Applications for Classification and Prediction. Shanghai Arch. Psychiatry 2015, 27, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Jiao, S.R.; Song, J.; Liu, B. A Review of Decision Tree Classification Algorithms for Continuous Variables. J. Phys. Conf. Ser. 2020, 1651, 012083. [Google Scholar] [CrossRef]
- Nembrini, S.; König, I.R.; Wright, M.N. The Revival of the Gini Importance? Bioinformatics 2018, 34, 3711–3718. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.D.; Floro, M.S. Food Insecurity, Gender, and International Migration in Low- and Middle-Income Countries. Food Policy 2020, 91, 101837. [Google Scholar] [CrossRef]
- Isanaka, S.; Mora-Plazas, M.; Lopez-Arana, S.; Baylin, A.; Villamor, E. Food Insecurity Is Highly Prevalent and Predicts Underweight but Not Overweight in Adults and School Children from Bogotá, Colombia. J. Nutr. 2007, 137, 2747–2755. [Google Scholar] [CrossRef]
- Eicher-Miller, H.A.; Zhao, Y. Evidence for the Age-Specific Relationship of Food Insecurity and Key Dietary Outcomes among US Children and Adolescents. Nutr. Res. Rev. 2018, 31, 98–113. [Google Scholar] [CrossRef] [PubMed]
- Hwalla, N.; Al Dhaheri, A.S.; Radwan, H.; Alfawaz, H.A.; Fouda, M.A.; Al-Daghri, N.M.; Zaghloul, S.; Blumberg, J.B. The Prevalence of Micronutrient Deficiencies and Inadequacies in the Middle East and Approaches to Interventions. Nutrients 2017, 9, 229. [Google Scholar] [CrossRef] [PubMed]
- Niles, M.; Bertmann, F.; Belarmino, E.; Wentworth, T.; Biehl, E.; Neff, R. The Early Food Insecurity Impacts of COVID-19. Nutrients 2020, 12, 2096. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Gerdes, M.W.; Martinez, S.G. Identification of Risk Factors Associated with Obesity and Overweight—A Machine Learning Overview. Sensors 2020, 20, 2734. [Google Scholar] [CrossRef] [PubMed]
- El Bilbeisi, A.H.; Al-Jawaldeh, A.; Albelbeisi, A.; Abuzerr, S.; Elmadfa, I.; Nasreddine, L. Association of Household Food Insecurity with Dietary Intakes and Nutrition-Related Knowledge, Attitudes, and Practices among Parents, Aged ≥ 18 Years in Gaza Strip, Palestine: A Descriptive Study. Heliyon 2022, 8, e09582. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The State of Food Security and Nutrition in the World 2018: Building Climate Resilience for Food Security and Nutrition; Food and Agriculture Organization: Rome, Italy, 2018. [Google Scholar]
- Arredondo, M.; Núñez, M.T. Iron and Copper Metabolism. Mol. Asp. Med. 2005, 26, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Ammerman, A.S.; Adair, L.S.; Aiello, A.E.; Flax, V.L.; Elliott, S.; Hardison-Moody, A.; Bowen, S.K. The Four Domain Food Insecurity Scale (4D-FIS): Development and Evaluation of a Complementary Food Insecurity Measure. Transl. Behav. Med. 2020, 10, 1255–1265. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Section | Items |
|---|---|
| Socioeconomic and Demographic Data | Gender, age, governorate, living area (south, middle, and north), locality (refugee camp, village, or city), education level, family size, father’s employment, mother’s employment, family income. |
| Household Food Insecurity | Food quantity, food quality, food acceptability, and the certainty of obtaining food. |
| Nutrition Status (Dietary Intake) | 24 h recall: grams intake, calories, protein, carbs, fiber, cholesterol, vitamin B1, vitamin B2, vitamin B3, vitamin B5, vitamin B6, choline, folate, vitamin B12, vitamin C, vitamin E, vitamin K1, calcium, chloride, magnesium, phosphorous, potassium, sodium, copper, fluoride, iron, manganese, zinc. |
| Nutrition Status (Anthropometric Measures) | Height, weight, mid-upper arm circumference, waist circumference, body mass index (BMI). |
| Nutrition-related Practices | Difficulty eating breakfast; difficulty eating three meals. |
| Variable | Overall Food Security | ||
|---|---|---|---|
| Food Security n (%) | Food Insecurity n (%) | F (p-Value) | |
| Total | 851 (81.8) | 189 (18.2) | |
| Gender | |||
| Male | 399 (78.5) | 109 (21.5) | 7.2 |
| Female | 452 (85) | 80 (15) | |
| Age (Year) | |||
| 5–8 | 263 (87.1) | 39 (12.9) | 4.0 * |
| 9–12 | 287 (79.3) | 75 (20.7) | |
| 13–18 | 301 (80.1) | 75 (19.9) | |
| Living Area | |||
| South | 339 (81.7) | 76 (18.3) | 0.290 |
| Middle | 279 (80.9) | 66 (19.1) | |
| North | 233 (83.2) | 47 (16.8) | |
| Locality | |||
| City | 464 (87.7) | 65 (12.3) | 68.1 ** |
| Village | 327 (85.4) | 56 (14.6) | |
| Camp | 60 (46.9) | 68 (53.1) | |
| Family Income | |||
| Low | 45 (39.5) | 69 (60.5) | 122.1 ** |
| Moderate | 514 (81.3) | 118 (18.7) | |
| High | 292 (99.3) | 2 (0.7) | |
| Family Size | |||
| 2–4 | 213 (81.9) | 47 (18.1) | 9.3 ** |
| 5–6 | 390 (86.9) | 59 (13.1) | |
| 7+ | 248 (74.9) | 83 (25.1) | |
| BMI | |||
| Underweight | 374 (81.3) | 86 (18.7) | 0.303 |
| Normal | 317 (81.3) | 73 (18.7) | |
| Overweight | 115 (83.9) | 22 (16.1) | |
| Obese | 45 (84.9) | 8 (15.1) | |
| Nutrient (Unit) | Nutrient Intake per RDA | Food Security Level | |||
|---|---|---|---|---|---|
| ≥RDA n (%) | <RDA n (%) | Food-Secure Mean ± SD | Food-Insecure Mean ± SD | F (p-Value) | |
| Energy (kcal) | 768 (73.8) | 272 (26.2) | 1584.4 ± 616.4 | 1465.8 ± 813 | 4.8 * |
| Protein (g) | 816 (78.5) | 224 (21.5) | 58.7 ± 27.3 | 52.7 ± 34 | 47.2 ** |
| Carb (g) | 842 (81) | 198 (19) | 216.1 ± 91.9 | 203.8 ± 115.7 | 8.3 * |
| Fat (g) | 517 (49.7) | 523 (50.3) | 55.7 ± 27.3 | 51.2 ± 30.7 | 7.6 * |
| Fiber (g) | 74 (7.1) | 966 (92.9) | 13.5 ± 7.8 | 13.8 ± 9.9 | 9 * |
| Folate (mg) | 760 (73.1) | 280 (26.9) | 177.5 ± 115.4 | 151.4 ± 121 | 9.4 * |
| Vit A (UI) | 745 (71.6) | 295 (28.4) | 134.2 ± 136 | 126 ± 125.2 | 12.3 ** |
| VitB1 (mg) | 312 (30) | 728 (70) | 1.4 ± 2.1 | 1.6 ± 2.4 | 1.8 |
| VitB2 (mg) | 529 (50.9) | 511 (49.1) | 2.6 ± 3.7 | 2.2 ± 4.8 | 19.3 ** |
| VitB3 (mg) | 276 (26.5) | 764 (73.5) | 9.7 ± 7.7 | 8.1 ± 7.3 | 9.8 * |
| VitB5 (mg) | 397 (38.2) | 643 (61.8) | 3.4 ± 2.1 | 3.3 ± 2.4 | 19.2 ** |
| VitB6 (mg) | 743 (71.4) | 297 (28.6) | 2.4 ± 3.8 | 2.4 ± 4 | 12.4 ** |
| VitB12 (mcg) | 288 (27.7) | 752 (72.3) | 2.3 ± 4.9 | 2.4 ± 5.5 | 5.7 * |
| Vit C (mg) | 225 (21.6) | 815 (78.4) | 60.7 ± 62.4 | 43.7 ± 52.1 | 6.4 * |
| Ca 1 (mg) | 31 (3) | 1009 (97) | 473 ± 289.5 | 401.4 ± 381 | 2.9 |
| Mg 2 (mg) | 201 (19.3) | 839 (80.7) | 155.6 ± 81.5 | 163.5 ± 122.9 | 1.2 * |
| Mn 3 (mg) | 636 (61.2) | 404 (38.8) | 2.1 ± 3.5 | 2.3 ± 3.7 | 16.7 ** |
| P 4 (mg) | 235 (22.6) | 805 (77.4) | 691.7 ± 333.8 | 670.6 ± 485.5 | 9.2 * |
| K 5 (mg) | 6 (0.6) | 1034 (99.4) | 1361.1 ± 673.2 | 1272 ± 908.2 | 27.8 ** |
| Cu 6 (mg) | 445 (42.8) | 595 (57.2) | 2.1 ± 2.8 | 2.1 ± 3.3 | 12.8 ** |
| Fe 7 (mg) | 383 (36.8) | 657 (63.2) | 9.6 ± 6 | 8.8 ± 5.7 | 3.3 |
| Zn 8 (mcg) | 354 (34) | 686 (66) | 7.2 ± 5.5 | 6.3 ± 5.4 | 12.0 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qasrawi, R.; Sgahir, S.; Nemer, M.; Halaikah, M.; Badrasawi, M.; Amro, M.; Vicuna Polo, S.; Abu Al-Halawa, D.; Mujahed, D.; Nasreddine, L.; et al. Investigating the Association between Nutrient Intake and Food Insecurity among Children and Adolescents in Palestine Using Machine Learning Techniques. Children 2024, 11, 625. https://doi.org/10.3390/children11060625
Qasrawi R, Sgahir S, Nemer M, Halaikah M, Badrasawi M, Amro M, Vicuna Polo S, Abu Al-Halawa D, Mujahed D, Nasreddine L, et al. Investigating the Association between Nutrient Intake and Food Insecurity among Children and Adolescents in Palestine Using Machine Learning Techniques. Children. 2024; 11(6):625. https://doi.org/10.3390/children11060625
Chicago/Turabian StyleQasrawi, Radwan, Sabri Sgahir, Maysaa Nemer, Mousa Halaikah, Manal Badrasawi, Malak Amro, Stephanny Vicuna Polo, Diala Abu Al-Halawa, Doa’a Mujahed, Lara Nasreddine, and et al. 2024. "Investigating the Association between Nutrient Intake and Food Insecurity among Children and Adolescents in Palestine Using Machine Learning Techniques" Children 11, no. 6: 625. https://doi.org/10.3390/children11060625
APA StyleQasrawi, R., Sgahir, S., Nemer, M., Halaikah, M., Badrasawi, M., Amro, M., Vicuna Polo, S., Abu Al-Halawa, D., Mujahed, D., Nasreddine, L., Elmadfa, I., Atari, S., & Al-Jawaldeh, A. (2024). Investigating the Association between Nutrient Intake and Food Insecurity among Children and Adolescents in Palestine Using Machine Learning Techniques. Children, 11(6), 625. https://doi.org/10.3390/children11060625